
Abstract
Chronic kidney disease (CKD) is a significant threat to the quality of life of the global population. Thus, slowing kidney disease progression is considered vital in the treatment of CKD patients. The study aimed to evaluate the effectiveness of a program designed to slow the progression of CKD among Type 2 diabetes mellitus patients with HT with stage 3 CKD (CKD 3) in Thailand by adopting the information-motivation-behavioral skills (IMB) model and applying technology. This study was conducted as a cluster randomized controlled trial. The program activities comprised: (i) providing disease information and teaching behaviors to slow the progression of kidney disease to patients and family members via a 2-h session; (ii) teaching practical behavioral skills for appropriate diet and exercise to patients and family members via a 2-h session; (iii) enhancing personal motivation via the Line application and motivational interviewing via telephone calls; (iv) enhancing social motivation with the support of a family member; (v) employing technology to monitor behaviors and increase patient motivation; and (vi) assessing behaviors that were not practical, exploring barriers to behavior modification, and teaching further practical behavioral skills via the Line application. The data were analyzed using percentages, means, standard deviations, chi-square tests, t-tests, and a 2-way repeated-measures analysis of variance. The results showed that after the experiment, the experimental group had significantly higher mean scores in terms of knowledge, perceived benefits, perceived severity, self-efficacy, and behaviors to slow the progression of kidney disease than the control group (P < .05). Further, the experimental group had significantly better clinical outcomes (SBP, DBP, eGFR, BUN, creatinine, albuminuria, FBS, and HbA1c) than the control group (P < .05). In summary, the findings indicate that the program improved clinical outcomes, especially kidney function, effectively slowing the progression of kidney disease.
Keywords
Introduction
Chronic kidney disease (CKD) is a serious global health problem that significantly contributes to morbidity and mortality rates. According to the global mortality rate report in 2017, 1.2 million deaths were directly related to CKD in 2017, an increase of 32% compared to CKD-related deaths in 1990. Prevalence of CKD stage 3 to 5 increased with age, estimated prevalence was 8.9% in 30 years and increased to 27.9% in 70 years. 1 In treating chronic renal patients with end-stage renal failure, the following procedures require peritoneal dialysis, hemodialysis, or kidney transplantation. 2 The lives of CKD patients and families are affected both physically and mentally, which profoundly impacts their overall quality of life.2,3
Various factors contribute to the decrease of kidney function, of which, the most common are diabetes and high blood pressure. Among patients with chronic kidney failure, 67 to 93% have hypertension. Among patients with stage 3 CKD (CKD 3), those with diabetes were 1.87 times more at risk and those with high blood pressure were 1.6 times more at risk, and the rate of CKD was 43.5% in diabetic patients, and 61% in diabetic patients aged 65 years and older. 1 Thus, treating the complications of diabetes and high blood pressure in patients with CKD is crucial in reducing the rate of kidney deterioration among such patients.
The literature review revealed that most of the programs that aim to slow CKD progression promote self-care behaviors, and the majority of educational activities revolve around disease progression, treatment, the prevention of complications, blood sugar control, blood pressure control, and lifestyle changes.4 -6 The focus was on organizing activities for patients that are designed by researchers. However, there is a lack of patient participation in the process of designing activities that were tailored to patients’ needs, and there is also a lack of family involvement and interactions with patients.
Family members provide essential support to CKD patients. Indeed, family members provide management, such as coordination, the pursuit of expenses, and psychosocial support. Family members also provide care according to treatment plans (eg, appropriate disease dietary support, medication regulation, and weight control), ensure CKD patients exercise, and respond to patients’ physical, mental, social, and economic needs to maintain their quality of life.4,7,8 Thus, it is important to provide specific information to increase knowledge, especially knowledge that could increase crucial behavioral skills, and to increase personal and social motivation and family participation to support appropriate behavioral modifications to slow the progression of CKD. This study sought to achieve this using the information-motivation-behavioral skills (IMB) model.
