
Abstract
Introduction:
Sudanese American and other immigrant and refugee communities are at greater risk for exposure to COVID-19. This survey sought to better characterize COVID-19 vaccination practices, motivators, and drivers for hesitancy among Sudanese Americans.
Methods:
We developed an online, cross-sectional survey in English and Arabic distributed by Sudanese American community leaders in April 2022 with data stored anonymously in REDCap. Inclusion criteria were self-reporting being born within Sudan and living in the US within the last 2 years. Descriptive analysis tested survey responses for possible associations between the primary outcome, self-reported vaccination status, and questions regarding vaccination history, perspectives on vaccination, and demographic characteristics using Fishers Exact and Chi Squared Tests.
Results:
Of 111 survey responses received, 107 met inclusion criteria. 93% of respondents reported COVID-19 vaccine uptake with the primary motivation to protect oneself from disease. The most cited reason for vaccine hesitancy was belief it had not been studied enough. The group that reported vaccination had higher levels of education (.032) and were more likely to perceive that COVID-19 vaccinations were able to reduce spread (.001), decrease severe outcomes (.004), and benefits outweighing their risks (.004).
Discussion and Conclusions:
This survey population of Sudanese Americans demonstrated high levels of vaccine uptake (93%), far greater than either the corresponding US (78%) or Sudanese population (15%). It is likely that high levels of educational attainment moderated vaccine uptake, though our survey may not have had the power to fully evaluate vaccine hesitancy.
Introduction
The COVID-19 pandemic, due to Severe Acute Respiratory Syndrome Coronavirus 2 (COVID-19) demonstrated important principles of vaccine use, that both their efficacy and their practical limitations must be taken into account.1 -3 Equitable distribution has been a key issue for low-and-middle-income countries but vaccine hesitancy, defined as delay in acceptance or refusal of vaccination despite availability of vaccination services, has also been a global trend.4 -6 Several studies have documented decreasing confidence in other vaccines, commonly leading to parents’ decision not to vaccinate children.7,8 This places the world’s population at increasing risk from previous vaccine preventable disease. 9 The World Health Organization recognized vaccine hesitancy as one of the top 10 global health threats in 2019, and it played a definitive role during the COVID-19 pandemic and with administration of COVID-19 boosters. 6
Motives for vaccine hesitancy are multifactorial and efforts to address vaccine hesitancy should be tailored to specific populations. 4 Describing the motives of communities living within the US with a different country of origin—while acknowledging the contextual differences between immigrant, refugee, and migrant populations that affect health care utilization—could provide a unique window into both local and global health behaviors, including COVID-19 vaccine hesitancy. 10 While 1 survey reported that many refugees, especially those working in essential industries, intended to receive a COVID-19 vaccine, many of these communities faced higher levels of exposure to COVID-19 and barriers to care. There is little data in the US describing vaccine uptake among immigrant, refugee, or migrant populations.11,12
Our study chose to survey the Sudanese American population due to risk factors for exposure to COVID-19, prior evidence of lack of health education regarding infectious disease acquisition, and pre-existing relationships to their community among our team (FA and NA). 13 While studies have evaluated Sudanese perceptions of social distancing behaviors, this is the first project to our knowledge to characterize Sudanese American perspectives on the COVID-19 vaccine. 14 Our hypothesis was that Sudanese persons who have immigrated to America would demonstrate decreased levels of COVID-19 vaccination rates compared to the American public vaccination rates. Our primary objective was to examine rates of vaccination among Sudanese Americans. Our secondary objectives were to assess motivators for vaccine uptake and drivers for vaccine hesitancy in Sudanese Americans.
Methods
Participants and Sample Size
Inclusion criteria required participants be adults who are 19 years or older, originally from Sudan, and have lived in the US within the last 2 years before completing the survey. Community leaders in The Sudanese American Public Affairs Association, with participants from all over the US, and the Omaha Sudanese American Community Organization received an invitation to both participate in and distribute the survey in their Facebook and WhatsApp groups. This project’s sponsor is a member of both organizations. The survey was also made available to the New York Sudanese community, which has an estimated 1803 members. The message was then forwarded to other groups in a snowball sampling technique. Given this convenience sampling method, we are unable to track the exact number of people who received the survey.
