
Abstract
Objectives:
Primary healthcare providers have an important role in helping people manage their reproductive health and fertility by assessing pregnancy intentions to inform the provision of contraception and/or preconception care. This study explores how women navigating fertility decisions perceived and experienced interactions with their healthcare providers around their fertility.
Methods:
We conducted in-depth interviews (N = 17) and focus groups (N = 17 groups) with 65 women aged 18 to 35 years about fertility, infertility, and reproductive planning. Two researchers coded 2 transcripts using thematic and inductive methods and met to develop a structured codebook. We then applied the codebook to the remaining transcripts.
Results:
In all interviews and focus groups, participants discussed their interactions with healthcare providers around fertility. Three central themes emerged in the data, including a desire for more information from healthcare providers about fertility; experiences of having fertility concerns dismissed by healthcare providers (eg, ability to become pregnant when desired); and, feelings that healthcare providers lacked sensitivity in discussing fertility related issues. Notably, these themes were present, even among participants who were not trying to become pregnant or who did not wish to become pregnant.
Conclusion:
Participants wanted information about fertility from their primary healthcare providers that they felt was lacking. Moreover, participants wanted their healthcare providers to engage with them as multifaceted individuals with current needs as well as future plans regarding fertility. While healthcare providers regularly assess pregnancy intentions, they may need to make a concerted effort to address fertility concerns among both those who want to pursue pregnancy and those who do not wish to become pregnant immediately.
Introduction
The reproductive justice framework outlines the rights of all people to have children, to not have children, and to parent children in safe and healthy environments.1,2 While there has been a shift among some healthcare providers and the organizations and institutions that help govern their practices toward embracing the reproductive justice framework, the priority for many has remained ensuring access to contraception and abortion.2,3
Primary healthcare providers, including both general practitioners and gynecologists, frequently focus on pregnancy prevention and preconception health when speaking with patients about issues related to their fertility. To that end, there are numerous guidelines available to healthcare providers to help assess patients’ need for contraception and for shared decision-making regarding choice of contraceptive method for those who do not wish to become pregnant. Contraceptive counseling protocols often begin with some variation of the question, ‘would you like to become pregnant in the next year?,’ 4 and most primary care and gynecological care organizations recommend routine screening of pregnancy intentions.5,6 For those who do not wish to become pregnant in the next year, counseling protocols guide the healthcare provider toward discussions of contraceptive methods. For those who want to become pregnant, counseling protocols transition to topics related to preconception health, including physical and mental health conditions and history, nutrition, genetics, environmental exposures, and other relevant topics.4,7 However, for many patients, a desire to become pregnant is not clear cut,8,9 and counseling protocols often lack guidance when it comes to addressing such nuances.
Positive patient-provider interactions are considered key drivers of treatment behavior and health outcomes,10,11 yet we know that patients are often dissatisfied with their provider interactions. 12 Existing research on patients’ experiences with healthcare tends to focus on evaluating specific healthcare visits rather than examining healthcare experiences and perceptions more broadly.13 -16 There is a dearth of research on perceptions of healthcare providers outside of clinical settings, which may be important in understanding how people experience and perceive their interactions with healthcare providers overall, rather than in specific encounters. The present study addresses this gap by focusing on healthcare experiences of a general population of people capable of pregnancy beyond singular clinical encounters.
Methods
We conducted 17 Focus Group Discussions (FGDs; n = 48 individuals) and 17 in-depth Interviews (IDIs) with a total of 65 participants aged 18 to 35 years from February-April 2022. Eligible participants lived in Ohio, identified as female, were not pregnant or sterilized, and had ever had sex with a male partner. We focused on individuals who were 18 to 35 years and who were not currently pregnant or sterilized to understand the perspectives of those who were most likely to be actively thinking about or making decisions around fertility, but who had not yet made an active decision to permanently prevent pregnancy or have a(nother) child. Participants were recruited using paid Facebook advertisements. FGDs and IDIs took place over Zoom and lasted approximately 1 h. All FGDs and IDIs were facilitated by researchers trained in qualitative data collection, recorded, and transcribed. We concluded data collection when we reached saturation of key themes, which we assessed through ongoing meetings with researchers and data collectors. 17 Participants provided consent via Qualtrics and were compensated for their time with a $40 gift card. This study met ethical standards and was approved by the Institutional Review Board at [blinded]. Prior to participating in a FGD or IDI, participants completed a brief questionnaire on sociodemographic characteristics.