Currently, technology plays a significant role in the daily lives of people and provides people with the ability to access information. As an optional tool, technology can also increase the efficiency of information provision, enable the tracking of patients’ conditions, encourage behavioral modification, 9 provide more rapid and fluid access to services, improve communication between providers and patients, 10 and enable patients to manage themselves to some extent and monitor their own condition to sustain healthy behavioral options. 11 In Thailand, a senior group used the Line application daily to communicate with their families and friends. 12 This elderly group was quite comfortable and familiar with the use of technology and the internet, which allowed them to monitor current events, find health information, and access optional therapies. 13 Thus, technology has been shown to enable communication between health personnel and patients, increase motivation for behavioral modifications, enable patient care results to be monitored, and improve the overall quality of healthcare services.
This study sought to evaluate the effectiveness of a program in slowing the progression of CKD among Type 2 diabetes mellitus (T2DM) patients with HT with Stage 3 CKD (CKD 3) in Thailand by adopting the IMB model and applying technology. The program aimed to prevent patients from entering stage 5 CKD, reduce the effect on the lives of patients and their families, lower the burden of costs for renal replacement therapy, and, most importantly, improve the quality of life of patients.
Materials and Methods
Study Design
A cluster randomized controlled trial with a two-group, pre-post test design was conducted. Thai clinical trials registry identification number is TCTR20230830001 (https://www.thaiclinicaltrials.org/show/TCTR20230830001).
Sample and Study Eligibility
In this cluster randomized controlled trial, 6 districts in the Samutprakarn province, Thailand, were randomly allocated to the experimental and control groups. Patients were randomly selected from patient lists in the sub-district health promoting hospitals if they had been diagnosed with diabetes and/or hypertension with CKD 3 failure complication (GFR 30-59 ml/min/1.73 m2), were aged 40 to 70 years, had blood pressure >140/90 mmHg at least once in the last 6 months, had HbA1C > 7% in the last 6 months, were able to communicate, read, and write in Thai, lived with their family, and had no complications or severe illnesses during the study that might have caused any obstacle to activity participation.
Participant Recruitment Into Study Groups
The sample size for this study was calculated by G* Power 3.1.9.4 based on a previous study by Jiamjariyapon et al. 14 The power of analysis was .95, the error type I was .05, and the effect size was .80. The minimum number of the sample size for each group was 35 patients. For this study, the calculated sample size was inflated by 10% to compensate for potential missing data or drop outs. Thus, the sample size was 38 patients for each group. In total, 76 patients with diabetes and hypertension with CKD 3 complication (GFR 30-59 ml/min/1.73 m2) were assigned to the following 2 groups: 1) the experimental group (n = 38); and 2) the control group (n = 38). On-site computer systems were used to allocate concealment. The CKD 3 patients in the experimental group participated in the program to modify the risk factors to slow the progression of kidney disease. The patients in the control group received the usual care. The study ran over a 14-week period.
Study Measures
A number of research measurement tools were used in the study.
Program to slow the progression of CKD in the community
The program activities comprised: i) providing disease information and teaching behaviors to slow the progression of kidney disease to patients and family members via a 2-h session; (ii) teaching practical behavioral skills for appropriate diet and exercise; (iii) enhancing personal motivation via the Chatbot in Line application and motivation interviewing via telephone calls; (iv) enhancing social motivation with the support of a family member via the Line application; (v) employing technology to monitor behaviors and stimulate patient motivation; and (vi) assessing behaviors that were not practical, exploring barriers to behavior modification related to the repetition of knowledge and motivation, and teaching further practical behavior skills via the Line application (see Figure 1).
