
Abstract
Introduction:
Missed visits have been estimated to cost the U.S. healthcare system $50 billion annually and have been linked to healthcare inefficiency, higher rates of emergency department visits, and worse outcomes. COVID-19 disrupted existing outpatient healthcare utilization patterns. In our study, we sought to examine the frequency of missed outpatient visits over the course of the COVID-19 pandemic and to examine patient-level characteristics associated with non-attendance.
Methods:
This study utilized data from a longitudinal cohort study (the Chicago COVID-19 Comorbidities (C3) study). C3 participants were enrollees in 1 of 4 active, “parent” studies; they were rapidly enrolled in C3 at the onset of the pandemic. Multiple waves of telephone-based interviews were conducted to collect experiences with the pandemic, as well as socio-demographic and health characteristics, health literacy, patient activation, and depressive and anxiety symptoms. For the current analysis, data from waves 3 to 8 (05/01/20-05/19/22) were analyzed. Participants included 845 English or Spanish-speaking adults with 1 or more chronic conditions.
Results:
The percentage of participants reporting missed visits due to COVID-19 across study waves ranged from 3.1 to 22.4%. Overall, there was a decline in missed visits over time. No participant sociodemographic or health characteristic was consistently associated with missed visits across the study waves. In bivariate and multivariate analysis, only patient-reported anxiety was significantly associated with missed visits across all study waves.
Conclusion:
Findings reveal that anxiety was consistently associated with missed visits during the COVID-19 pandemic, but not sociodemographic or health characteristics. Results can inform future public health initiatives to reduce absenteeism by considering patients’ emotional state during times of uncertainty.
Keywords
Introduction
Patient visit non-attendance, defined as scheduled medical appointments that are missed by patients with or without prior notification or cancellation, have been estimated to cost the U.S. healthcare system $50 billion annually and is a leading cause of healthcare inefficiency and reduced productivity. 1 While rates of non-attendance vary across health systems, a recent systematic review found that 15% to 30% of scheduled appointments among patients with chronic conditions are not attended; this rate can be as high as 50% in some primary care settings.2 -4 At the patient level, missed medical visits can delay diagnosis and/or intervention; among patients with chronic conditions and/or acute illness, it has been linked to higher rates of emergency department visits and hospitalizations and worse disease management and outcomes.5 -7
A large body of evidence suggests that appointment non-attendance is highest among minoritized patients, individuals of low socioeconomic status, patients who are younger, women, and adults with limited health literacy.8 -11 Prior research on the underlying causes of visit non-attendance indicates that common barriers include competing family/employment demands, forgetfulness, lack of transportation, low self-efficacy, miscommunication, and medical mistrust.3,9,11,12 As a result, initiatives to reduce missed visits have historically been aimed at implementing reminder systems, providing or facilitating transportation, and improving patient education and coordination of care.2,6,13
The COVID-19 outbreak rapidly changed the landscape of healthcare in the United States and disrupted existing outpatient healthcare utilization patterns. Concerns over COVID-19 transmission and uncertainty surrounding the pandemic resulted initially in high levels of visit non-attendance. 14 Little is known, however, about how visit non-attendance due to COVID-19 changed over the course of the pandemic and whether patient-level factors that were previously linked to missed visits remained predictive of non-attendance during this historic time. To address these research gaps, we used data from the Chicago COVID-19 and Comorbidities (C3) cohort study to track visit non-attendance due to COVID-19 from the onset of the pandemic through 2022 and to examine patient-level characteristics associated with missed visits. Our study focused specifically on middle aged and older adults with chronic conditions, a population with higher healthcare utilization that was also at increased risk of negative COVID-19 outcomes.15 -18
Methods
The study utilized data collected from the COVID-19 and Chronic Conditions (C3) study, which has been described in detail previously. 16 In brief, the C3 study was designed to follow a cohort of patients to examine the effects of the COVID-19 pandemic on individuals’ physical and mental health, health behaviors, and healthcare access. C3 began collecting data in the first weeks of the pandemic (March 13-20, 2020) and, to date, has included 8 waves of data collection. The analyses reported herein are from data collected in Wave 3 (05/01/20-05/22/20) through Wave 8 (02/17/22-05/19/22), during which data collection on our primary variable of interest for this study (canceling or missing a medical appointment) was collected. The Northwestern University Institutional Review Board (IRB) approved all study procedures.
