
Abstract
Introduction:
Recruiting organizations (i.e., health plans, health systems, or clinical practices) is important for implementation science, yet limited research explores effective strategies for engaging organizations in pragmatic studies. We explore the effort required to meet recruitment targets for a pragmatic implementation trial, characteristics of engaged and non-engaged clinical practices, and reasons health plans and rural clinical practices chose to participate.
Methods:
We explored recruitment activities and factors associated with organizational enrollment in SMARTER CRC, a randomized pragmatic trial to increase rates of CRC screening in rural populations. We sought to recruit 30 rural primary care practices within participating Medicaid health plans. We tracked recruitment outreach contacts, meeting content, and outcomes using tracking logs. Informed by the Consolidated Framework for Implementation Research, we analyzed interviews, surveys, and publicly available clinical practice data to identify facilitators of participation.
Results:
Overall recruitment activities spanned January 2020 to April 2021. Five of the 9 health plans approached agreed to participate (55%). Three of the health plans chose to operate centrally as 1 site based on network structure, resulting in 3 recruited health plan sites. Of the 101 identified practices, 76 met study eligibility criteria; 51% (n = 39) enrolled. Between recruitment and randomization, 1 practice was excluded, 5 withdrew, and 7 practices were collapsed into 3 sites for randomization purposes based on clinical practice structure, leaving 29 randomized sites. Successful recruitment required iterative outreach across time, with a range of 2 to 17 encounters per clinical practice. Facilitators to recruitment included multi-modal outreach, prior relationships, effective messaging, flexibility, and good timing.
Conclusion:
Recruiting health plans and rural clinical practices was complex and iterative. Leveraging existing relationships and allocating time and resources to engage clinical practices in pragmatic implementation research may facilitate more diverse representation in future trials and generalizability of research findings.
Keywords
Introduction
Pragmatic trials are an important component of implementation science, yet not much is known about the effort required to recruit a representative sample of organizations into studies. 1 A recent report identified the need to increase representation of diverse populations in research as “urgent” with wide ranging health implications. 2 In particular, rural populations are historically underrepresented in cancer research. Only about 3% of National Institutes of Health (NIH)-funded cancer research is conducted in rural communities, yet 14% to 19% of the US population lives in rural areas and 1 in 4 Medicaid patients aged 65 years and older is served by a rural clinical practice.3 -6
NIH investment in rural-focused cancer control research may bridge these funding disparities, 6 but only if research teams have effective strategies to recruit rural clinical practices and community organizations. Research has shown some facilitators and barriers to engaging clinical practices in pragmatic trials,7 -12 but less about how much effort it takes to effectively recruit organizations (i.e., health plans or health systems) into this research.1,13,14 Given the growing focus on engagement of community-based primary care practices in research by the NIH, additional insight into these processes is critical. 15
To address this gap, this manuscript reports on recruitment into SMARTER CRC, a pragmatic clinical trial to increase colorectal cancer (CRC) screening for Medicaid patients served by rural clinical practices (i.e., clinical practices). 16 Building on prior evidence that recruitment is often more challenging than expected,12,17 our study team sought to quantify the effort required to recruit a representative sample of health plans and clinical practices. In addition, to empirically understand the key factors for successful trial recruitment, we analyzed why health plans and diverse clinical practices chose to participate in a complex interventional study. We hypothesized that to meet recruitment targets for successful randomization into the pragmatic trial, we would need to learn and address the motivations for research participation at more than 1 type of organization (i.e., clinical practices nested within health systems nested within health plans). Further, because of these complex relationships and other constraints (i.e., organizational resources, the pandemic), we hypothesized that recruitment might require more time than prior studies. We include the timeline and activities required for recruitment, characteristics of clinical practices, and reasons why rural health plans and clinical practices participated. We anticipate these findings can inform future efforts to engage rural health care organizations in cancer prevention trials and facilitate more diverse representation in research.
