
Abstract
Background:
In 2021, the Health Resources and Services Administration (HRSA) launched the National Hypertension Control Initiative (HTN Initiative) with the goal to enhance HTN control through Bluetooth-enabled self-measured blood pressure (BT-SMBP) monitoring and use this data to inform clinical decisions in Federally Qualified Health Centers (FQHCs) with a large proportion of their population with uncontrolled blood pressure (BP). We sought to understand the experience of Michigan-based FQHCs in implementing the HTN initiative.
Methods:
Staff from three Michigan-based FQHCs were invited to participate in semi-structured interviews from September to November 2022. Interviews were conducted in-person and were based on the Tailored Implementation in Chronic Diseases framework. Content analysis was performed by three coders.
Results:
Ten staff participated in interviews (FQHC 1: n = 6, FQHC 2: n = 1, FQHC 3: n = 3). The FQHCs differed in their stage of implementation and their approach. FQHC 1 created a large-scale, community health worker driven program, FQHC 2 created a small-scale, short term, BP device loan program, and FQHC 3 created a primarily outsourced, large-scale program through a contracted partner. Positive staff attitudes and outcome expectations, previous experience with SMBP grants, supportive clinic leadership, social support, and free BP cuff resources were identified as facilitators to implementation. Patients’ high social needs, SMBP-related Technology, and insufficient workforce and staff capacity were identified as barriers.
Conclusion:
BT-SMBP among FQHC patients is promising but challenges in integrating SMBP data into clinic workflow, workforce capacity to support the high social needs of participants, and to assist in reacting to the more frequent BP data remain to be overcome.
Keywords
Introduction
Nearly half of all Americans (47% or 116 million people) experience hypertension (HTN), and only about half of Americans with HTN have controlled blood pressure (BP).1 -3 Black Americans have one of the highest prevalence of HTN in the world and are less likely than White Americans to have their BP controlled. 3 Disparities in BP are also evident among low-income Americans, who have higher prevalence and less BP control than other Americans. 4
New strategies to reach and support the control of BP in historically marginalized populations are needed. One approach is through partnerships with Federally Qualified Health Centers (FQHCs). FQHCs provide primary care to nearly 30 million Americans, 91% are low-income, and 60% are racial/ethnic minorities.5,6 A complementary strategy to support BP control is via mobile health (mHealth), which leverages cellphone and smartphone devices already adopted by the majority of U.S. adults, and with high penetration among low-income and minoritized populations. 7
In this context, the Health Resources and Services Administration (HRSA) and the Office of Minority Health partnered on the National Hypertension Control Initiative: Addressing Disparities among Racial and Ethnic Minority Populations (HTN Initiative).8,9 Through this initiative, in 2021, HRSA awarded nearly $90 million in supplemental funding to FQHCs with a large proportion of patients with uncontrolled BP (<58.9%). The HTN Initiative’s goal was to enhance BP control using Bluetooth-enabled Self Measured Blood Pressure monitoring (BT-SMBP) for patients with HTN and use their data to inform HTN treatment. 8 With the support of BT-SMBP devices, combined with supporting mHealth cell phone apps, individuals can monitor their BP and communicate that data back to their healthcare providers in real or near real-time. We sought to understand the experience of Michigan-based FQHCs in implementing the HTN initiative via qualitative interviews based on the Tailored Implementation in Chronic Disease (TICD) Framework.
Methods
This is a qualitative study using semi-structured interviews to assess barriers and facilitators to implementing BT-SMBP for patients with HTN and the clinical use of their BP data to inform HTN treatment at FQHCs.
Theoretical Framework
The semi-structured interview guide was developed using the Tailored Implementation in Chronic Diseases (TICD) determinant framework to assess barriers and facilitators to BT-SMBP patient initiation and clinic integration. The TICD is a comprehensive framework based on an extensive systematic review of determinants of practice in primary and secondary care as well as public health services. The TICD explores determinants of practice in seven domains which include guideline factors, health professional factors, patient factors, professional interactions, incentives and resources, capacity for organizational change, and social, political, and legal factors. 10 The interview guide began with a general description of the HTN initiative at each FQHC network. Open ended questions assessing all TICD domains except social, political, and legal factors were included in the interview guide. The interview guide concluded with a query of general advice for other FQHCs to implement BT-SMBP.
Funding
This work was funded by the National Institutes of Health- National Institutes of Minority Health and Disparities (R01MD011516) and research funds provided by the University of Michigan.
