
Abstract
Introduction/Objectives:
With growing vaccination misinformation and mistrust, strategies to improve vaccination communication across community-based settings are needed.
Methods:
The Rural Adolescent Vaccine Enterprise (RAVE), a 5-year (2018-2022) stepped-wedge cluster randomized study, tested a clinic-based practice facilitation intervention designed to improve HPV vaccination. An exploratory aim sought to explore the use of partnerships between primary care clinics and a community partner of their choosing, to implement a social marketing campaign related to HPV immunization. We assessed perceptions about the value and success of the partnership, and barriers and facilitators to its implementation using a 29-item community partner survey, key informant interviews, and field notes from practice facilitators.
Results:
Of the initial 45 clinics participating in RAVE, 9 were unable to either start or complete the study, and 36 participants (80.0%) were actively engaged. Of these, 16/36 clinics (44.4%) reported establishing successful partnerships, 10 reported attempting to develop partnerships (27.8%), and another 10 reported not developing a partnership (27.8%), which were often caused by the COVID-19 pandemic. The most common partnership was with public health departments at 27.3%. Other partnerships involved libraries, school districts, and local businesses. More than half (63.7%) reported that creating messages regarding getting HPV vaccination was moderately to very challenging. Just under half reported (45.5%) that messaging was hard because of a lack of understanding about the seriousness of diseases caused by HPV, parents being against vaccines because of safety concerns, and religious values that result in a lack of openness to HPV vaccines. Community partners’ health priorities changed as a result of RAVE, with 80% prioritizing childhood immunizations as a result of the RAVE partnership.
Conclusions:
Community groups want to partner with primary care organizations to serve their patients and populations. More research is needed on how best to bring these groups together.
Keywords
Introduction
Community-oriented primary care (COPC), an approach where healthcare and community medicine are brought together in a coordinated effort, has been in existence for decades. 1 COPC includes both the delivery of primary clinical care with attention to continuity, and a focus on appraising community needs followed by planning and service provision while evaluating the effects of care. 1 Despite this framework, primary care and public health efforts have remained relatively distinct sectors. 2 The increasing need to address health disparities has resulted in renewed efforts to better integrate primary care with population health services.3 -5 Many health-related areas have benefitted from such partnerships, including maternal health, neonatal and children’s health, nutrition and physical activity, and home-based elder care.6 -9
As trends in vaccine hesitancy continue to grow,10 -12 vaccination delivery is an area ripe for COPC. In 2019, the reluctance to receive recommended vaccinations due to parental concerns was identified as 1 of the top 10 threats to global health by the World Health Organization (WHO). 12
A 2021 report indicated that the human papilloma virus (HPV) now infects approximately 14 million new individuals each year in the U.S. with over 50% of infections occurring in 15- to 24-year-olds. 13 Unfortunately, up-to-date vaccination against HPV remains low at a rate of 62.6%, 14 with rural areas experiencing significant disparities in HPV vaccination. 15 Since HPV vaccination is recommended for all children, starting at ages 9 to 11 years, 16 parental concerns about vaccination are important to understand. In a 2021 survey of 78,728 respondents, reasons given by parents for not vaccinating their children include that it is not needed/necessary, safety concerns, perceptions that it is not recommended, lack of knowledge about the vaccine, or that child is not sexually active, which collectively accounted for 75% of responses. 17 Caregivers of 39,364 unvaccinated adolescents reported safety concerns as the primary reason for not initiating the HPV vaccine series, which increased from 13.0% in 2015 to 23.4% in 2018, despite an actual decrease in adverse event reporting during the same time period. 17
These findings demonstrate a rise in vaccine hesitancy overall and especially with the HPV vaccine and suggest a need for new educational supports in and outside of the primary care clinical setting. Within a larger cluster-randomized trial testing a clinic-based intervention to improve HPV vaccination, we conducted an exploratory study to assess the development and implementation of partnerships between rural primary care clinics and community-based or public health organizations formed to conduct social marketing campaigns aimed at improving HPV vaccine readiness among rural Oregon families.
Methods
Study Design and Components
The Rural Adolescent Vaccine Enterprise (RAVE) is a 5-year stepped-wedge cluster randomized study designed to test a clinic-based intervention to improve HPV vaccination among rural Oregon primary care clinics. 18 Forty-five family medicine and pediatric clinics enrolled and were randomized in the study, which began in 2018 and ended in late 2022. Participating clinics were recruited from the Oregon Rural Practice-based Research Network. 19 Oregon Health & Science University’s Institutional Review Board (IRB# 18660) approved all study activities.