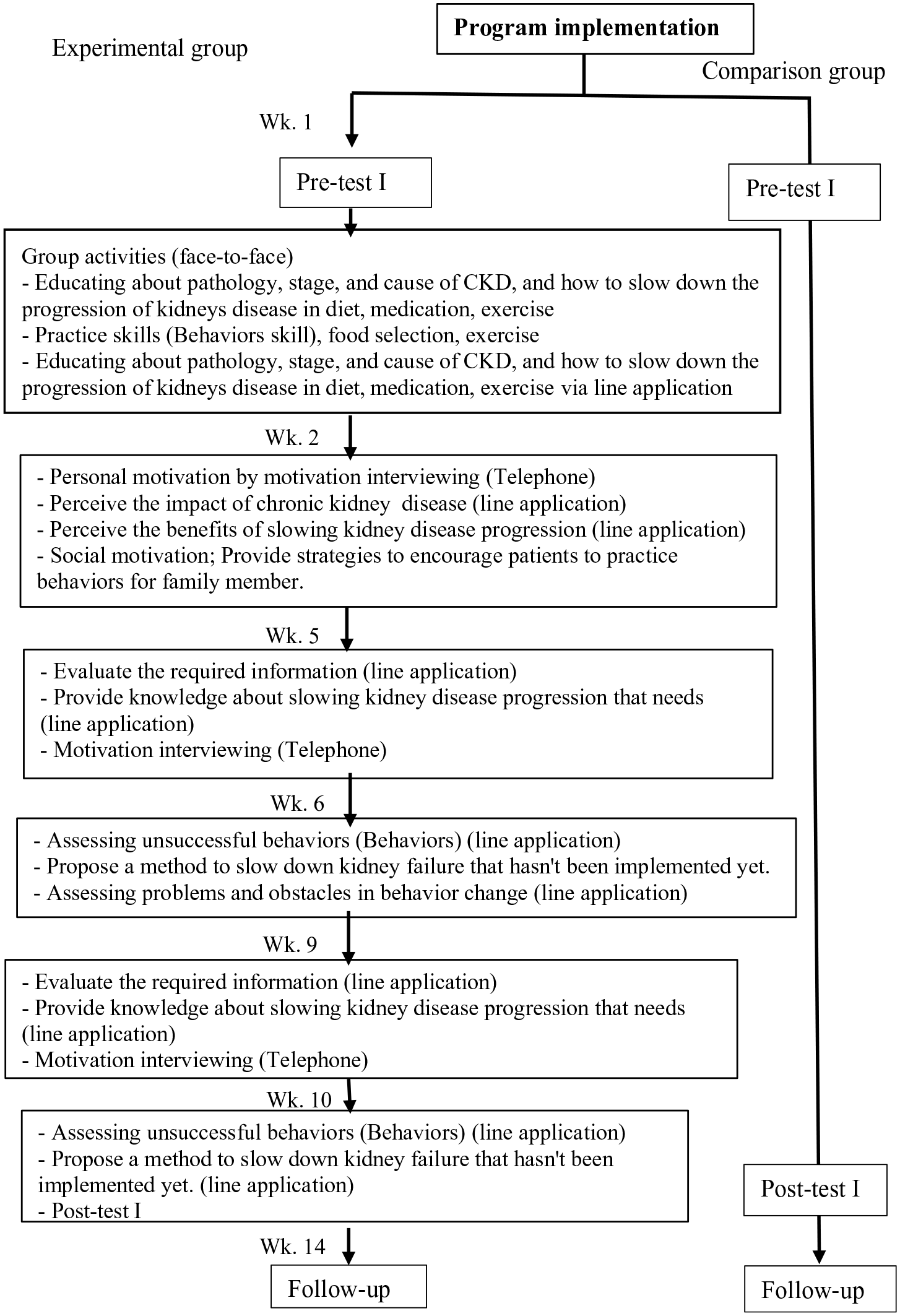
Flow diagrams of a comparison between the experimental group and the comparison group in program implementation.
Questionnaires
The questionnaires were designed to gather general demographic data, and data on patients’ knowledge of pathology and CKD progression, patients’ perceptions of the benefits of behavior modification in slowing the progression of the kidney disease, patients’ perceptions of the disease severity of the kidney disease, patients’ perceptions of their self-efficacy in slowing the progression of the kidney disease, and patients’ perceptions of their behaviors in slowing the progression of the kidney disease (dieting behavior, exercises, and medication usage). In terms of the questionnaires, the reliability of patients’ perceptions of the benefits of behavior modification in slowing the progression of the kidney disease was 0.93, that of patients’ perceptions of the severity of the kidney disease was 0.80, that of patients’ perceptions of their self-efficacy in slowing the progression of the kidney disease was 0.85, and that of patients’ perceptions of their behavior in slowing the progression of kidney disease was 0.80. The researcher test reliability by applying the KR-20 of questionnaire on knowledge to slowing the progression of the kidney disease was 0.86. The instruments for evaluating all parts of this research had a CVI of 1. The pre- and post-experimental questionnaires were administered before the experiment, and at weeks 10 and 14.