Study Participants and Procedures
Staff members from three Michigan-based FQHC Networks were invited to participate in semi-structured interviews from September to November 2022. As one of the FQHCs had not begun enrolling patients at the time of their interviews, a follow up interview was conducted with one staff member in February 2023. FQHCs were purposively selected based on location in Michigan and receipt of funding for the program. Participants were compensated $20.
Data Collection
Interviews were conducted jointly by AH and CW, when possible, to allow for one researcher to take field notes. Interviews were conducted in-person at the FQHCs and were 15-60 minutes in length. Interviews were audio recorded, professionally transcribed, and reviewed by the research team for accuracy.
Data Analysis
The research team created a codebook based on the TICD framework; Transcripts were deductively coded based on the TICD framework using Atlas.TI, a qualitative data analysis software. AH, CW, and MM coded two transcripts, meeting via Zoom after coding each transcript to discuss discrepancies until a consensus was reached. The remainder of the transcripts were randomly assigned to AH, CW, and MM to code independently. The coded data was exported into Excel spreadsheets for review. Data was sorted according to preliminary themes and refined into final themes.
Results
Participant Characteristics
Ten staff members from 3 Michigan-based FQHCs participated in interviews (FQHC 1: n = 6, FQHC 2: n = 1, FQHC 3: n = 3). The number of interviews conducted at each FQHC was determined by ability to establish contact with FQHC staff, staff availability, and relevant staff given each FQHCs unique implementation status. Participants had a mean age of 43 years, half identified as White and were divided between clinic administration and direct patient care providers (Table 1).
Participant Characteristics.
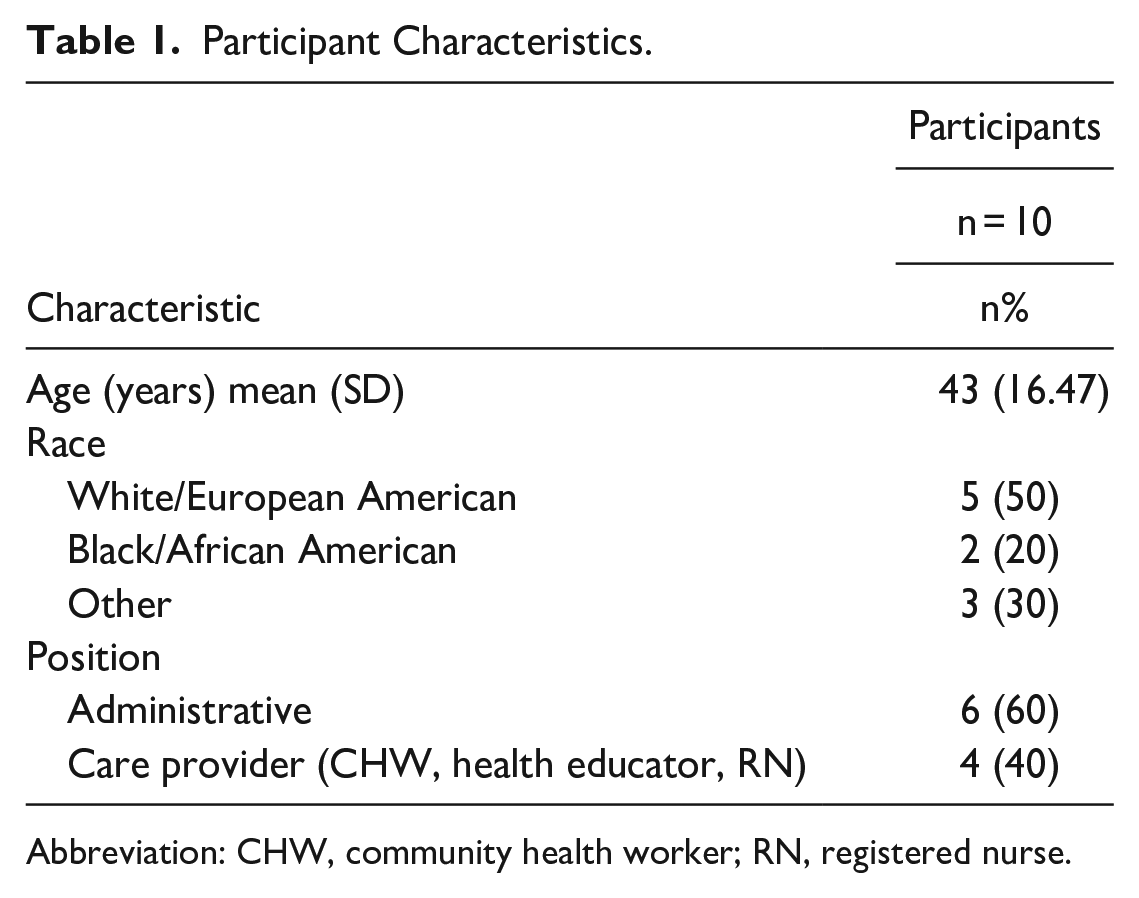
Abbreviation: CHW, community health worker; RN, registered nurse.