The clinic-based intervention involved each clinic receiving 18 months of longitudinal practice facilitation grounded in the Model for Improvement and tailored to individual clinic needs. 20 With the guidance of a practice facilitator, clinics created aim statements, used standardized tools (eg, fish-bone diagramming) to identify and prioritize targets for improvement, and conducted plan-do-study-act cycles to guide improvement. An exploratory aim of the study included the development of a partnership between each clinic and a community-based or public health organization of their choice to create a social marketing campaign designed to create vaccine ready families in their community. Each clinic was responsible for identifying a partner and reaching out to establish the partnership. Examples of selected organizations include: libraries, school districts, local public health groups, and local businesses. Together, with support from a practice facilitator, clinics and community groups created their campaign to promote HPV vaccination. Each clinic received $2000 to complete these activities.
Partnership Assessment and Data Collection
Three approaches were used to assess the community partnerships. First, a 29-item community partner survey was designed and pilot tested to assess community partner health priorities before and after RAVE, perceptions about the effectiveness of their campaigns, past and future planned activities with community partners, challenges associated with messaging the HPV vaccine in their respective communities, and what specifically makes HPV vaccine messaging challenging. Surveys were administered after the social marketing campaigns had been implemented. Data were entered using REDCap. 21
Second, practice facilitators conducted key informant interviews with staff members at both primary care clinics and each partnering community-based organization. The interview questions included an assessment of the extent to which a partnership was formed, the process by which they found a community partner, best aspects of the partnership, what aspect of the partnerships were challenging, what they would do differently in a future partnership program, and what they learned from this partnership experience that they wish they had known at the start. The interview questions for the community partners were the same. The interviews lasted approximately 30 min, and field notes were taken and entered into REDCap for qualitative analyses.
Finally, qualitative researchers (authors CB and NR) used supplemental qualitative data, including implementation field notes and comments in post-intervention surveys to better understand partnership formation and execution. These data were used to develop representative case examples that reflected how participating clinics partnered with community-based organizations (Supplemental Appendix A).
Data Analyses
Descriptive statistics including frequencies and percentiles were used to assess survey responses using SPSS version 29. Classical content analysis was used to identify and characterize emergent themes from the interview data. 22 The field notes were independently coded by authors (PAC and MBE) and consensus meetings were used to review codes, identify emergent themes, define the themes, and then choose exemplars that reflect them.
Results
Of the initial 45 clinics participating in RAVE, 9 were unable to either start or complete the study, and 36 participants (80.0%) were actively engaged in study activities. Of these, 16 clinics reported establishing successful partnerships (44.4%), 10 reported attempting to develop partnerships (27.8%), and another 10 reported not developing a partnership (27.8%). Eleven community partners completed the community partner survey (42.3% response rate among those who formed or attempted to form partnerships), and data provided reflected a diverse group of community partners with the most common being public health departments at 27.3% (Table 1). More than half (63.7%) reported that creating messages regarding getting HPV vaccination was moderately to very challenging. Just under half reported (45.5%) that messaging was hard because of a lack of understanding about the seriousness of diseases caused by HPV, parents are against vaccines in general because of safety concerns, and religious values result in a lack of openness to HPV vaccines (Table 1).
Characteristics of the Community, Community Partners, and Their Perspectives on What Makes Messaging HPV Vaccines to the Community Challenging (n = 11).

Categories not mutually exclusive.
Table 2 reports on the community partners’ community health priorities before and as a result of RAVE, which shows that 30% prioritized childhood and adolescent vaccines before RAVE and 80% prioritized this as a result of RAVE. In addition, when assessing the frequency of partnering with different community groups, the community partners reported most often never partnering with dental clinics, pharmacies, primary care clinics, youth organizations, childcare organizations, adult organizations, religious organizations, and local businesses before RAVE, but indicated they planned to increase partnerships with these groups as a result of RAVE (Table 2). The community partners rated 18.2% of their typical public health/social media campaigns as moderately to very effective, while 63.7% rated their RAVE Campaigns as moderately to very effective (Table 2).
Community Partner Experiences Before and Planned Experiences as a Result of RAVE (n = 11).

Twenty-six clinics completed key informant interviews. Of these, 14 (53.8.%) established successful partnerships, 5 (19.2%) attempted to established partnerships, and 7 (26.9%) were unable to establish partnerships.