Methods
Study Setting
SMARTER CRC is a pragmatic trial to implement mailed fecal immunochemical testing (FIT) and patient navigation to follow-up colonoscopy. 18 It is a collaboration between the Oregon Rural Practice-based Research Network (ORPRN), 19 Kaiser Permanente Center for Health Research (KPCHR), health plans serving a Medicaid population (i.e., Medicaid health plans), and rural and frontier clinical practices. Building on existing community-academic partnerships,20 -28 the study used a collaborative health plan-clinical practice implementation model to overcome challenges in implementing mailed FIT programs in rural primary care settings.21,29 Between 2013 and 2019, CRC screening was an incentivized quality metric for Oregon Medicaid health plans, who received annual performance-based payments for reaching CRC screening targets. 30 Study activities were approved by the Oregon Health & Science University Institutional Review Board (STUDY00020681), with a ceding agreement with KPCHR.
Eligibility Criteria: Health Plans and Rural Clinical Practices
At the time of study initiation, 16 regionally based Medicaid health plans were operating in Oregon. Eleven of the 16 health plans met eligibility criteria defined as serving primary care practices located in rural areas defined by Rural-Urban Commuting Area (RUCA) 31 codes or the Oregon Office of Rural Health. 32 Rurality classifications were operationalized as RUCA codes 1 to 3 as metropolitan, RUCA codes 4 to 6 as micropolitan, RUCA codes 7 to 10 as rural areas, or rural area defined by the Oregon Office of Rural Health as “any geographic areas in Oregon ten or more miles from the centroid of a population center of 40,000 people or more.”31,32 The intervention relied on health plan insurance claims to identify the patient population eligible for CRC screening; this approach was intended to overcome data challenges in implementing population outreach interventions with rural clinical practices.33,34
We sought to recruit 30 clinical practices within participating health plans meeting the following criteria: (1) rurality as defined above using RUCA 31 or the Oregon Office of Rural Health definitions, 32 (2) more than 30 eligible Medicaid or dual-eligible Medicaid/Medicare patients, and (3) a claims-reported CRC screening rate less than 60% in 2019.
Recruitment and Outreach Protocol
Per the study design, we recruited Medicaid health plans and clinical practices clustered within health plans. Medicaid health plans were approached between January 2020 and April 2021. Although in person recruitment was anticipated, strategies were adapted to virtual engagement modalities to comply with COVID-19 mandates in 2020. Generally, the recruitment team made an initial contact via e-mail to a known contact with a quality improvement focused role (e.g., quality performance coach, quality improvement supervisor, director of quality) at various levels of the health plan to schedule a half-hour virtual or phone meeting with the research team (i.e., project manager and practice facilitator). Following initial contact the research team confirmed interest and obtained a Letter of Support (LOS) or Partnership Agreement Letter (PAL) to complete health plan recruitment.
Clinical practice recruitment occurred between January 2020 through April 2021. The study team developed an initial list of eligible practices in collaboration with each participating health plan. Recruitment outreach varied by lead recruiter, modality (e.g., email, phone, text), intensity, and prior engagement (e.g., “cold call” vs. leveraging existing relationships). In some cases, health plans assisted with practice-level outreach. Study team members conducted regular outreach with eligible clinical practices to answer questions, provide information, and collect LOS or PAL forms. Outreach targeted roles with decision-making authority (i.e., medical directors, quality managers and directors, and clinic managers), or population health champions who could reach decision-makers.
Data Collection and Qualitative Analysis
Here we describe recruited clinical practice and health plan characteristics, and qualitative findings on clinical practice participation. Data sources included research staff recruitment logs (including contact counts and encounter fieldnotes), semi-structured interviews and clinic intake surveys for recruited clinical practices, and publicly available data to identify federal designation and RUCA code for recruited and non-recruited clinics.
Recruitment contact logs
The study team tracked contacts in a recruitment log, including organization, recruitment status, CRC screening rates if known, organization affiliation, contact information, next steps, and contact attempt details. Fieldnotes were taken during recruitment meetings. For the purposes of analysis, 1 recruitment touch was counted as 1 email or text thread regarding the same topic, 1 phone call, or 1 virtual meeting. Descriptive analyses were conducted to summarize, describe, and explore activity patterns.
