
Abstract
Introduction/Objective:
Community health workers (CHWs) can be extremely important in many facets of healthcare, especially for marginalized communities. Health Literacy and Preventive Behaviors of Emerging Infectious Diseases and Re-emerging Infectious Diseases of the Respiratory System were important for CHWs in Preventing and Control Diseases.
Methods:
This quasi-experimental research; a 2 pretest-post group design, aimed to investigate the result of the experiential learning program of the CHWs toward health literacy and preventive behaviors of the infection of emerging and re-emerging diseases of the respiratory system. The samples are 66 CHWs working in Ngao District, Lampang Province which were divided into 2 groups; the experimental and control groups, 33 subjects for each group. The tools used in this research consisted of an experiential learning program for 6 weeks and a questionnaire concerning health literacy and preventive behaviors of emerging and re-emerging diseases in the respiratory system.
Results:
The experimental group had the mean score of health literacy regarding the prevention of emerging and re-emerging diseases of the respiratory system at the highest level (
Conclusions:
The research results could be a guideline for developing the CHW’s potential effectively and proficiently.
Keywords
Introduction
The contagious disease situation of respiratory disease is more severe and spreads rapidly due to changes in population, human behavior, disease, the ecological system of animals, and the environment. The world climate change causes global warming and the habitat is invaded by humans. This leads to occurring emerging infectious diseases and re-emerging infectious diseases. particularly, respiratory infection diseases which are easily transmitted such as COVID-19 spreading quickly across the world. Emerging infectious disease refers to a new infectious disease or disease found in a geographical area. In terms of re-emerging infection disease refers to a disease that was spread in the past and disappeared for many years and then emerged again. 1 Thailand is likely to encounter emerging infectious and re-emerging infectious diseases. Two or 3 decades ago, infectious diseases were found such as bird flu, Middle East respiratory symptoms or MERS, and Ebola virus which all were fatal.
The emerging infectious and re-emerging infectious diseases are more severe and also have a great effect on the economy and the health of people around the world. Three decades ago, the emerging contagious diseases occurred mainly from animals to humans which are around 75%. The management of emerging infectious diseases needs to get cooperation from all sectors in Thailand and foreign countries based on knowledge management and new technology development. This is done by CHWs who devote their time to take part in caring for themselves, their families, and the community which is regarded as a social capital that is an important healthcare system. 2 It is an important power in solving health problems in an approach to service that is hardly seen in other countries. The evidence easily seen is the prevalence of COVID-19 which the village health volunteers have an important role in monitoring, controlling, and preventing the spread of COVID-19 in their community. They are more accepted and have an important role in solving the contagious diseases occurring in the community. Thus, the health volunteer should gain knowledge, capability, and skills in performing their duty leading to functioning properly and effectively.
The effective learning process in developing the personnel’s knowledge and understanding leads to good performance which promotes the learners to learn through their previous knowledge by focusing on the learner center and participating in all activity processes leading to more knowledge and understanding consisting of 4 processes: (1) concrete experiment; sharing and exchanging the experiences, (2) reflection observation, (3) abstract conceptualization; concluding the main ideas gained from processes 1 and 2, followed by adding their knowledge and skill, and (4) active experiment; leading to actual practice. 3 To enhance the village health volunteers to fulfill their duty, they must have these 3 factors; (1) basic/functional health literacy (2) communicative/interactive health literacy, and (3) critical health literacy, 4 and 6 skills; (1) reaching health data and health service, (2) understanding health data and health service, (3) exchanging knowledge through questioning and answering, (4) making a decision on health, (5) adapting one own health behavior, and (6) telling health care prevention. The studies indicated that health literacy is related positively to health behavior. 5 Disease preventive behavior means the person’s practice in reducing the risk factor that causes the disease or the ailment with no symptoms in the belief of having good health. Health literacy had a positive relation to Covid-preventive behavior (r = .635, P ≤ .01). 6 health literacy related to preventing and controlling the dengue fever of the CHWs at the statistically significant level of r = .710, P ≤ .001. 7
CHWs participated in the experiential learning program, 5 they had more knowledge, working skill, and better performance behavior.8 -10 Developing the CHWs’s knowledge and experience through Kolb’s concept of preventing and curing the prevalence of emerging and re-emerging infectious diseases in their community effectively is one of the practical nurse’s duties. As a result of that, the residents in their community are free from emerging infectious and re-emerging infectious diseases of the respiratory system. The aim is to compare the mean score of literacy and preventive behavior in emerging infectious and re-emerging infectious diseases of the respiratory system of the CHWs participating in the experiential learning program before and after joining the program.