Successful Partnerships
The first emergent theme among successful partnerships was Relationship Building and/or Strengthening (Table 3). Here we found that if the development of rapport between those working on the partnership was meaningful and sustained, the experience was enjoyed and successful. This involved strong communication for both planning and execution. The connection, in some cases, was the beginning of a new relationship and in others, there was a reconnection, but there was a sense of wanting to sustain the relationship rather than it being “one and done.” In addition, we found that building these relationships took considerable time and effort on behalf of the clinic, particularly if the connection was brand new.
Summary of Emergent Themes from Clinic Interviews According to Community Partnership Status (n = 26) Clinics.

The second emergent theme was Connection to the Community, which we described as a sense of bonding with the community in terms of people or patients that fostered a shared mission based on aligned values. This bonding served as a type of glue that kept the partnership together and motivated participants in their work. The third emergent theme was Operational Features, which were aspects of partnership functioning, such as established routines, organizational culture, viewpoints, or perceived roles or standards that either facilitated success or had to be overcome to achieve success.
The last emergent theme among those with successful partnerships was Alignment of Health Related Values, which we described as perceived or actual orientation of the partners on ideals related to health. This involved some hesitancy about pushing what may be perceived as a controversial agenda as well as embracing a health-related agenda, which was easier when the partner was also in the business of health. These themes are further highlighted in Case Example 1 (Supplemental Appendix A).
Attempted Partnerships
Emergent themes partnerships that were attempted but not fully formed included a Lack of Interest, Lack of Experience, Lack of Connection, and Poor or Miscommunication (Table 3). This represented an absence of purpose, perceived lack of relevance to their daily work or lack of prior experiences that might otherwise effectively link the partnership to a joint mission. Poor or miscommunication within the practice or partner organization also affected how well connections developed and were maintained. Without these, the partnership did not solidify.
A second emergent theme was the impact of the COVID-19 where the pandemic affected some organizations more than others. When schools and other organizations shut down, these likely partnerships could not recover and implement activities. These themes are further highlighted in Case Example 2 (Supplemental Appendix A).
No Partnership Developed
The emergent themes for No Partnership Developed also included the Impact of COVID Timing, where they were attempting to implement their partnerships at a time when COVID was hitting rural communities hard. This prevented even attempting to develop a partnership and the effort was quickly abandoned. Similarly, clinic capacity was affected by clinician turnover or limited time and resources, all of which affected clinic’s attempts to develop partnerships. These themes are further highlighted in Case Example 3 (Supplemental Appendix A).
Thirteen community partners participated in the key informant interviews (Table 4). Of these, 9 (100.0%) reported developing well-established partnerships, and 4 were partially executed; thus, 9/14 or 64.3% of well-established partnerships were represented. Those who did not fully develop or attempted to develop partnerships declined to be interviewed. Four emergent themes were identified among the well-established partners. These included Existing Strategies Important for the Community that Can be Deployed, which is recognition and pride on the part of the community partner that they and the clinic both have contributions to make in their community and that joining their skillsets makes them stronger. Partners recognize the clinical knowledge and potential influence the clinic can have on parents’ receptiveness to vaccines, while the community partners have a good understanding of challenges and nuances of community-based activities and have more available resources. A second emergent theme was Relationship Development or Strengthening, which is the establishment of a connection or a reconnection that served to foster nuanced activities between clinic and community partner. A third emergent theme was Excitement for Future Work, which involved an expression that there is more to do and/or showed a general excitement for the work as personally gratifying or as well as beneficial to the partners and the community. The final emergent theme for those with well-established partnerships was Co-learning or Information Sharing that resulted in nuanced knowledge about each other and the community they are both serving.
Emergent Themes from Community Partner Interviews According to Partnership Status (n = 13 partners).