We developed FGD and IDI guides focused on understanding participant’s experiences and perceptions around fertility and infertility, the messages they received about fertility, and sources of information. FGD guides were centered on social/community norms, while IDIs centered on personal experiences. However, personal experiences came up naturally in nearly all FGDs. Focus groups were intentionally small to ensure that they could be facilitated effectively virtually without extending beyond 1 h. Focus groups of 2 people specifically resulted from no-shows. In cases of no-shows, we continued with the FGD out of respect for participants’ time. If only 1 participant attended the focus group, we pivoted to conducting an in-depth interview with the permission of the participant. Example questions, and how they were asked in FGDs and IDIs, are included in Supplemental Appendix Table 1.
Transcripts were coded in Dedoose 18 using thematic and inductive methods to identify key themes. 19 Two team members independently coded 2 transcripts and then met to collaboratively develop a structured codebook. 19 The team members applied this codebook to a third transcript and met to reconcile differences and finalize the codebook before applying to all remaining transcripts.
Results
We conducted 17 IDIs and 17 FGDs with 65 participants. Discussions of interactions with primary healthcare providers, including both general practitioners and OBGYNs (obstetricians and gynecologists), were discussed in all FGDs and IDIs. Most participants were White (n = 45) or Black/African American (n = 10). Half were aged 30 to 35 years (n = 31; Table 1).
Participant Characteristics (N = 65).
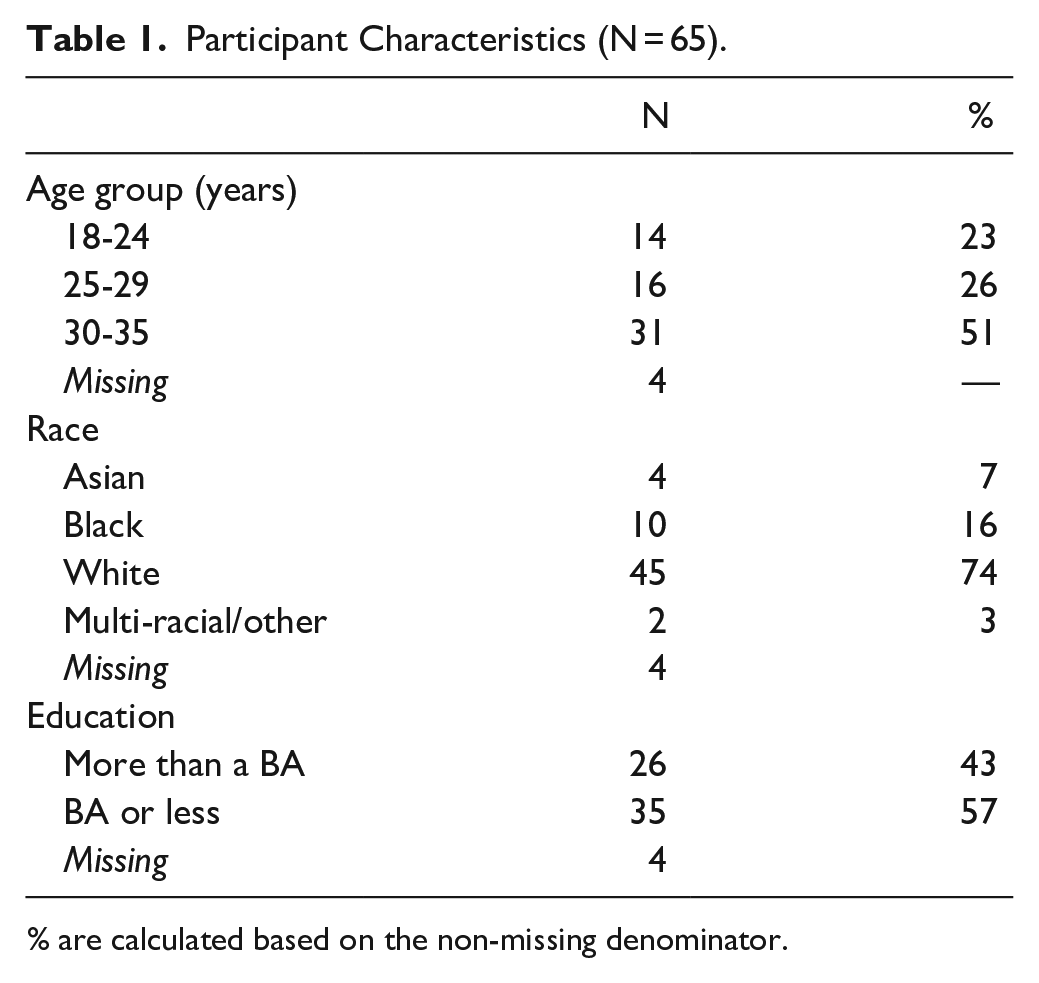
% are calculated based on the non-missing denominator.