Two members of the study team (BB, EM) reviewed data from the recruitment contact logs and classified clinical practices into categories. Eligible clinical practices were classified as “Did Not Approach” if the research team did not reach out, “Unable to Engage” if they were non-responsive after several multi-modal outreach attempts, or “Halted” if the research team did not have direct leads for outreach (i.e., a known organizational contact). Clinical practices were categorized as “Declined” when they notified the study team they would not participate, and “Disengaged” when non-responsive after initial engagement. Clinical practices were “Recruited” if they signed a LOS or PAL.
Semi-structured interviews
Semi-structured qualitative interviews were conducted with 5 staff members from the 3 participating health plans and 58 staff members across 27 participating clinical practices at study baseline between January 2021 and June 2021. Purposive sampling was used to identify interviewees, and interviews occurred after recruitment and before intervention implementation. Interviews were recorded, professionally transcribed, and validated by a member of the research team. Interview transcripts were uploaded into ATLAS.ti (Version 9.0) for data management and analysis.
Qualitative data analysis was led by the study qualitative lead (EK) with support from 2 qualitative research assistants (EM, CL), and findings were reviewed with the broader research team. The analysis team used thematic analysis to classify emergent themes by reading and coding transcripts independently, meeting to discuss codes and identify emergent themes, and sharing back query report summaries. 35 Once all interviews were coded, analyzed, and summarized, the Consolidated Framework for Implementation Research (CFIR) 36 was used to categorize the reasons why health plans and clinical practices chose to participate. After quantitative data were summarized, we re-reviewed qualitative themes to inform final results on recruitment and pull representative case examples.
Results
Effort Required to Meet Study Recruitment Targets
Overall recruitment outreach was extended by 6 months due to external disruptions (e.g., COVID-19, wildfires, dissolved CRC incentive metric). Figure 1 displays the consort diagram related to study recruitment. Nine health plans were approached to participate in study activities. Ultimately, 5 health plans chose to participate and 3 regional divisions chose to operate centrally with 1 point-of contact (noted as collapsed), resulting in 3 recruited health plan sites. Four health plans declined to participate, each with distinct reasons. One was unable to obtain organizational buy-in, 1 was unable to commit due to the demands of COVID-19, 1 lacked the bandwidth, saying “we just don’t think we have the bandwidth nor the interest at the clinics to take on the project,” and 1 did not operate in a manner conducive to the health plan and clinic collaborative model and was therefore a mutual decision between the health plan and study team. Two health plans were not approached because they did not have the capacity to support the intervention at the time.

Health plan and clinical practice recruitment consort diagram.
A total of 101 clinical practices were identified, however 25 did not meet eligibility criteria (see Figure 1). Pilot clinical practices were excluded because they had already implemented the intervention. Seventy-six clinical practices were deemed eligible for the study and 58 were approached between January 2020 and April 2021. Ultimately, 51% (n = 39) clinical practices enrolled in the study and 49% (n = 37) did not enroll. However, upon obtaining additional practice eligibility data, practices needed to be collapsed or excluded altogether if they had too few patients or could only provide research data as a single site. Another 5 clinical practices withdrew from the study prior to randomization, resulting in the randomization of 29 sites.
Of recruited clinical practices (Table 1), most either did not have any federal designation (38%, n = 15) or were Rural Health Clinics (RHCs) (36%, n = 14). The majority of both recruited clinical practices (67%, n = 26) and non-recruited clinical practices (59%, n = 22) were micropolitan (i.e., had a RUCA code between 4 and 6). Of clinical practices that did not enroll, most (42%, n = 16) either did not have a federal designation or were RHCs (32%, n = 12). Notably, of both recruited and non-recruited practices, only 1 (3%) was designated as a Tribal Health Center; this practice enrolled in the study.
Characteristics for Recruited and Not Recruited Eligible Clinical Practices.

Percentages may not total 100% due to rounding. Rurality: Metropolitan, RUCA code 1 to 3; Micropolitan, RUCA code 4 to 6; Rural Area, RUCA code 7 to 10.