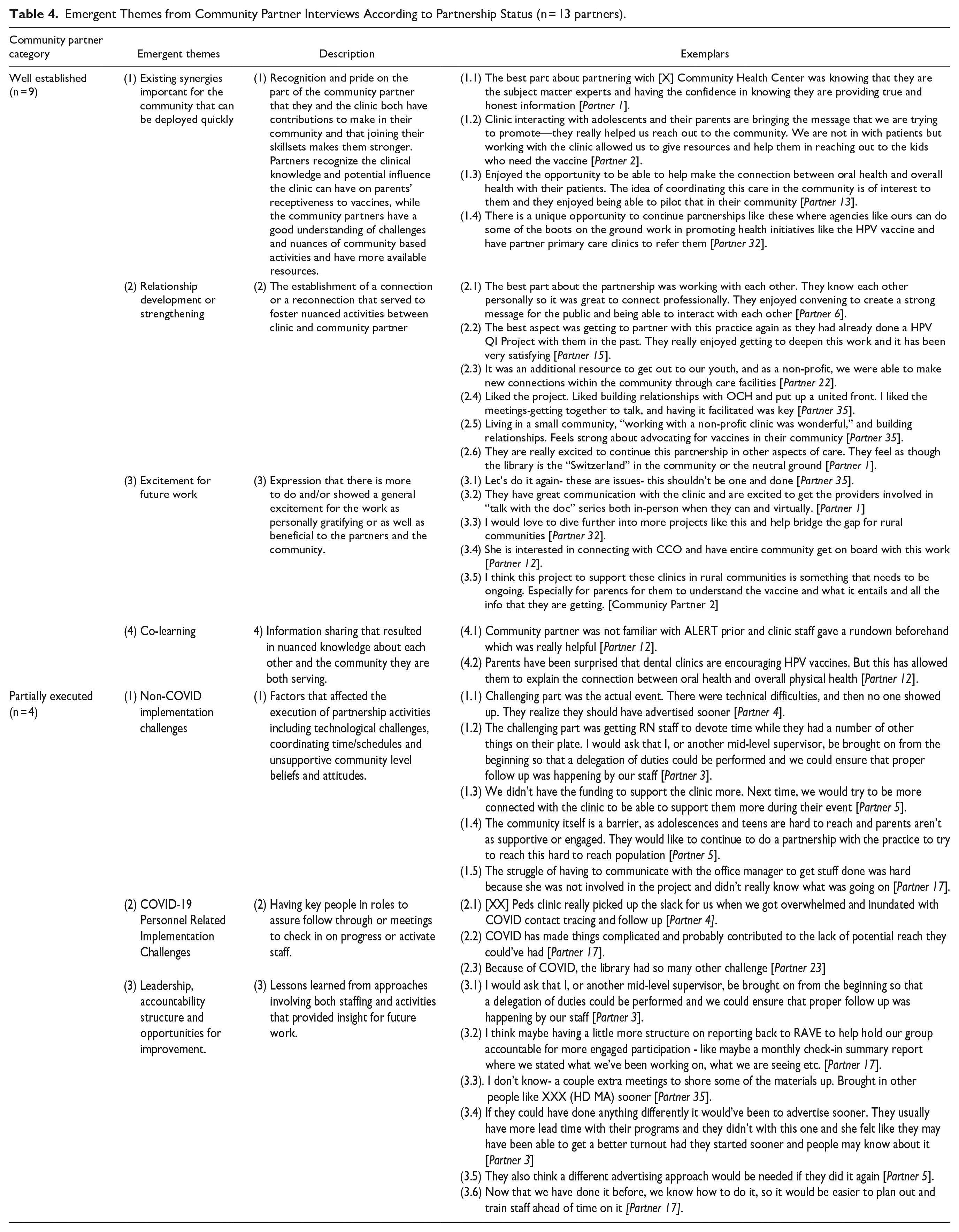
Among community partners who reported having partially developed partnerships, 3 themes emerged, the first of which involved Non-COVID Implementation Challenges or factors that affected the execution of partnership activities including technological challenges, coordinating time/schedules, and unsupportive community level beliefs and attitudes (Table 4). The second was COVID-19 Personnel-related Implementation Challenges which involved having key people in roles to assure follow through or meetings to check in on progress or activate staff. The final emergent theme was Leadership, Accountability Structure, and Opportunities for Improvement, which were lessons learned from approaches involving both staffing and activities that provided insight for future work.
Discussion
In this exploratory study, we sought to understand the development and implementation of a partnership between primary care clinics and community-based organizations to promote HPV vaccination through social marketing. With minimal support from a practice facilitator, just over 40% of clinics provided data indicating they successfully developed a partnership and conducted a social marketing campaign. While developing novel partnerships posed a challenge for most clinics, and all partnerships were impacted by the COVID-19 pandemic, valuable and diverse partnerships were formed. Those that formed partnerships reflected on their double value, first by directly pertaining to disseminating important HPV vaccination information, and secondly by indirectly contributing to future community-oriented primary care outreach potential. They also highlighted their higher perceived effectiveness compared to other unilateral social marketing campaigns. This is consistent with literature showing value of COPC6 -9 and suggests that while many clinics are able to develop community partnerships with little support, other clinics may need additional support to fully form these relationships.