Three central finding emerged: participants wanted more support and information from their healthcare providers about fertility and trying to become pregnant; participants often felt dismissed by providers when they had fertility concerns prior to trying to become pregnant; and, participants, particularly those with chronic health conditions, felt that their interactions with providers around fertility lacked sensitivity. A cross-cutting theme was the desire for individualized, accurate, and sensitively conveyed information from healthcare providers.
Trying to Become Pregnant
Many participants who wanted to become pregnant felt that they were not able to have conversations with their healthcare providers about trying to get pregnant. Many identified that there was not sufficient time to have these conversations in their limited interactions with providers. A FGD participant who had recently begun trying to become pregnant was frustrated that healthcare providers did not talk to their patients about getting pregnant on a routine basis. She said:
“Most people in my circle go to their OBGYN once a year. And I just wish these conversations were being had and I know they aren’t. None of my friends have ever been approached by a healthcare provider about their fertility [or] their plans to parent or not and that’s just so messed up, in my opinion.” -FGD_7, White, completed college
This participant went on to reflect on her experience, noting that she was “an educated person” but that she did not have the resources she needed when it came to trying to get pregnant. She wanted her healthcare provider to offer specific recommendations. She said:
“I’ve never had a conversation [about trying to get pregnant] with my OBGYN [. . .] She was just like, yeah, just have a lot of sex and if you want to track your cycle, you can. And that was it. And I was like, I know what that means [but] I don’t think most of my friends even know what tracking your cycle means. That’s crazy [. . .] providers don’t do a good job educating patients.” -FGD_7, White, completed college
Others echoed concerns that providers had little advice for those trying to become pregnant. Several participants wondered if they might be infertile, and nearly all wanted information about their fertility, but felt that they were expected to seek information outside of a healthcare setting. Participants who had questions about their fertility, but were not actively trying to become pregnant, felt that they had few options. One participant shared her experience looking for information:
“I’ve actually had to look into it and [did] a lot of research to even find anything [. . .] Doctors don’t even discuss that with [you]. Even if [you] are at that prime age, I feel like it can be really difficult to access resources that you need about your own fertility. I don’t really think there’s an easy way to learn this information [and] get that information from professionals.” -IDI_3, White, not completed college
This participant did “a lot of research” on her own, but felt that resources were lacking and wished that the information came from her healthcare provider directly. Most participants felt that a healthcare provider could only give them information about fertility if they tried to become pregnant for a year, but before that they were “on their own.” One participant described this process as reactive:
“I was researching pregnancy and stuff, it was [. . .] try for a year and then if you don’t get pregnant in a year, then go to your doctor and talk to them about it. And so, it’s like this set of rules [. . .] We’re not going to test you beforehand, we’re going to test you after [if] there’s a problem. So very reactive instead of proactive” -IDI_7, White, completed college
In some cases, participants shared positive experiences with providers who they felt offered trustworthy and tailored counseling around their individual circumstances and focused on education. One shared her experience when she decided she wanted to become pregnant:
“I talked to my doctor about taking out my birth control in order to get pregnant [. . .] she actually told me about going through [my] family history and doing genetic testing to see if there’s anything I should be concerned about [. . .] We’ve done the usual bloodwork, just to make sure that I was indeed [in] the perfect health state to have a child, to support a child. She’s kind of moved my medicines around in terms of my vitamins, having me take a prenatal now. She’s done a lot of education. And we’ll continue to have education about diet changes and alcohol and I’m sure a slew of other things.” -IDI_15, Woman of color (Asian/Asian American), completed college
Feeling Dismissed by Healthcare Providers