Participants
C3 participants were active enrollees in 1 of 4 parent studies which have been described previously.16 -18 Inclusion criteria across parent studies varied. Some studies included participants of any age, while others focused on older adults exclusively. All studies included patients with 1 or more chronic conditions including type 2 diabetes, kidney transplant or older individuals taking 5 or more long-term medications. These patients were at higher risk of contracting COVID-19.16 -18 Exclusion criteria across all studies included participants with severe, uncorrectable, vision, hearing, and/or cognitive impairments that would preclude study consent and/or participation; 1 study enrolled English and Spanish-speakers while the others recruited only English speakers. 16
Data Collection Procedures
At each study wave, trained research assistants contacted eligible participants via telephone, invited them to participate in the C3 survey, and obtained verbal consent. They then administered a 30 to 40 min structured survey to participants via phone; responses were recorded using the REDCap software. Participants were compensated with a $15 gift card.
Measures
Patient demographics and socioeconomic status were originally collected as part of the parent studies. Participants self-reported sociodemographic attributes (ie, age, sex, race, income, and insurance status) and health characteristics (ie, number of chronic conditions and self-reported health status). Participants’ health literacy was assessed through the Newest Vital Sign (NVS) and patient activation was measured through the Consumer Health Activation Index (CHAI).16,18,19 Depressive and anxiety symptoms were measured through validated Patient Reported Outcomes Measurement Information Service (PROMIS) short-form instruments in Waves 3 through 8, with higher scores indicating worse symptoms. 20 The primary outcome for these analyses was missed healthcare appointments due to COVID-19, which was measured asking a single question “Did you choose to miss or cancel any medical appointments because you were too worried about getting the coronavirus?” (Responses: “Yes” or “No.”)
Analysis
Frequencies with percentages and means with standard deviations were used to describe the sample. For bivariate analyses, chi-square tests and t-tests were used to assess the association between patient characteristics and missing or canceling medical appointments. Multivariate logistic regression models were performed for each wave, to predict our main outcome, controlling for potential confounders, such as age, sex, race and depression and anxiety levels. Odds ratios and 95% confidence intervals were estimated.
Results
A total of 845 participants who had completed at least 1 wave of the C3 study were included in analyses. Response rates from Wave 3 (05/01/20-05/22/20) through Wave 8 (02/17/2022-05/19/2022) were high (range 95.5%-98.8%). Participants were racially diverse and on average were 65 years old. The majority (63.3%) were female and over half (58.1%) had 3 or more chronic conditions. Over half (52.8%) of participants reported a college degree or higher level of education and 22.6% had limited health literacy. Approximately half (50.4%) of participants had low levels of patient activation. Table 1 displays the study sample characteristics.
Sample Characteristics. f

10 missing race data.
8 missing poverty data.
43 missing literacy data.
44 missing activation data.
1 missing insurance data.
Figures are frequencies and percentages, unless noted otherwise.
There was wide variability in the percentage of patients reporting missed or canceled visits due to COVID-19 across study waves (Wave 3 (05/01/20-05/22/20): 22.4%; Wave 4 (07/15/20-08/21/20): 16.0%; Wave 5 (11/30/20-03/03/21): 15.5%; Wave 6 (04/12/21-07/16/21): 7.5%; Wave 7 (09/08/21-12/16/21): 3.1%; and Wave 8 (02/17/22-05/19/22): 5.3%). Overall, data trends indicate a decline in the percentage of patients who reported missing or canceling healthcare appointments due to concerns about COVID-19 over the study time period.
Bivariate analyses exploring the relationship between patient sociodemographic, or health characteristics and missed/canceled visits did not reveal any consistent predictors of visit non-attendance across the study waves (Table 2), although there were isolated associations at certain timepoints (eg, educational attainment in Wave 4, living below the federal poverty level in Wave 7). In later waves, those patients who missed or canceled a visit were younger on average than those who did not (Wave 6: 62.7 vs 64.8, P = .03; Wave 7: 60.4 vs 64.8, P = .02; Wave 8: 61.3 vs 64.8, P = .02). Health literacy and patient activation did not have a consistent relationship with missed/canceled visits during our study period.