Overview of BT-SMBP Program by FQHC
FQHC 1 began implementation in February 2021 and created a large-scale, data-driven, CHW-supported remote monitoring program. Patients with uncontrolled BP in the prior year were identified in the electronic medical record (EMR) and contacted by the clinic’s CHW for enrollment. After 20 months, FQHC 1 enrolled over 580 patients into the program. As necessary, patients were offered the alternative to utilize paper BP logs. BP data was manually transferred from the smartphone application (or paper BP log) to the clinic’s EMR by CHWs. Patients graduated from the program after 2 months of controlled BP. Participants were able to keep their BP device after graduation. FQHC 2 began implementation in September 2022 and structured the HTN initiative as a small-scale, short-term BP device loan program; Thirty-six BP devices were available to patients for one-month loans. Patients were identified in-real time during clinic appointments. FQHC 2 manually transferred patient’s BP data from the patient’s app to the clinic’s EMR. FQHC 2 had just begun enrollment, thus complete enrollment data was not available at the time of the interview. After an unsuccessful attempt to launch the BT-SMBP program internally, FQHC 3 worked with an outside company to launch a large-scale, social needs driven BT-SMBP program. The company was responsible for patient outreach, enrollment, and tracking BP measurements. Eligible patients were primarily identified via EMR searches; Patients with comorbidities and high social and economic needs were prioritized for enrollment. Participants were loaned a BT-BP device for the duration of their participation; The partner company facilitated data transfer directly into the clinic EMR, which was then accessible by providers. After their first 2 months, approximately 250 patients had enrolled. FQHC 3 intended to engage participants for at least a year.
Barriers and Facilitators to implementing BT-SMBP in FQHCs
The identified barriers and facilitators to implementing the BT-SMBP program fell within five of the seven TICD domains; These domains include individual health professional factors, capacity for organizational change, patient factors, guideline factors, and incentives and resources.
Individual Health Professional Factors
Attitude/outcome expectancies
Facilitators were abundant in the individual health professional factors domain. Staff at all three FQHCs expressed overall positive attitudes towards the SMBP Program. Staff attitudes at FQHC 1 and 3 were tied to observed or anticipated patient outcomes including controlled BP, reduced emergency department visits, greater medication adherence, increased knowledge about hypertension, appointment attendance, and increased trust in the healthcare system,“[. . .] it’s very rewarding to see that their blood pressure is under control, it makes me happy just to feel that I had made a difference[. . .] there’s barriers, there’s hiccups, but it’s worth it” (FQHC 1). FQHC 3 staffs’ positive attitudes were also tied to anticipated clinician benefit, including the ability to create more tailored hypertension treatment plans, increased use of self-management goals in addition to BP medication, and alleviate their mental burden of worrying about a patient that presented with high BP. FQHC 2’s positive attitude toward the program was tied to their easier-than-anticipated experience implementing the program.
Knowledge/skills
Knowledge and skills also served as significant facilitators. FQHCs 1 and 2 shared that being a part of other hypertension grant initiatives helped prepare them to participate in the HTN initiative through preestablished workflows, and providing a foundation of knowledge, “I do work with Million Hearts, so [. . .] that was very helpful in terms of, um, just giving a step-by-step guide to, you know, how to create and build this program [. . .]” (FQHC 2).
Capacity for Organizational Change–leadership support
The capacity for organizational change domain had many facilitators. FQHC 1 and 2 expressed strong program leadership. At FQHC 1, staff shared having program champions and providing CHWs with significant training opportunities and mentorship from seasoned CHWs and health educators. FQHC 2 shared hiring a program manager.