Participants who were not trying to become pregnant often felt that healthcare providers focused exclusively on their immediate goals of pregnancy prevention, dismissing concerns about their fertility more generally or about their ability to become pregnant in the future. This was particularly poignant among participants who had underlying medical conditions that they knew might impact their ability to become pregnant. A FGD participant shared a conversation she had with her doctor:
“I said to my doctor, ‘I’m just really worried that I’m not gonna be able to have a baby because of [polycystic ovarian syndrome (PCOS)] and like, that’s my biggest stress. And she was always like, ‘well, you don’t need to worry about that right now, it will be fine once it’s time, it’ll happen, there’s medicines we can give you and it’ll happen really quickly’ and blah, blah, blah. And I felt [she] kind of dismissed my concerns because in her mind I wasn’t in the age range that I should be getting pregnant at that time. I didn’t have a desire for pregnancy at that moment, so she just really dismissed it and never really acknowledged my concerns or acknowledged when I was asking what else I could be doing.” -FGD_10, White, completed college
One participant had a series of negative experiences with providers when she expressed concerns about infertility, which she attributed to her age and the fact that she did not currently want to become pregnant. She recently made an appointment with a new doctor and discussed her hope that she would be taken seriously:
“[I am] looking to really talk to them about my [family] history [and] my own personal health, and what that looks like for me in the future, to kind of decide what we should do. They could be like, ‘you’re worrying about nothing.’” -IDI_5, Woman of color (Black), not completed college
She emphasized how important having children was to her, although she was not yet ready to become pregnant:
“This is something that I really want to be prepared for and not be shocked later on when [. . .] I’m struggling to get pregnant or struggling to maintain a pregnancy.” -IDI_5, Woman of color (Black), not completed college
Another participant shared that several gynecologists told her she may have difficulty becoming pregnant, but that the conversation was dismissed because she was not currently trying to become pregnant. She talked about her anxiety over her future fertility and feeling that providers did not take her concerns seriously:
“I’ve had gynecologists in the past telling me like, ‘oh, this might be an issue.’ I think the most frustrating part is when I really start to ask more questions. I’ve been told this by like three different gynecologists [. . .] ‘we’ll deal with this when you want to start getting pregnant.’ [. . .] My anxiety can’t take this, I want to know what it is now and not wait until I’m ready to have kids and then have to go through this process!” -FGD_6, White, completed college
Some participants felt that providers did not listen to them when it came to their fertility desires. Participants who were in their 30s noted that they began to feel pressure from people in their lives, including some healthcare providers, to make decisions about fertility because of their age, even when they were not ready to do so. For example, 1 participant who was 34 years-old described an encounter with her doctor:
“The doctor looked at me last week [. . .] ‘how old are you?’ I said, 34. He said, ‘do you want children?’ And I said yes. And he looked at me like I was, you know, the look [. . .] the comment was, you might want to start looking into fertility doctors, things like that. And I was like, well, I’m not even in a relationship, I’m not dating right now, so it’s a non-issue. And he was like, you might want to look into that anyway.” -IDI_17, Woman of color (Black), completed college
In some FGDs, particularly with women of color, participants discussed how some people avoided healthcare providers because they anticipated that they might be dismissed or mistreated. For example, 1 participant noted that finding validation from a doctor regarding infertility was resource intensive and not always desirable. She said “not everyone has the ability to go see a specialist, or not everyone wants to even see a specialist. Maybe doctors scare them, or they just don’t like going to the doctor.” -FGD_2, Women of color, not completed college
Others were concerned that they would be ignored or invalidated if they asked questions about their fertility, although they had not experienced this themselves:
“People do go to their primary care appointments and ask questions. And some people, they have questions but don’t ask the doctor when they’re there [. . .] it’s fear of embarrassment or acting like they’re dumb or stupid for asking the question.” -FGD_16, Women of color, completed college
Lack of Sensitivity Around Fertility Related Information