Clinical practice recruited within the 1 to 3 RUCA code met the Oregon Office of Rural Health definition of rural area.
Touches to clinical practice recruitment
The recruitment period for the 39 clinical practices extended 467 days (from January 17, 2020 through April 28, 2021) and included 177 total recruitment touches. Figure 2 provides a graphic representation of recruitment efforts (e.g., number of recruitment touches, modality, length of recruitment) for the 39 recruited clinical practices by health plan. Seventeen clinical practices were recruited individually (i.e., study staff communicated directly with the clinical practice) while the remaining 22 clinical practices were recruited in 9 groups (i.e., study staff communicated with a single point of contact about recruitment). The median number of recruitment touches for clinical practices recruited individually was 5 (range: 2-17). Clinical practices in groups often required more recruitment touches per point-of-contact (median: 7 touches, range: 3-10).

Recruitment Effort for Recruited Clinical Practices by Health Plan (N = 39).
Time to clinical practice recruitment
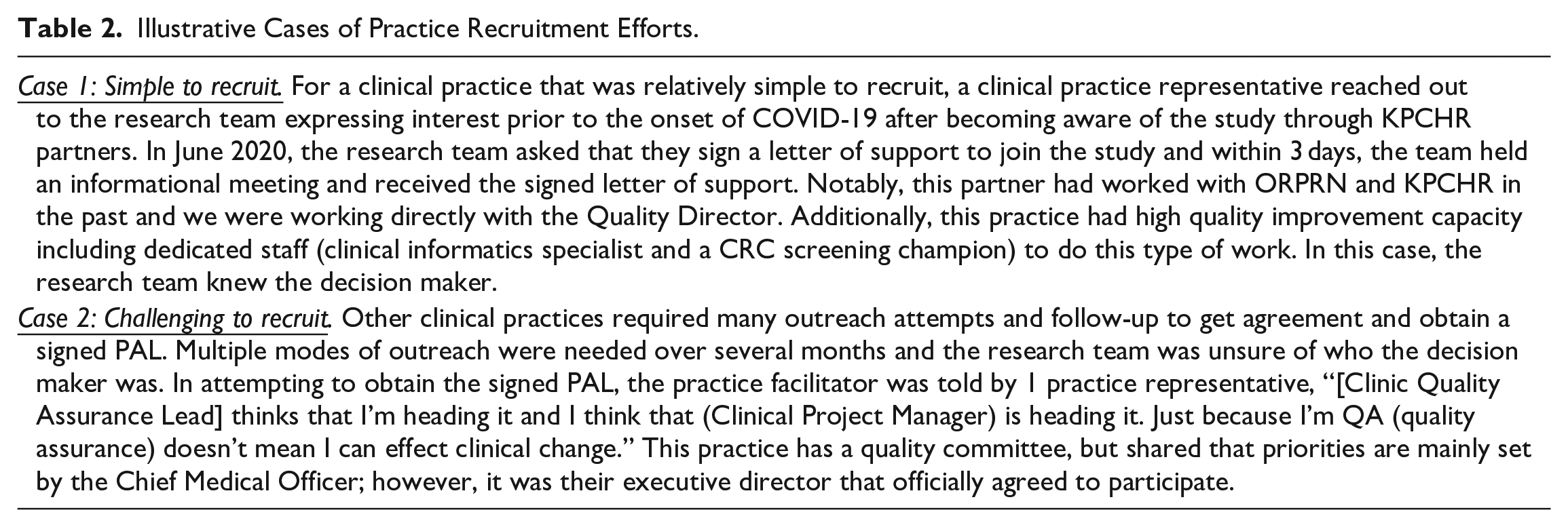
The time to recruitment differed for clinical practices recruited individually versus in groups. We also saw different lengths of time for “active recruitment,” defined as the initiation of outreach through a verbal agreement to participate, versus “full recruitment,” defined as the initiation of outreach through signed participation agreements (e.g., LOS or PAL). The active recruitment window among individual sites was a 69-day median, whereas group recruitment had a 134-day median—nearly twice as long. However, the full recruitment periods showed a smaller difference with a 190-day median for individual practices (range: 5-296 days) and a 209-day median for groups (range: 35-329 days). It was not uncommon to wait months to receive the PAL from a clinical practice after the last recruitment touch: for 7 individual sites and for 3 groups the PAL was submitted more than 3 months after the last recruitment touch. Additionally, groups sometimes submitted a single PAL for all participating sites and sometimes submitted individual PALs. We highlight 2 cases in Table 2 representing the range and complexity of the recruitment effort.