Method
It is quasi-experimental research, which is a 2-group pretest-posttest design, divided into 2 groups; an experimental group and a control group. The experiment takes 6 weeks as shown in Figure 1.
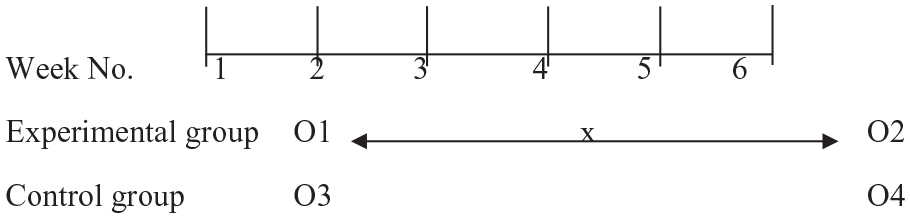
Research design.
Population and Sample
Population
The target populations applied in this research are 1321 CHWs working in 12 health promotion hospitals under the authority of Ngao Public Health Office, Lampang Province, and participating in the health care seminar which is a fundamental public health set up by the Ministry of Public Health.
Sample
The sample size is determined by analyzing the power of the test of Cohen (1992) 11 through G*power by setting up the parameter value for testing the 2-tail test hypothesis, the power of the test at 0.80, and the significant level at .05. From the estimation of the effect size value at 0.05, the sample size is 26 samples so the sample size is increased by 20% 12 to prevent the drop-out rate and the incomplete of the questionnaire using Gupta et al. 13 As a result, the total number of samples is 66 and 33 for each group; the experimental group and the control group. The experimental group participates in the experiential learning program for 6 weeks while the control group participates in a normal classroom. The experimental and control groups were selected using simple random sampling without replacement from the list of the CHWs working in sub-district health promotion hospitals.
Research Tools
A. The research tools
(1) Experiential learning program of the CHWs on literacy and preventive behavior toward the emerging infectious and the re-emerging infectious diseases of the respiratory system by using Kolb’s concept 5 divided into 4 steps;
Step 1 Concrete experiment, Step 2 Reflection observation, Step 3 Abstract conceptualization, and Step 4 Active experiment.
(2) The experiential learning program consists of (1) a PowerPoint on knowledge about the diseases and the prevention of emerging infectious and re-emerging infectious diseases, health literacy, data accessibility, and knowing the incidence of emerging and re-emerging diseases (2) A set of demonstrating equipment consisting of personal prevention equipment (PPE) and cleaning and eradicating equipment.
B. Data gathering tool (a questionnaire) comprising 3 parts as follows.
Part 1: General information—Sex, age, education, career, duration of being a volunteer, history of a seminar on emerging and re-emerging diseases, and ways of following the information.
Part 2: A 5-rating scale questionnaire consists of 38 questions adapted from the Department of Disease Prevention. The questions are about health literacy and health behavior on emerging infectious and re-emerging infectious diseases. The questionnaire validity following Cronbach’s alpha is .92.
Part 3: Questions on preventive behaviors about emerging and re-emerging diseases of the CHWs adapted from the questionnaire on the topic of preventive practice toward the 2019 Coronavirus disease of the CHWs by Wongcharoen et al 14 consisting of 2 main points; (1) using the personal preventing equipment and (2) cleaning the equipment and eradicating the waste. This questionnaire comprises 19 questions along with a 5-rating scale answer. Its validity value of Cronbach’s alpha is .89.
Data Collection Method
Data was collected as the following steps; After receiving the research ethical permission and the permission letter from the School of Nursing, University of Phayao, the researchers sent the letter to the Ngao sheriff to receive permission to collect the data in an area of Ngao District. Then, the research team collected the data in 6 weeks from February to March 2023.