Several participants had been told by healthcare providers that they may be infertile or at risk for infertility. In these cases, participants often felt that this information was not conveyed carefully or clearly, leading them to feel dismissed and confused. One participant shared her experience seeing an OBGYN at age 18 years. The participant spoke in a way that underscored her confusion about the interaction with her provider. She said her provider told her that she “had a condition similar to PCOS” and that her “uterus [was] facing the wrong way.” She was told that these conditions were both “playing against” her fertility, but that the doctor said, “we can’t really say for sure” and “you’ll find out when you find out.” In reflecting on that experience, this participant said:
“I think it’s a subject that [doctors] don’t know how to approach because they don’t know if it’s going to completely destroy someone’s life to hear that kind of news. I honestly feel like, looking back on it, it was less of my doctor’s way of saying she doesn’t know and more of her way of saying, like, don’t lose hope, if that’s something that you want. But either way, I was like, can you just tell me what to Google or give me a brochure or something so that I can get a little bit of information? That’s all I want.” -FGD_4, White, completed college
Many participants discussed medical conditions that they knew could impact their fertility. One participant described her experience with her gynecologist who told her she may have difficulty becoming pregnant or even be infertile after being diagnosed with PCOS. She emphasized that the way the information was conveyed to her was more harmful than the fact that she may not be able to become pregnant:
“When they told me [. . .] I was going to have trouble getting pregnant, I started sobbing [. . .] I was so, so upset [. . .] She made it seem like it was the end of the world that I maybe, potentially, may not have kids. And that is what scared me the most, is the way that [she] said it.” -IDI_1, White, not completed college
Another participant, also with PCOS, talked about learning from her gynecologist at age 21 years that she was “not technically infertile but getting pregnant naturally was [. . .] borderline impossible.” At the time she said she was happy (“when you are 21 it’s [. . .] the best thing someone could tell you”) but that when she later had a gap in her birth control and did not get pregnant (although she did not want to be pregnant at the time) she said “it kind of hit me like, holy shit, I might actually be infertile [. . .] I had to sit with it for a second.” -FGD_13, Women of color, completed college
A participant in her early 20s at the time shared an experience of her healthcare provider asking if she ever wanted to become pregnant in preparation for what she felt was an unrelated medical procedure. Of being asked about her future desire to get pregnant, she said:
“That’s a very big [question]. You know, I was [in my] early 20s. And no, I was not interested [in getting pregnant]. And now my perspective has shifted quite a bit. I wish there was more counseling [. . .] It was the first time I’d ever been asked about fertility, and I honestly was blown away that someone would ask me about that. I never dreamed that would be a question posed to me. And it was just offered so flippantly [. . .] I made the decision for the state that I was in at 21 years old, and now I’m concerned that maybe that is going to impact my fertility. So, I wish there’d been a little more support upfront [. . .] It is not a simple yes or no question.” -FGD_5, White, completed college
This participant wanted more consideration and support from her healthcare provider who asked, what she felt was, a deeply important and consequential question about her future fertility plans “flippantly.”
Discussion and Conclusion
People who are capable of pregnancy experience a meaningful gap between the contraceptive counseling and preconception care they are offered and their desire for information and engagement about their fertility and reproductive planning. In line with some previous studies, we found that participants felt that their interactions with healthcare providers did not fully meet their needs. 12 Our participants, many of whom did not wish to become pregnant, were still concerned about their fertility. Many wanted to have conversations with their primary care providers about trying to become pregnant, even when they did not want to become pregnant at that time and, in many cases, were using or wanted to be using contraception to actively prevent pregnancy. Participants felt that there was no space to have complex conversations within their brief and infrequent encounters with their providers. In some cases, participants felt that their concerns about fertility were actively dismissed. We know that most people will want to both prevent and pursue pregnancy at various stages in their lives, yet participants felt unable to engage in nuanced conversations about their fertility with their healthcare providers.