Illustrative Cases of Practice Recruitment Efforts.
Reasons for Participation
Table 3 summarizes health plan and clinical practice participation in relation to factors in the outer setting, inner setting, and intervention characteristics. Health plans and clinical practices often differed in their reported reasons for participating. However, for the outer setting, both health plans and clinical practices reported patient needs and resources as a reason for participation. Health plans and clinical practices did not report any of the same inner setting reasons for participation. Regarding intervention characteristics, both reported cost as a reason for participation.
Medicaid Health Plan and Rural Primary Care Clinical Practice Reasons for Participation Utilizing the Consolidated Framework for Implementation Research (CFIR).

CFIR Constructs in
Health plan motivations to participate also included the opportunity to network with similar organizations to improve screening rates (outer setting), the importance of organizational commitment to CRC screening (inner setting), and perceived value of the program (intervention characteristics). Each participating health plan had prior experience with mailed FIT programs and prior research or technical assistance experience with the study team. Clinical practice motivations also included the pressures of meeting preventive care needs as under-resourced rural clinical practices and quality metric reporting requirements (outer setting). Inner setting reasons included a prior relationship with the research team, improving access for patients, seeing value in the offered training, leadership enthusiasm, and the “COVID-19 proof” nature of the intervention (i.e., mailing FITs to patients’ homes could be accomplished during COVID-19 care interruptions).
Discussion
Our research suggests that recruiting rural clinical practices for pragmatic clinical trials requires flexibility to enable success. Due to the multi-level nature of the recruitment process (i.e., recruiting health plans prior to clinical practices), research team time was needed to identify which clinical practices identified by the health plans met recruitment eligibility criteria. Ultimately, 76 clinics were deemed eligible. Consistent with prior research, we found that it is important to build ample time for recruitment as clinical practices have competing priorities. 37 Many of the competing priorities were related to COVID-19, but not exclusively, and other factors routinely strain clinician and staff time. For example, prior research found that an additional 13 months was required to meet recruitment targets for an implementation study, even after a generously planned 27-month recruitment period. 12 This was consistent with our results, where a 9-month recruitment period was planned and ultimately 15 months was needed.
The process of recruiting health plans and clinical practices was complex and iterative. We incorporated known strategies to enhance recruitment, including building on prior relationships,7,8,12 multi-modal outreach methods (i.e., email, phone, and text), 7 remaining highly flexible,11,37 and using messaging that resonated with clinical practice needs. 12 Our findings support prior research emphasizing the perceived importance of the research topic, 11 an opportunity to improve patient care 13 and offering a streamlined intervention with limited burden on clinical practices. 37
While health plans and clinical practices chose to participate for different reasons, most had prior relationships and a commitment to CRC screening. Despite external disruptions (e.g., COVID-19 and wildfires), clinical practices appreciated the health plan-clinical practice partnered approach to reduce the administrative burden. Notably, even with CRC screening eliminated as a statewide incentivized quality metric, health plans and clinical practices described the importance of screening. Similar to prior research, 13 participating sites valued the support to improve screening.
CRC research in vulnerable populations is often focused on FQHCs,13,38 -40 and with only 23% of our enrolled clinics being FQHCs, our findings suggest the importance of including other practice types. This may be especially important for RHCs, as they’re historically underrepresented in research. 6 Additionally, only 3% (n = 1) of practices were designated Tribal Health Centers.