Patient Factors
Patient motivation
At FQHC 1, staff widely cited that giving patients a free BP cuff motivated patient enrollment, and that social support from CHWs motivated program engagement, especially in light of the isolation caused by the COVID-19 pandemic.
Patient beliefs/knowledge
A couple of staff at FQHC 1 and 3 identified patient education on hypertension as a facilitator to patient engagement, emphasizing the link between knowledge and self-efficacy, “[. . .] it is really a question of making sure that the patient is comfortable with recording his or her blood pressure [. . .] Getting them used to the fact that there is a right way to measure the blood pressure and take the blood pressure” (FQHC 3).
Patient needs
FQHC 1 cited patients’ lack of digital resources and digital literacy as barriers to enrollment. “I think one of the reasons [patients decline to participate] is, it is, like, our digital literacy in our patients too, right? [. . .] So, it’s sometimes hard for them [. . .] they don’t have a smartphone. Like, [. . .] it’s hard to kind of tell. . .the whole set up, once they don’t have all the right tools to be able to, you know, set it up. So, a lot of patients who don’t have one, we give them a physical paper log to document, but at the same time, it’s. . .well, there’s no point in having [BT-SMBP] if you’re not going to be using your phone to integrate it and send that information back to your provider.” More generally, FQHC 1 cited their patient population’s high level of social needs as a barrier to program engagement, “You’re going to deal with patients who are mentally unsound, physically unsound [. . .] you need to figure out what’s going on with them, and you have to dig deep with a patient. What are your barriers? Financial barriers [. . .] literacy barrier[s]. They don’t know where they need to go. It’s housing barriers that we deal with, transportation barriers [. . .].” In response to their patients’ social needs, several staff expressed that providing wrap-around resources, including sodium-free herbs, low-sodium cookbooks, and hypertension resource guides as potential facilitators to patient engagement.
Guideline Factors
Feasibility
Technology-related barriers challenge program feasibility, from setting the patient up to getting the BP data to clinicians in all three clinics. FQHC 2 shared that the WIFI connection at one of their clinics was not strong enough to set up the patients’ devices, which limited in-person patient training. Staff members at FQHC 1 shared problems pairing the BP devices with cell phones. One staff member shared that many patients had a cellphone model that would not pair with the BP device’s corresponding smartphone application. Another staff member shared that larger cuff attachments produced error messages. Staff cited difficulty maintaining the pairing between participants BP devices and their cellphones, as well as staying logged into the corresponding app, “A common problem with me [is] when a patient upgrades their phone [. . .] and they forget to download the app. They’ll start taking their blood pressure and they’ll think that the device is automatically sending it to their phone. [. . .] but they don’t have the app it’s not connected via Bluetooth, so they’re just taking their blood pressure and thinking everything’s perfectly fine.”
Without the aid of a tailored software, staff at FQHC 1 and 2 shared finding makeshift ways to use existing computer software to track program participants’ devices and participation, including Excel spreadsheets and leaving outstanding orders within their EMR.
At FQHC 1 and 2, staff shared having to manually transfer participants’ BP data to the EMR, “[BP readings don’t] automatically transfer over. So, I would need to go into one app to then print out all their blood pressure readings to then use our Athena [EMR] scan to upload it [pictures] to their chart.” In contrast, through FQHC 3’s remote monitoring partner, BPs flow directly from the patient into the patient’s EMR.
Incentives and Resources
Incentives and resources were dominated by barriers. Human resources, including staffing and staff capacity, were barriers to implementation. FQHC 1 shared having high CHW turnover rates, disrupting the continuity of the program and the social relationships made between CHWs and their patients, “[. . .] you would train a CHW or staff would take over the hypertension grant and then they would leave after four to six months [. . .] and then we would have to do the process again which it was just like, you know, like the patients want to see familiar faces too” (FQHC 1). Insufficient pay motivated staff turnover. FQHC 3 stated being heavily impacted by the industry-wide COVID workforce shortage.
Staff at the FQHCs shared already having limited capacity. At FQHC 1, CHWs shared juggling a myriad of health education and screening responsibilities which make balancing their workload with the SMBP program difficult. The dysergy of the workforce shortage and limited workforce capacity resulted in FQHC 3 changing from an mainly clinic-run program to contracting a remote monitoring company, “[. . .] everyone in healthcare is frankly understaffed and overburdened [. . .] So then when you add on another initiative like this where we’re looking at patients, we’re engaging with them, educating them, enrolling them, monitoring them, and so on, that can be a big lift. So, what we’ve done is we found a partner that will not only help us to reach out to and enroll the patients but will help us with the 24/7 monitoring.”