Data Analysis
Data were analyzed using descriptive statistics; percentage, mean, and standard deviation, for personal data and studied variables, and inferential statistics; pair t-test—comparing in the group and independent t-test—comparing between the group, for comparing the mean score of preventing the emerging infectious and the re-emerging infectious diseases of the CHWs before and after participating in the program of the experimental group and the control group. Criterion interpretation 1 = lowest, 2 = low, 3 = moderate, 4 = high, and 5 = highest.
Results
Part 1: General Data
Most of the control group were females (87.90%), aged 51 to 60 years old (54.50%), with an average age of 52 years (SD = 7.47), education levels; high school/vocational certificate level (51.50%) and primary education level (36.40%), being a CHWs less than 10 years (60.60%). The majority joined in the seminar on emerging and re-emerging diseases in respiratory (60.60%) and had a channel to follow the information through the internet (39.40%), followed by the public health official (33.30%). In the experimental group, the majority were females (93.90%), age 51 to 60 years old (56.00%), an average age 51.00 years (SD = 6.12), education level high school/vocational certificate level (51.50%) and primary education level (42.40%), being a CHWs less than 10 years (60.60%). The majority joined in the seminar on the emerging and re-emerging diseases in respiratory (87.90%) and had a channel to follow the information through the public health official (39.40%) followed by television (36.40%). When comparing the personal data between the 2 groups, it showed that there was no statistically significant difference (P > .05).
Part 2
Comparison of the mean score of literacy and preventive behavior toward the emerging infectious and the re-emerging infectious diseases of the respiratory system of the CHWs participating in the experiential learning program.
According to Table 1, the experimental group had a higher mean score of literacy and preventive behavior on the prevention of emerging infectious and re-emerging infectious diseases of the respiratory system of the CHWs after participating in the program higher than before participating in the program statistically significant difference of P < .001.
Comparison of the Mean Score of Literacy and Preventive Behavior Toward the Emerging Infectious and the Re-Emerging Infectious Diseases in the Respiratory System of the CHWs in the Experimental Group Before and After Participating in the Program (n = 33).

Regarding Table 2, the experimental group had a mean score of literacy on the prevention of emerging infectious and re-emerging infectious diseases of the respiratory system before participating in the program overall at a high level (
Mean Score, Standard Deviation, and Score Level of Literacy and Preventive Behavior on the Emerging Infectious and the Re-Emerging Infectious Diseases of the CHWs Between the Control Group and the Experimental Group Before and After Participating in the Experiential Learning (n = 66).
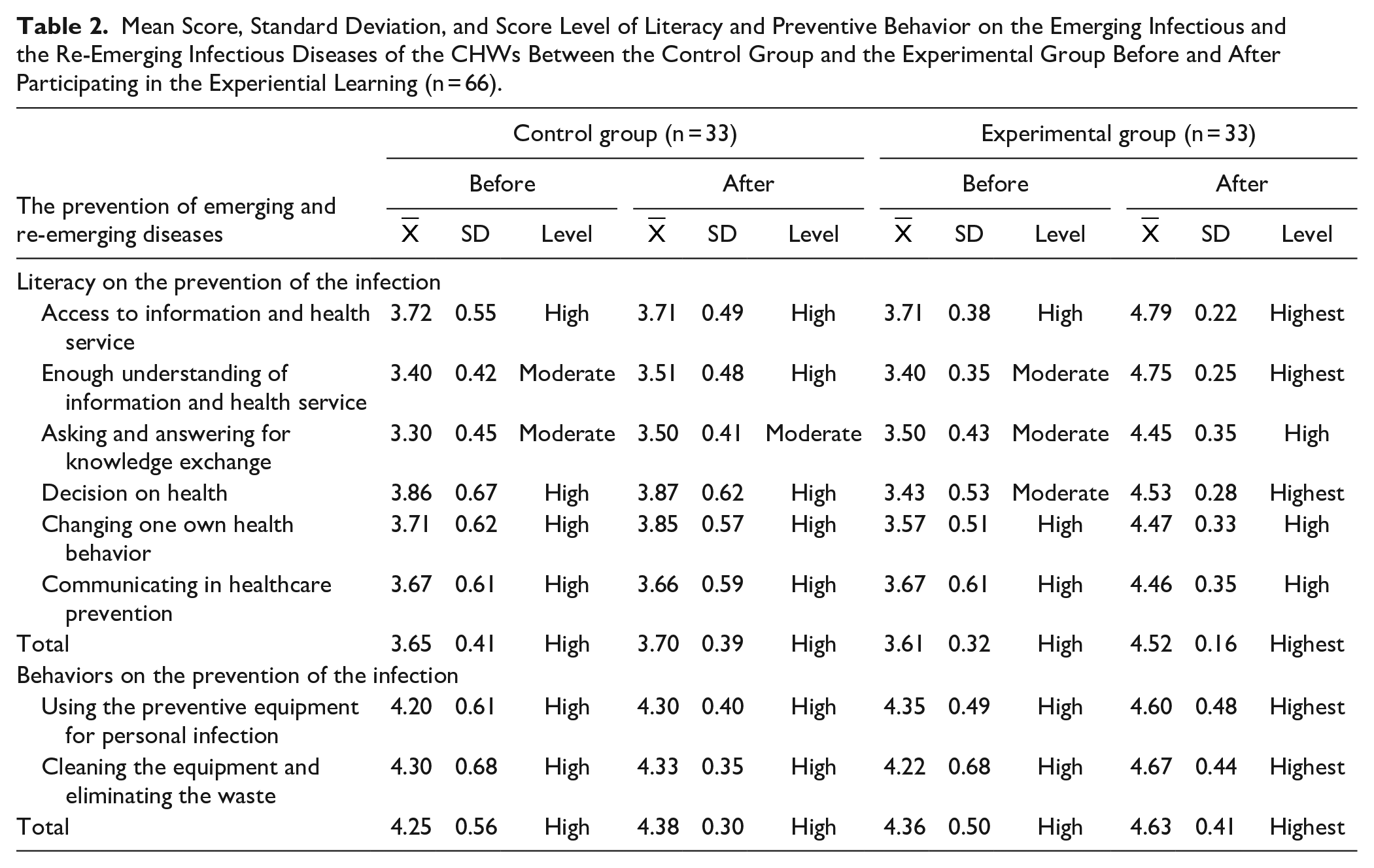
For Table 3, the experimental group had a mean score of literacy on the prevention of emerging infectious and re-emerging infectious diseases of the respiratory system of the CHWs after participating in the program higher than before participating in the program at a statistically significant difference of P < .001.
Comparison of the Mean Score of Literacy and Preventive Behavior Toward the Emerging Infectious and the Re-Emerging Infectious Diseases in the Respiratory System of the CHWs Between the Control Group and the Experimental Group (n = 66).