Data collection and analysis
The data were collected and analyzed using descriptive statistics (e.g., percentage, mean, and standard deviation [SD]), chi-square tests, t-tests, and a 2-way repeated-measures analysis of variance.
Ethics approval
Ethics approval was obtained from the Ethics in Human Research Committee, Faculty of Public Health, Mahidol University Patients meeting (MUPH 2021/024). The researcher also submitted the research project proposal to the Ethics in Human Research Committee, Samutprakarn District Public Health Offices.
Results
Table 1 sets out the background characteristics of the patients. In the experiment group, there were more women than men (76.30 and 23.70%, respectively) and more patients aged 60 to 70 years than 50 to 59 years (89.50 and 7.90%, respectively). The majority of the patients in the experimental group were Buddhists (94.70%). Among the patients, 78.90% were married and 13.20% were divorced.
Socio-Demographic Characteristics of Patients in the Experiment and Comparison Groups.

t-Test.
Chi-square test 2-sided.
Table 2 sets out the results after the experiment and during the follow-up period. The patients who received the intervention had significantly better knowledge of how to slow the progression of kidney disease (MD = 6.18, SD = 3.57 and MD = 7.60, SD = 3.43, respectively), perceive the disease severity of the kidney disease (M = 36.97, SD = 4.92 and M = 39.47, SD = 2.15, respectively), perceive benefits of behavior modification in slowing the progression of the kidney disease (M = 37.15, SD = 4.47 and M = 39.52, SD = 1.88, respectively), self-efficacy in slowing the progression of the kidney disease (MD = 9.52, SD = 8.75, MD = 14.3, SD = 10.04, respectively), and behaviors in slowing the progression of kidney disease (M = 4.28, SD = 12.89 vs M = 12.44, SD = 14.37 respectively) than the control group (P < .001).
Comparison of Outcomes Between Groups Before the Experiment, After the Experiment and the Follow-Up Period.

Mean difference.
P-value < .001.
Clinical Outcomes
The clinical outcome results are set out below.
From Table 3, it was found that the resulting in clinical outcomes as follow,
Compare Clinical Outcomes Between Experiment and Comparison Group.

P-value < .05.
Nutrition stage
The mean BMI of the patients in the experimental group was lower during the follow-up period than before the experiment and lower than that of patients in the control group (M = 24.88, SD = 4.26).
Blood sugar
The mean FBS and HbA1c of the patients in the experimental group were lower during the follow-up period than before the experiment and were lower than that of patients in the control group (M = 108.00, SD = 17.94 vs M = 6.62, SD = 0.58 respectively) (P < .001).
Blood pressure
The mean SBP and DBP of the patients in the experimental group were significantly lower during the follow-up period than before the experiment and were lower than that of patients in the control group (M = 120.42, SD = 13.53 vs M = 64.18, SD = 8.25, respectively) (P < .001).
Kidney function
The kidney function mean (eGFR, BUN creatinine, and albuminuria) of the patients in the experimental group during the follow-up period differed significantly to the mean of these patients before the experiment and to the mean of the patients in the control group (M = 54.65, SD = 8.65, M = 16.61, SD = 5.99, M = 0.93, SD = 0.23, M = 77.63, SD = 74.05, respectively) (P < .001).