FQHCs shared incongruence between program funding and objectives, as one staff member at FQHC 3 put it, “When I first looked at it, my analysis of the funding that was made available through the [HTN Initiative] and the number of patients they wanted engaged, I mean there was a strong disconnect [. . .].” Limited grant funding resulted in program structures with diminished patient reach and duration of engagement; Both FQHC 2 and 3 acknowledged their inability to bill insurance exacerbated their funding challenges. As a result, FQHC 2 created a BP device loan program with a limited number of devices (12) for brief periods of engagement (1 month). FQHC 3 shared that their remote monitoring company priced according to the number of patients being monitored, which limited their reach. A complete summary of barriers and facilitators by TICD domain are presented in Table 2.
Barriers and Facilitators by Tailored Implementation in Chronic Disease (TICD) Domain.
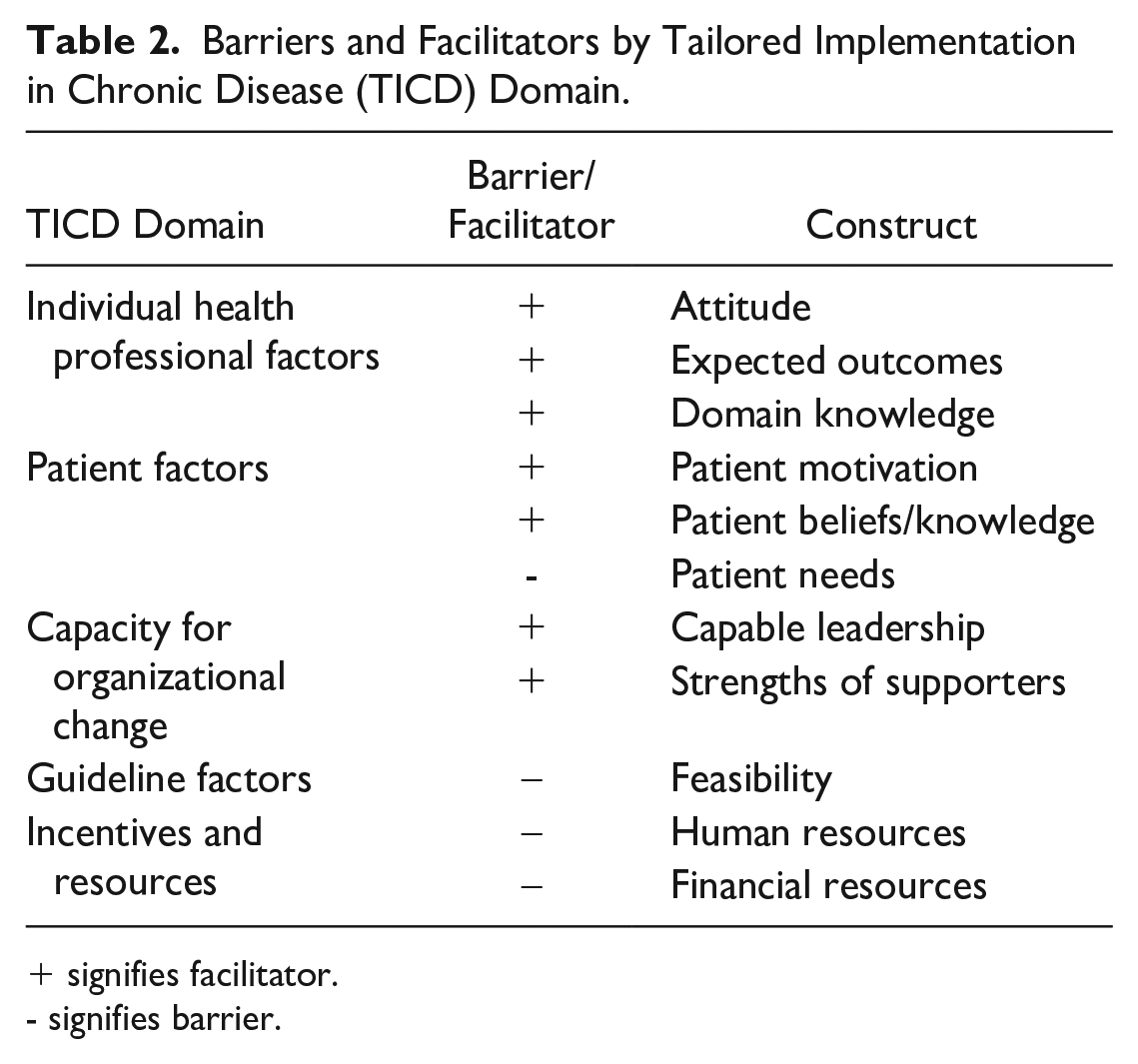
+ signifies facilitator.