Discussion
Comparison of the Mean Score of Literacy Toward the Prevention of Emerging Infectious and Re-Emerging Infectious Diseases of the Respiratory System of the CHWs
The comparison result of the mean score of literacy in the prevention of the emerging infectious and re-emerging infectious diseases of the respiratory system of the CHWs before and after participating in the program, indicated that the mean score of literacy was higher than before participating in the program at the statistical significance at P < .001 and between the group it showed that the group participating the program had the mean score of the literacy in the prevention of the emerging infectious and re-emerging infectious diseases of the respiratory system higher than the non-participating group at the statistical significance P < .001 which could explain that the experiential learning is a way of learning through the practice focusing mainly on the role and the learner’s participation or active learning leading to gaining the knowledge from his or her experience. Experiential learning is a process that the Department of Health suggests using as a way to promote health literacy. 15 It is believed that learning through the learner’s experience together with participatory learning and familiarity with health services and systems will result in higher health literacy.16 -18
Thus, bringing the experience in the prevention of the prevalence of the infectious disease occurring in the community to be the basis in promoting the CHWs to have more knowledge in the emerging infectious and re-emerging infectious diseases in respiratory. The experiential learning process concentrates on the CHWs’s learning center. Also, the researcher uses the group process in the program to make the volunteers discuss among the group by exchanging their previous ideas and experiences to analyze the infectious incidence in the community properly and effectively leading to the conclusion and concept. This concept is the main factor in developing literacy and understanding the problems occurring in the community. 5 Develop the learners to have complex and creative ideas, and understand the content and apply them properly. 5 It is seen that these concepts and experiences come from the learner center. Thus, after participating in the experiential learning program, the CHWs have more literacy about the emerging infectious and re-emerging infectious diseases in the respiratory
Comparison of the Mean Score of the Preventive Behavior Toward the Prevention of the Emerging Infectious and the Re-Emerging Infectious Diseases of the Respiratory System of the CHWs
The comparison of the preventive behavior in the emerging infectious and the re-emerging infectious diseases of the respiratory system of the CHWs of the experimental group indicated that after participating in the experiential learning program had a mean score higher than before joining the program at the statistically significant at P < .001). When comparing the participating group and the non-participating group, it showed that after participating in the experiential learning program, the participating group had the mean score of the preventive behavior on the emerging infectious and the re-emerging infectious diseases of the CHWs higher than the non-participating group at the statistical significance at P < .001. It could be explained that the experiential learning concept 5 contained in the program consisted of the experiential steps as follows; reflection and discussion, conceptual conclusion, and experimental practice. Giving knowledge, and developing the