Bivariate Analyses of Missed/Canceled Visits by Patient Demographic and Psychosocial Characteristics. a

χ2 tests and t-tests are used to assess the associations between patient characteristics and outcomes at each wave. Bold text indicates results that are statistically significant.
Figures are frequencies and percentages unless noted otherwise.
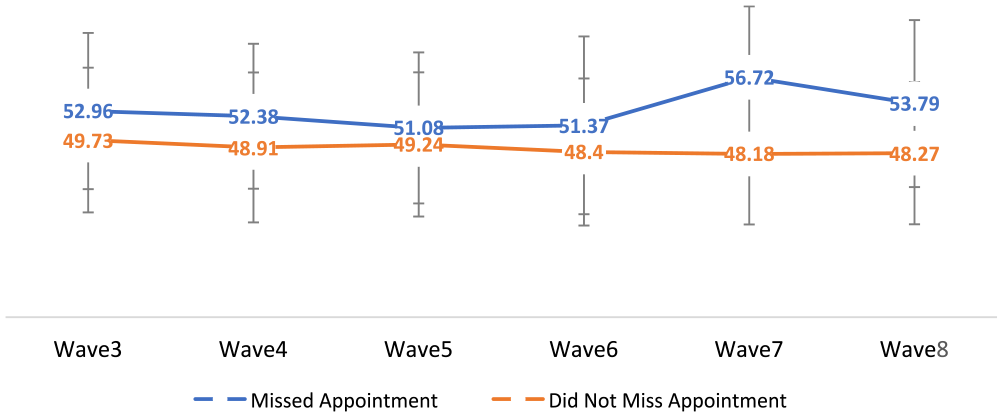
In contrast, elevated anxiety and depression symptoms were consistently and significantly associated with visit non-attendance due to COVID-19 across each study wave. Individuals reporting greater depression and anxiety symptoms were more likely to miss or cancel visits due to COVID-19 related concerns than their counterparts (Table 2). Figures 1 and 2 provide a visual depiction of the difference in depression and anxiety t-scores across study waves among participants who chose to cancel and/or miss a healthcare appointment due to COVID-19 concerns and those who did not; higher t-scores represent worse depression and anxiety symptoms.

PROMIS anxiety t-scores, by whether participants missed an appointment.
PROMIS depression t-scores, by whether participants missed an appointment.
In multivariate analysis, similar results were found, with certain patient demographic characteristics being associated with missed/canceled visits due to COVID-19 in some waves but not others (eg, female sex in Wave 4 and Wave 5, younger age in Waves 6 to 8; Table 3). In later waves (wave 6 through 8), older participants were less likely to miss or cancel an appointment (Table 3). Only greater anxiety symptoms remained a significant and consistent predictor of visit non-attendance due to COVID-19 concerns across nearly all study waves (Table 3).
Multivariate Analyses of Missed/Canceled Visits by Patient Demographic and Psychosocial Characteristics. a

Logistic regressions, OR, and 95% confidence intervals are presented. Bold text indicates results that are statistically significant.
Race is excluded from model, due to insufficient data.
Discussion
Findings from this longitudinal study revealed an overall decline in missed or canceled appointments due to COVID-19 concerns over the course of the pandemic. In contrast to studies conducted before, which found sociodemographic characteristics like health literacy, race, or socioeconomic status to be predictive of visit non-attendance, our study highlighted the role played by psychological factors, such as increased anxiety and depressive symptoms.3,21 After controlling for relevant covariates, we found that only greater anxiety symptoms were consistently associated with canceling or missing medical appointments due to COVID-19 across nearly all surveys.
Our study was not able to determine the exact reasons behind longitudinal changes in visit non-attendance during the COVID-19 pandemic. However, the decline in canceled or missed medical appointments across study waves may have been influenced by the introduction of the COVID-19 vaccine in early 2021 and its increased availability over time. As higher risk patients, participants in our study were likely to be among the first to be eligible for vaccination. Increased availability of telehealth services may also have reduced rates of visit non-attendance over time as patients were able to safely attend medical visits from their home. Finally, the widespread implementation of public health and social measures to combat the spread of the virus, in tandem with less public uncertainty and fear of COVID-19 as the pandemic continued, may have led fewer patients to miss a visit due to COVID-19 concerns.