- signifies barrier.
Discussion
In summary, three Michigan-based FQHCs participated in semi-structured interviews about their experience implementing the HTN Initiative. Each FQHC was at a different stage of implementation, ranging from a year and a half of implementation to preparing to begin. Implementation strategies varied significantly ranging from a small, clinic-run, loaner BT-SMBP program to a large-scale, outsourced model with continuous BP data transfer.
Facilitators to program implementation were abundant in the individual health professional factors and capacity for organizational change domains. Across FQHCs, staff demonstrated positive attitudes towards the program; many staff’s positive attitudes were tied to observed or anticipated benefits to patients and clinicians. This is notable, particularly given their multiple other responsibilities and the increased workload of BT-SMBP, FQHC staff remained positive about the program, highlighting their commitment to their patients’ health and wellbeing. Knowledge and skills acquired through participating in other SMBP initiatives provided the FQHCs with a foundation to build their programs. High capacity for organizational change, including dedicated program leadership and mentors, training opportunities, and provider champions aided implementation. Some facilitators were also present in the patient factors domain. BP devices that participants could keep and social support from CHWs were identified as strong patient motivators to program adoption and engagement.
Implementation faced several barriers; barriers were prevalent across the patient factors, guideline factors, and incentives and resources domains. Unmet social needs among patients were identified as competing priorities. Patients’ lack of digital resources and low digital literacy deterred patient enrollment and engagement.
Technology posed a significant barrier to program feasibility with insufficient WIFI, difficulty pairing devices, error messages, and a lack of technological infrastructure to track loaned BP devices, track patient engagement, and manage SMBP data. Such disjointed technology resulted in increased staff burden, requiring manual BP data transfer by CHWs into patient’s EMRs.
Short staffing and overburdened staff limited ability to implement large clinic run programs, as staff were unable to identify, enroll, and engage patients in the program in addition to their existing workload. FQHCs managed this by scaling back their program or outsourcing initiative enrollment and data transfer. Only once clinics have the necessary technology and designated program staff can they truly engage in real time monitoring.
Overall, insufficient funding negatively impacted clinics reach and duration of engagement, made contracted help financially inaccessible, and resulted in BP device loan-based programs. Such short durations of participant engagement may result in insufficient BP data to inform provider clinical decisions. From a patient standpoint, the engagement period may be too brief to cultivate knowledge of their BP and the efficacy of BP medications, thereby decreasing the benefit of increased medication adherence.
The identified barriers and facilitators present several pathways of action to bolster program implementation. FQHCs with experience implementing SMBP-related initiatives can serve as a resource to less experienced FQHCs through learning health collaboratives, clinic champions or shared protocols. Similarly, documentation of these barriers and facilitators can help inform funding entities of the FQHC BT-SMBP landscape, helping to set realistic expectations and provide additional resources in response to current unmet needs. Financially accessible technology that can aid in tracking patient engagement and convey patient data directly into the EMR in clinically useful ways has the potential to overcome several identified barriers and continue to support staff attitudes towards the program.
This study has limitations. This study represents three FQHCs across southeast and central Michigan and may not be generalizable. We did not include physicians due to scheduling challenges nor did we include patients. Lastly, staff may have provided socially desirable responses. However, this risk was attenuated by conducting 1-on-1 interviews by researchers knowledgeable about the FQHC environment and qualitative methods.
FQHCs took varied approaches to implementing the HRSA SMBP program. Across clinics, the individual health professional factors, capacity for organizational change, and patient factors domains contained facilitators to implementation. The guideline factors and incentives and resources domains were dominated by barriers. Overall, BT-SMBP among FQHC patients is promising but challenges remain to be overcome.
Footnotes
Acknowledgements
All co-authors have reviewed this publication and accept their authorship.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the National Institues of Health-National Institues of Minory Health and Disparities (R01MD011516) and research funds provided by the University of Michigan