Data Collection
We developed a culturally and linguistically tailored survey guided by principles from the Vaccine Examination Scale. 15 The survey (10 min in length) was presented in English and Arabic simultaneously with the assistance of Sudanese American health professionals from a variety of Sudanese cultural contexts. This helped to ensure appropriate cultural adaptation and we utilized back translation of the survey to confirm preservation of the survey’s meaning, (Supplemental Appendix 1). The first set of questions addressed the participants’ length of residence in the US. The rest of the survey consisted of 3 components: vaccination history along with detailed questions asking about drivers for vaccination, hesitancy, and barriers to uptake (7 questions); sources of information on the COVID-19 vaccine along with Likert Scale questions regarding participants’ perceptions of the COVID-19 vaccination (7 questions); and general demographic information (10 questions). The final question gave respondents the opportunity to be entered into a raffle for a $100 gift card.
Measures and Analysis
Data were collected in April 2022 and stored using REDCap electronic data capture tools without identifying information accessible to the investigators. Participants who did not meet inclusion criteria were excluded from the analysis. Fisher’s exact tests and Chi-squared test were used to evaluate possible associations between the primary outcome, vaccine uptake, and additional survey responses. Data analysis was conducted using STATA SE v17.0 (StataCorp, College Station, TX).
Ethics Statement
The Office of Regulatory Affairs reviewed and approved the IRB protocol for the purposes of this study on March 10, 2022. Consent was not obtained as the data were analyzed anonymously.
Results
Demographic Characteristics
Our sample consisted of 111 survey responses out of about 306 in our selected Sudanese American community groups. Four were excluded for failing to meet inclusion criteria [3 reported living outside the US, 1 did not respond], leaving 107 participants for analysis. Of these, 54% were between 30 and 49 years of age, 50% were females, and 70% spent most of their life in Khartoum while in Sudan (Table 1). Respondents currently live across 21 states and most (66%) have been in the US for 10 years or more. Eighty-six percent received education beyond high school and 48% received a post-graduate degree. Thirty-five percent reported working in healthcare either currently or at one point. Nearly 70% of our survey reported no chronic health conditions, though the prevalence of hypertension and diabetes was reported as 19% and 14%, respectively. About a third (31%) of respondents reported a positive COVID test and 72% knew at least one person who passed away due to COVID-19.