Our descriptive analysis provides a robust foundation for future research. Future studies could more systematically explore recruitment across heterogeneous rural environments, similarities and differences between rural and urban health plan and clinical practice recruitment, study team relationships with recruited and non-recruited organizations, characteristics of recruited and non-recruited organizations, the level of contact required (i.e., level of study team member conducting outreach to reach organizational decision makers), the relationship between a provider champion and recruitment outcomes, and cost analysis of recruitment. Notably, future studies could actively test comparative outreach strategies by controlling the modality of recruitment or recruitment lead.
Limitations
This study uses observational data to shed light into the complexities of clinical practice recruitment. However, there are a number of important limitations to inform future research. First, while we tracked recruitment activities for all clinical practices approached, we only have primary qualitative and quantitative data from health plans and clinical practices that chose to participate; we did not conduct interviews or surveys with sites that declined. Second, it is possible that not every recruitment interaction or point of contact was documented. While we anticipate any missed contacts did not occur systematically, this may have impacted our ability to quantify recruitment efforts and contribute to limitations due to wide variation and confounding variables not captured in our data. Third, we used publicly available data to identify federal designation and RUCA codes for non-recruited clinical practices after recruitment ended, thus it is possible there were changes in status from the time sites were approached during the recruitment period. Lastly, because this study focused on a rural health intervention, there is not an urban comparison.
Conclusion
Iterative and adaptable strategies were key to recruiting health plans and clinical practices into this pragmatic trial. The need to engage diverse sites into pragmatic research warrants additional research in this area and substantial investment. Our research identifies clinical practice and health plan motivators to participation and demonstrates the facilitators to multi-level, multi-tiered recruitment and the time and effort required to recruit a representative sample into the study.
Footnotes
Acknowledgements
The authors express their gratitude to Mary Patzel, MBA for leading qualitative data collection efforts; Erin Kenzie, PhD for leading qualitative data analysis; Caroline Lawrence for assisting in the analysis of qualitative data; Tiff Weekley, MA for assisting in the compilation of publicly available data for non-recruited clinical practices; and to health plan research partners for sharing information with their networks and providing data for research purposes. This study was conducted as part of the NCI-funded consortium The Accelerating Colorectal Cancer Screening and Follow-up through Implementation Science (ACCSIS) Program. The overall aim of ACCSIS is to conduct multi-site, coordinated, transdisciplinary research to evaluate, and improve colorectal cancer screening processes using implementation science strategies.
Abbreviations
Colorectal Cancer (CRC); Fecal Immunochemical Testing (FIT); Oregon Rural Practice-based Research (ORPRN); Kaiser Permanente Center for Health Research (KPCHR); Screening More Patients for CRC through Adapting and Refining Targeted Evidence-based Interventions in Rural settings (SMARTER CRC); Accelerating Colorectal Cancer Screening and Follow-up through Implementation Science (ACCSIS); National Institutes of Health (NIH).
Availability of Data and Materials
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: From 2021 to 2023, Dr. Coronado served as PI on a contract through the Center for Health Research funded by Guardant Health that assessed adherence to a commercially available blood test for colorectal cancer.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research reported in this publication was supported by the National Cancer Institute of the National Institutes of Health under Award Numbers UG3CA244298 and UH3CA244298. Dr. Davis’ time was supported in part by a career development award from the National Cancer Institute (1K07CA211971-01A1). Dr. Petrik’s time during manuscript preparation was supported by grant number K12HS026370 from the Agency for Healthcare Research and Quality. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health or Agency for Healthcare Research and Quality. The funders were not involved in the study design, collection, analysis, interpretation of data, the writing of this article or the decision to submit it for publication.
Ethical Approval and Consent to Participate
Study activities were approved by the Oregon Health & Science University Institutional Review Board (STUDY00020681) and was granted a waiver of informed consent, given minimal risks to patients.
Consent for Publication
All authors have received a final version of this manuscript and provide consent for its publication.
Trial Registration
Registered at clinicaltrial.gov (NCT04890054) and at the NCI’s Clinical Trials Reporting Program (CTRP #: NCI-2021-01032) on May 11, 2021.