skill were put into any step of learning and also conformed to the role and duty of the CHWs leading to good practice in terms of correctness and proficiency. Ultimately, the CHWs had self-confidence in developing their potential as much as possible. Besides, the program had 3 activities (1) knowledge development (2) skill development through demonstrating from the researcher and then giving feedback to the sample group (3) working in the community, it found that giving knowledge to the sample group through learning by doing could make them know how to prevent the COVID-19 infection and related to their preventive behavior of the volunteers at the statistical significance P < .001.14,19,20 Besides, it still found that health literacy correlated with health behavior leading to having more preventive behaviors.20 -22 and also found that health literacy correlated with the preventive behavior of COVID-1923-25 which was the emerging disease in the respiratory system. It is believed that if the CHWs have good literacy and preventive behavior toward emerging infectious and re-emerging infectious diseases, they can reduce their risks of infecting the disease while performing their duty.
Conclusions
The experiential learning program can be brought to develop the CHWs in preventing diseases. This is because learning through the learner’s experience together with participatory learning and familiarity with health services and systems will result in higher health literacy and skill. The skill development through the demonstration and feedback demonstration, along with performing the real practice in their community makes them have better literacy and preventive behavior. The research results could be a guideline for developing the CHW’s potential effectively and proficiently.
Implications
The health officials and the involved sectors/stakeholders can bring the result of the experiential learning program of the CHWs toward literacy and preventive behavior toward the emerging infectious and the re-emerging infectious diseases of the respiratory system of the CHWs in preventing the infection from functioning their duty and people in the community.
Footnotes
Acknowledgements
Special thanks to CHWs working in 12 health promotion hospitals under the authority of Ngao Public Health Office, Lampang Province, and the medical staff in Ngao Public Health Office, Lampang Province, for participating in the health care seminar which is a fundamental public health set up by the Ministry of Public Health.
Author Contributions
Conceptualization: Neeranuch and Dao; Methodology: Dao and Neeranuch; Formal analysis and investigation: Neeranuch, Dao, and Thapkwan; Writing—original draft preparation: Neeranuch; Writing—review and editing: Neeranuch and Dao; Funding acquisition: Dao and Neeranuch; Resources: Pitakpong, Kiattisak, Jutapong, and Tanawat Supervision: Neeranuch.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Right Protection of the Informants: This research was permitted in human research ethics from the University of Phayao on November 2022, No. UP-HEC 1.2/020/66.
Consent to Participate
The researcher explained the research objective, the research method, and the research outcome to the CHWs and signed a consent form. All data were kept in a safe place and destroyed after the publication of the research results and only the research team could reach the data.
Consent for Publication
Informed consent documents included explicit consent for the sharing and use of de-identified quotes in publications.
Availability of Data and Material
Data are available upon reasonable request to the corresponding author.