Respondent Demographic Characteristics by Reported Vaccination Status of Sudanese-Americans.
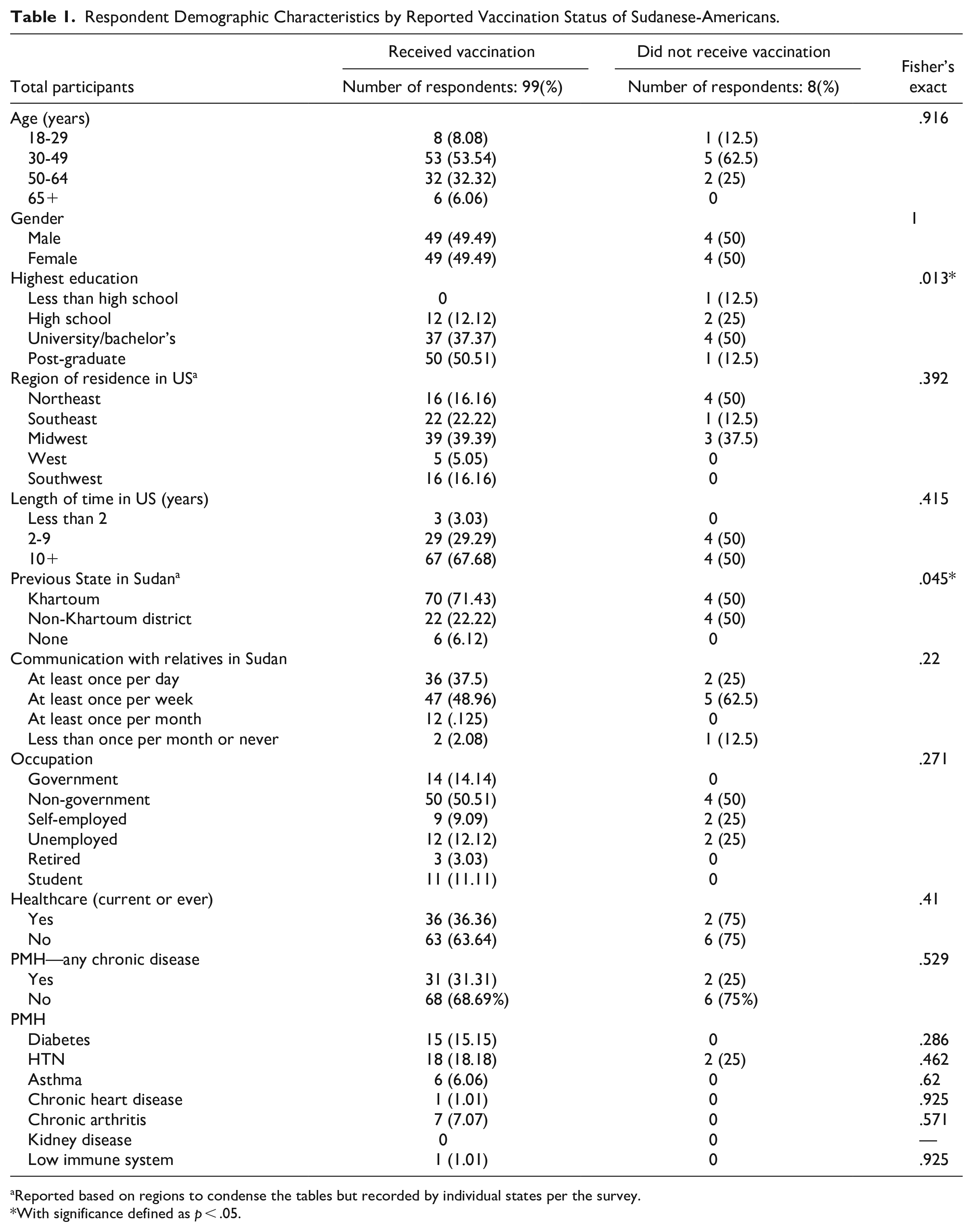
Reported based on regions to condense the tables but recorded by individual states per the survey.
With significance defined as p < .05.
Primary Outcome and Vaccination History
Our sample demonstrated 93% vaccine uptake with the primary motivation to protect oneself from disease (64%). Eight respondents had not been vaccinated with only “fear of side effects” reported as an existing barrier. Of the 6 unwilling to take the vaccine, the most cited reason (4 participants) was a belief that it had not been studied enough, with 2 participants citing harmful substances within the vaccine or lack of trust in the companies producing it, respectively. Of 14 possible hesitancy responses, 9 were selected at least once. Most (76%) reported interest in having their children vaccinated and 12% said they had never refused any vaccination (other than the COVID-19 vaccine).
Sources of Information
All but 1 respondent report utilizing social media. Whatsapp (93%) and Facebook (78%) were the most common platforms. When asked about their primary source of information on COVID-19, only 11% cited social media while the largest percentage (45%) used official government websites, followed by mass media (22%) and health personnel (11%).
Descriptive Analysis
Among demographic factors, vaccine uptake was positively associated with higher levels of education (.013) and prior state of residence in Khartoum (.045; Table 1). Responses to Likert scale questions regarding knowledge and attitude toward COVID-19 vaccination indicated an association between vaccine uptake and belief in COVID-19 vaccination’s ability to reduce spread (.001), decrease severe outcomes (.004), and the benefits outweighing the risks (.004) (Figure 1). When converted to a 5-point scale (5—Strongly Agree and 1—Strongly Disagree), the mean score for the vaccinated and unvaccinated groups among all questions is 4.47 and 3.51, respectively. No associations were found between vaccination status and a primary source of information on COVID-19 among all options, though there were strong trends to report official government websites among those vaccinated and social media among those unvaccinated (Table 2). When social media was considered against all other sources, however, those vaccinated were less likely to report it as a primary source of information (.005). Those vaccinated were also more likely to know someone who passed away due to COVID-19 (.038) and report anticipated vaccination of children (.038). Motivations for vaccine hesitancy could not be analyzed due to size constraints.