Counseling protocols, although useful, may inadvertently center conversations with patients on the question of whether or not they want to become pregnant. Although protocols are increasingly client-centered, recognize pregnancy ambivalence, and include questions to narrow in on patients’ needs,20-22 our participants indicated that their desire for information about fertility was not predicated on their desire to become pregnant in the near future. Counseling protocols are tools to help patients clarify their pregnancy intentions and make contraceptive decisions, but they are not designed to facilitate the types of conversations about fertility that our participants wanted, which often preceded pregnancy related decisions by months and years. Primarily, participants wanted to feel supported by their healthcare providers, not only in their current choices, but as people with complex lives and future plans. Healthcare providers should consider using, or continuing to use, evidence-based counseling protocols, while also providing individualized care and information to patients.
There is some evidence that reproductive life plan counseling may increase people’s knowledge of fertility related issues and preconception health, 23 but such protocols do not address desires for personalized information. In some cases, the information that participants wanted may have been beyond the scope of current medical guidelines or recommended practices (eg, fertility testing people who have not tried to become pregnant or those without recognized risk factors). The reality is that many people experience infertility of unknown cause, some of which may not be identifiable until one is trying to become pregnant. 24 Participants’ desire for certainty in this area of their life may not be compatible with current medical norms or technology, and we recommend that this deficit be acknowledged by healthcare providers as part of a person-centered approach to care. We recognize, and our participants recognized, that healthcare providers face many constraints in terms of time and resources, and the policies that govern them.
Participants craved accurate information about fertility, which they felt should come from healthcare providers. In many cases, participants did not push for the information that they wanted because the initial responses from their healthcare providers seemed to indicate that the provider felt the timing was not right to have a conversation about their fertility plans. Some of the frustration our participants expressed was related to limited or negative interactions with healthcare providers, but some was related to the dearth of information that they had about their fertility generally. It should be noted that the majority of our participants were White and many had college degrees, which are attributes that tend to contribute to general feelings of confidence in healthcare providers. Several participants of color noted avoiding interactions with healthcare providers. Indeed, we know that the quality of patient-provider interactions may vary based on race/ethnicity, which may contextualize our findings. 25 Our results may have been different with a more diverse participant population.26,27
We acknowledge that our participant pool was limited by choices in our recruitment strategy (eg, primarily recruiting using Facebook advertisements). A broader recruitment strategy may have yielded a more diverse participant pool. We also acknowledge that our inclusion criteria (eg, people capable of pregnancy, aged 18-35 years, etc.) excludes certain perspectives, which may be a valuable avenue of future research.
Ultimately, our participants wanted accurate information and engagement with their healthcare providers around fertility, whether or not they planned to become pregnant in the near future. Those who wanted to become pregnant acutely felt the gaps in their own knowledge and how these gaps went unaddressed by healthcare providers. Participants wanted their questions and concerns to be taken seriously and treated with care, something that most healthcare providers are also eager to convey. Providers could, and should, address some of our participants’ questions and concerns about fertility with information that they have from their training and understanding of the current medical literature. In cases where questions and concerns about fertility may be outside the scope of current technology, protocols, or norms, compassionate listening may go a long way in improving patient-provider interactions around fertility. Indeed, healthcare providers’ acknowledgement that their patients’ present and future selves and fertility—whether they were trying to prevent or pursue pregnancy—are of value is meaningful, even in the context of medical uncertainty.
Supplemental Material
sj-docx-1-jpc-10.1177_21501319241249405 – Supplemental material for Perceptions and Experiences With Healthcare Providers Among People Navigating Reproductive and Fertility Decisions
Supplemental material, sj-docx-1-jpc-10.1177_21501319241249405 for Perceptions and Experiences With Healthcare Providers Among People Navigating Reproductive and Fertility Decisions by Marta Bornstein, Anna C. Church, Kaleb Masterson and Alison H. Norris in Journal of Primary Care & Community Health
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Support for this project was provided by the Ohio State University Institute for Population Research through a grant from the Eunice Kennedy Shriver National Institute for Child Health and Human Development of the National Institutes of Health, P2CHD058484. The content is solely the responsibility of the authors and does not necessarily represent the official views of the Eunice Kennedy Shriver National Institute for Child Health and Human Development or the National Institutes of Health.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.