For many partners, the importance of childhood vaccination as a specific priority in their work evolved during their participation in RAVE. Only 30% noted this priority prior to participation, but 80% noted it afterward. This suggests that participating community organizations had a willingness to trust primary care clinics in identifying important health needs for the community and an adaptability of their internal priorities. The perceived challenges in creating HPV vaccination messaging due to the public’s lack of understanding about the seriousness of diseases caused by HPV, concerns about vaccine safety, and religious values or perceptions that children are not at risk were similar to those reported previously. 17 Despite these challenges, the majority noted higher perceived effectiveness of the RAVE social marketing campaign compared with their usual campaigns. It may be that by partnering with primary care clinics delivering HPV preventive care, they perceived the campaigns would be more impactful.
Successful partners tended to share health-related goals and values which allowed for the rapid operationalization of social marketing campaigns. Conversely, unsuccessful partnerships noted communication difficulties, lack of experience forming these types of collaborative relationships, and insurmountable barriers and strains from the COVID-19 pandemic. The COVID-19 pandemic impacted both clinics and community organizations alike through increased isolation, decreased staffing, and competing priorities.
The perspectives of unsuccessful clinics suggest an opportunity for additional supports that could improve the success rate in developing these partnerships. In particular, community organizations tended to have a designated employee whose job description included community outreach, but clinics rarely had staff with designated time for such outreach activities. Reflecting on the communication and staffing barriers experienced by some clinics, an individual in this role may have been useful. Community health workers may hold promise as individuals who could play this role in an applied COPC model.
Moving toward a model of community-oriented primary care requires further study of the optimal strategies to develop and sustain longitudinal partnerships between primary care clinics and community-based organizations. Though our exploratory intervention included both core features of COPC (the delivery of primary clinical care with attention to continuity; and a focus on appraising community needs followed by planning and service provision while evaluating the effects of care), we found many challenges existed with fostering these partnerships, which may explain why primary care and public health efforts have remained relatively distinct sectors. 2 These longitudinal relationships hold great potential for addressing the highest priority public health needs and providing a responsive infrastructure to serve community needs. Future research should focus on resources needed to make partnerships successful in different communities, and the most effective and sustainable models of implementation.
Limitations
As an exploratory study, this project was not designed or powered to be widely generalizable or allow for rigorous controlled analysis. Even so, this pilot project demonstrated on a small scale, the ability of several clinics to develop and implement, with varying levels of support, a community-specific partnership following a COPC model. Future research should consider assessing the effectiveness of both the partnership and the social marketing strategy and should consider the barriers and facilitators to successful and sustainable partnerships in more detail than we were able to achieve. Survey response rate and participation in the interviews was lower than expected, which increases the likelihood of response bias. Finally, as a project that occurred during the unique circumstances of the COVID-19 pandemic, it is difficult to predict how the partnerships may have evolved outside this timeframe. While it is likely that constraints on staffing, resources, and interactions made many elements of this partnership more challenging, it is also possible that some elements, like prioritization of vaccination, may have actually been facilitated by this unique circumstance.
Conclusions
With minimal support, some primary care clinics successfully initiated and developed partnerships with community organizations to conduct a social marketing campaign to improve HPV vaccination. An applied COPC model, as demonstrated in these partnerships, holds great promise to address issues of public health significance, like vaccination, in the future. More research is needed to identify the optimal implementation strategies for these types of partnerships and the barriers and facilitators to successful and sustainable partnerships.
Supplemental Material
sj-docx-1-jpc-10.1177_21501319241231405 – Supplemental material for Primary Care and Community-Based Partnerships to Enhance HPV Vaccine Delivery
Supplemental material, sj-docx-1-jpc-10.1177_21501319241231405 for Primary Care and Community-Based Partnerships to Enhance HPV Vaccine Delivery by Patricia A. Carney, Marie B. Engstrom, Chrystal Barnes, NithyaPriya Ramalingam, Caitlin Dickinson, Cort Cox, Laura K. Ferrara, Paul M. Darden, Lyle J. Fagnan, Miguel Marino and Brigit A. Hatch in Journal of Primary Care & Community Health
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the American Cancer Society (RSG-18-022-01-CPPB).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.