Scores based on responses to 5-point Likert Scale—Questions regarding COVID-19 vaccines [Blue: participants reporting vaccinated status (99) Orange: participants reporting unvaccinated status (8)].
Selected Participant Survey Responses by Self-reported Vaccination Status of Sudanese Americans.

Based on p-value < .05.
Discussion and Conclusions
Vaccine Uptake
Vaccine uptake among our survey population was much higher (92%) compared to the overall US (78%) or Sudanese population (15%) at the time of data collection. 16 This contradicts our initial hypothesis and suggests that barriers to care were not the primary deterrent to vaccine uptake among the convenience sample of Sudanese Americans surveyed. Instead, our findings suggest motivations for receiving the COVID-19 vaccine or additional protective factors were enough to overcome hesitancy or other barriers to care. Though protecting oneself from COVID-19 was clearly the primary motivator, our results corroborate previous studies that suggest a multifactorial model contributes to vaccine uptake. Unsurprisingly, one factor to consider among this population is education, given the large proportion that received post-graduate education. This corroborates previous studies linking education to increased vaccine uptake in Africa and likely moderates the differences in responses to Likert Scale questions regarding perceptions of the COVID-19 vaccine seen in Figure 1. 17 Though we did not complete this analysis, we would attribute this to increased health literacy and access to information regarding the risk and benefits of COVID-19 vaccination. Other contributors to vaccine uptake included residence in Khartoum state, which is where the capital city is located, while living in Sudan. Khartoum is largely urban with higher concentrations of tertiary health centers and resources compared to the rest of Sudan. This, along with the notable increase in vaccine uptake associated with family lost due to COVID-19 and willingness to vaccinate children, continue to support a multifactorial model for vaccine uptake that includes social determinants of health.
Vaccine Hesitancy
Given the high rate of vaccination and our small sample size, there was little opportunity to evaluate reasons for vaccine hesitancy and other barriers to vaccine uptake. Many drivers for vaccine hesitancy were selected by some of the participants, however, suggesting vaccine hesitancy is also multifactorial. Importantly, those reporting comorbidities associated with more severe outcomes were not more likely to receive vaccinations. The possibility exists that knowledge of the benefits of vaccines does not always translate to vaccine uptake, though our study may have been insufficiently powered to detect it.
Source of Information and Additional Influences
It is worth noting that the primary source of information on COVID-19 vaccines is influential in uptake. Though no specific social media platform showed a significant association with vaccine uptake, social media as a primary source of information compared to all other sources is associated with decreased COVID-19 vaccine uptake (see Table 2). This could be attributed to misinformation that, when not balanced by additional sources, begins to influence participant behavior. It suggests the need for government and official organizations to utilize these platforms when disseminating information on COVID-19 vaccines to both harness an effective tool and counteract misinformation present in these spaces. Finally, 23% of all respondents with children demonstrated hesitancy to vaccinating their children against COVID-19. While plans to vaccinate children are clearly associated with personal vaccine uptake, it is interesting that a cohort of respondents were vaccinated and still did not plan to vaccinate their own children (Table 2). These results (collected in May 2022) corroborate low levels of COVID-19 vaccine uptake in children, which remains below the national level. 16 This finding suggests COVID-19 vaccine uptake in adults does not always correlate with increased uptake in children. A systematic review of barriers to vaccine uptake in children identified similar factors—including education, confidence in vaccines, and social media use—to those identified in our study. 18 While our study was not designed to assess barriers to childhood vaccination, these similarities suggest that barriers are processed differently for children as opposed to oneself and more difficult to overcome.
Strengths and Limitations
Our study is the first to evaluate rates of vaccination and perceptions of the COVID-19 vaccine among Sudanese Americans. This helps to fill an important gap in literature among non-US born populations in the US. Moreover, this study was developed by a team made up largely of Sudanese Americans, which provides an important measure to ensure the cultural utility of the questionnaire. Finally, it was distributed by community groups which adds value in terms of describing the cultural and geographic context of the studied population, including pathways for dissemination of information.