While previous research has explored the influence of patient’s anxiety or depression on medical visit non-attendance, our study is unique as it longitudinally assesses the role played by these psychological factors over the course of a pandemic. 4 Our findings reinforce that anxiety plays a significant role in non-attendance among older patients with chronic conditions. Prior studies conducted before the pandemic have shown that increased anxiety is associated with less preventive health behaviors, greater likelihood of canceling medical visits, and obtaining inadequate care. 22 During the pandemic, research from multiple countries found significant declines in appointment attendance due to fear of infection and anxiety about COVID-19. 23 In Italy, Deledda et al 24 assessed the emotional impact of the COVID-19 outbreak amongst patients with pre-existing conditions, measuring patient degree of psychological flexibility, anxiety, depression, PTSD rates, and avoidance behaviors. They demonstrated that feelings of loneliness and elevated post-traumatic stress increased likelihood of canceling medical appointments.
Results from our study can inform initiatives to reduce absenteeism and improve continuity of care. This is especially important for patients with chronic conditions, who, in comparison to patients without a chronic disease, interact with the healthcare system more frequently, have more complex care, and are more likely to experience anxiety and depression.15 -18 While prior interventions to improve visit attendance have focused predominately on the use of reminder systems to address forgetfulness or miscommunication, our findings suggest that recognizing and alleviating patient’s anxiety and uncertainty surrounding COVID-19 could be beneficial in reducing missed or canceled visits. Future studies will be needed to gain further insight on psychosocial determinants of visit non-attendance after the pandemic and to determine optimal methods of intervening for patients with depression or anxiety.
This study has limitations that should be noted. Participants were predominantly older, many had 3 or more chronic conditions, and all lived in metropolitan Chicago, IL. As a result, our results might not be generalizable to younger or healthier individuals living in other regions of the United States or globally. This study relied upon self-report of missed or canceled visits; social desirability bias may have influenced participant responses. Given the brief nature of the survey, we did not ask for details on broader practice or community-level factors that may have influenced visit attendance, such as clinic practice capacity. We also did not inquire if the canceled visit was in person or via telehealth and did not explore whether this would have made a difference to cancellation rates. Additional studies are needed to evaluate if this method of care delivery would alleviate individuals’ anxiety regarding seeking care.
Conclusion
To our knowledge, this is the first study that has specifically examined visit non-attendance over time throughout the pandemic. Our results highlight the importance of considering psychosocial determinants of care seeking and avoidance, particularly during pandemics and times of national emergencies. Our study results emphasize the influence of increased anxiety symptoms on medical visit non-attendance for at risk patient populations during times of uncertainty. Understanding root causes underlying missed medical care during the COVID-19 pandemic can better inform provider and health-system approaches to improve visit attendance and continuity of care among adults with increased healthcare needs as the pandemic continues to evolve, or in future public health emergencies.
Footnotes
Authors’ Note
Prior Presentations: Findings were presented as a poster presentation at the NAPCRG (North American Primary Care Research Group) 51st Annual Meeting on October 31, 2023.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: SCB reports grants from the NIH, Merck, Pfizer, Gordon and Betty Moore Foundation, RRF Foundation for Aging, Lundbeck, Gilead, and Eli Lilly through her institution; and personal fees from Gilead, Sanofi, Pfizer, University of Westminster, Lundbeck, and Luto outside the submitted work. APP reports grants from Merck, Pfizer, Gordon and Betty Moore Foundation, RRF Foundation for Aging, Lundbeck, Gilead, and Eli Lilly through her institution; and personal fees from Gilead. MSW reports grants from the NIH, Gordon and Betty Moore Foundation, and Eli Lilly, and personal fees from Pfizer, Sanofi, Luto UK, University of Westminster, and Lundbeck outside the submitted work. All other study authors have no conflicts of interest to report.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by funding from the National Institutes of Health, Grant Numbers R01DK110172; R01NR015444, R01AG046352, R01AG030611; P30AG059988; and R01AG075043. REDCap software is supported by the National Institutes of Health’s National Center for Advancing Translational Sciences, Grant Number UL1TR001422. The opinions expressed in this paper are those of the authors and do not necessarily represent those of National Institutes of Health.