Our study does have significant limitations. The primary weakness of our study is its current sample size, particularly for the unvaccinated group. This significantly limits the power and generalizability of our findings in conjunction with our second key limitation—convenience sampling methods. We utilized convenience sampling through online platforms (WhatsApp and Facebook) as they provided a quick, efficient, and culturally practical survey distribution method for this population. This sampling method inherently creates the potential for selection bias. As a result of these factors, our survey is not representative of and represents only a small percentage of the larger Sudanese community in the US. While additional efforts were made to reach a heterogeneous population through phone contact, there is a need for alternative community-engaged outreach methods. Next, one of the aims of the study was to describe motivations for vaccine hesitancy. This could not be completed due to these size constraints. We do, however, demonstrate that access to social media can influence COVID-19 vaccine uptake. Fourth, our findings should be interpreted in light of high health literacy among this population. This likely modifies the significant differences in responses to Likert Scale questions regarding risks and benefits of COVID-19 Vaccination between vaccinated and unvaccinated groups. Finally, this survey was susceptible to response and recall bias given respondents were asked to recall practices in the past regarding a highly politicized health topic. We attempted to mitigate this bias using anonymous responses. The data we were able to generate is primarily intended for descriptive use and must be interpreted in the context of these limitations.
New Contributions to the Literature and Applications
In the future, it would be important to determine whether there are additional groups within the Sudanese American community not being reached by the organizations we utilized to overcome the sampling bias we may have encountered. Further research should better characterize specific motivations for vaccine uptake, especially the level of knowledge of vaccination as both individual and public protection. This will be particularly important to improve uptake of COVID-19 boosters, which will likely be required annually to maintain adequate population-level protection against COVID-19. In addition, it would be useful to address hesitancy toward vaccinating children, as updated recommendations require multiple vaccines for children ages 6 months to 4 years (https://www.cdc.gov/coronavirus/2019-ncov/vaccines/stay-up-to-date.html). Finally, there is a need to better characterize the effect of engaging social media platforms to supply official information, especially to groups with barriers to healthcare access. This would be valuable to educate these populations about the risks of COVID-19 for those with comorbidities and to effectively distribute COVID-19 vaccine-specific information to populations that most need it.
Supplemental Material
sj-docx-1-jpc-10.1177_21501319241234868 – Supplemental material for Perceptions of the COVID-19 Vaccination Within a Convenience Sample of Sudanese Americans
Supplemental material, sj-docx-1-jpc-10.1177_21501319241234868 for Perceptions of the COVID-19 Vaccination Within a Convenience Sample of Sudanese Americans by Jonathan Freese, Fatima Abuzaid, Harlan Sayles, Mujtaba Abdellatif and Nada Fadul in Journal of Primary Care & Community Health
Footnotes
Acknowledgements
We would like to thank the Sudanese American Public Affairs Association and the Omaha Sudanese American Community Organization for their support in distributing this survey among the Sudanese American Community and all who participated in the survey. We would also like to thank Deanna Hansen for her administrative support and constant encouragement as well as the rest of the multidisciplinary team at the Specialty Care Center who provided their expertise and example in many ways.
Author Contributions
All authors contributed to the study conception and design. Material preparation and data collection were performed by Jonathan Freese, Fatima Abuzaid, Mujtaba Abdellatif, and Nada Fadul. Data analysis was performed by Harlan Sayles. The first draft of the manuscript was written by Jonathan Freese and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: JF received partial financial support from the Grants for Emerging Researcher/Clinician Mentorship (G.E.R.M.) Program award through the IDSA Foundation and the HIV Medicine Association (![]() ). The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
). The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Compliance With Ethical Standards/Consent
The Office of Regulatory Affairs at the University of Nebraska Medical Center reviewed and approved IRB # 0024-22-EX for the purposes of this study on March 10, 2022. Consent was not obtained as the data were analyzed anonymously.
Data
All data are fully available without restriction. All relevant data are within the manuscript and its Supporting Information files.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.