Discussion
Slowing down kidney disease progression is directly related to behavior modifications by patients. 1 The program used in this study was based on the IMB model and combined with the application of technology. The researcher extracted information specific to kidney disease patients, including information on the causes of kidney disease and information on the proper care of patients with CKD. The information included essential and specific information on the type and amount of food that should be consumed daily, including protein, sugar, sodium, fat, potassium, and phosphorus, and example menus for kidney disease patients. This is consistent with andragogy (i.e., self-directed learning). In this program, the specific information on CKD was also related to the patients’ attention and learning. Enhancing patients’ personal motivation by increasing their perceptions of disease severity and their perceptions of the benefits of behavior modification in slowing the progression of kidney disease can strengthen the effects of chronic kidney disease among patients and their families, including physical, psychological, and socio-economic aspects and benefits of slow chronic kidney progression for patients and their family. 15 In addition, support from family members can motivate patients to modify behaviors. In Asian culture, family members play a vital role in promoting health and wellness. 7
The strategy also included motivational interviewing via telephone calls based on a brief advice process to help the patients resolve any hesitations by eliciting their intrinsic motivation as a personal motivation, supporting self-efficacy, and encouraging their commitment to change their behavior by adhering to the patients as the center. In addition, the behavior skills training activity that sought to increase patients’ perceptions of self-efficacy included: 1) demonstrating how to measure amounts of food and seasonings using a spoon, teaspoon, and tablespoon, and how to choose food for protein, sodium, fat, sugar, and potassium using natural food proportions; 2) having patients and family members select food menus and practice skills for selecting raw materials for cooking, and measure the amount of food and seasonings and food exchanges; and 3) practicing exercise skills. The patients and family members practiced their exercise skills and demonstrated reversal. 6 The distinct features of the program delivery might have also increased behaviors to slow the progression of CKD in the experimental group after the experiment and during the follow-up period, and the experimental group performed better than the control group.
Our findings showed the importance of public health messages and highlighted the program’s benefit in slowing the progression of CKD. The program that sought to provide patients with knowledge specific to kidney disease was designed using data related to the original behaviors, lifestyles, and cultures of the patients, and used images to highlight infographics, concise and easy-to-understand text and photographs, and exciting and easy-to-remember illustrations, and was sent via the Line application to continuously motivate behavior modification. Questions were asked after every infographic knowledge session with multiple-choice answer options and immediate feedback was provided to assess the patients’ understanding, increase patients’ perceptions of their self-efficacy, repeat knowledge, motivate, and further increase their practical behavior skills to slow the progression of CKD. The results was consistent with the study by Timmerman et al 6 on improved knowledge to manage weight, the basics for a healthy heart diet, and dietary recommendations for CKD.
The current study provides evidence that interventions based on established behavior-change strategies, including methods for overcoming expected reported clinical outcome effects, can slow the progression of CKD. The typical primary sources are diabetes and high blood pressure. Hyperglycemia causes glomerular and tubulointerstitial injury, ultimately leading to glomerulosclerosis. Moreover, hypertension can generate chronic kidney complications, resulting in ischemic glomerulus and eventual glomerulosclerosis. Other factors that cause a continuous decrease in kidney function include protein, sugar, sodium, fat, potassium, and phosphorus. 1
This study’s application of technology via the Line Official application to provide care to CKD patients helped to facilitate communication between health personnel and patients and encouraged patients to engage in autonomous self-care as appropriate. Emphasizing self-care via technology is a vital component and can be woven into the context of a patient’s daily life to address their specific needs and disease characteristics to promptly provide information about disease prevention, monitoring, and behaviors. In addition, increasing CKD patients’ knowledge, perceptions of disease severity, perceptions of the benefits of behavior modification, and perceptions of their self-efficacy in slowing the progression of the kidney disease tend to involve relatively intensive behavioral changes to control the amount of dietary protein, sugar, sodium, fat, potassium, phosphorus, and exercise; however, such strategies are critical in improving blood sugar and blood pressure and thus improving kidney function, which can slow down kidney deterioration, and postpone the period of end-stage renal failure. 16 In accordance with Chaiyasung et al, 17 they organized activities to promote self-care in chronic kidney disease patients by applying the concept of self-care in combination of knowledge and self-care practice for CKD patients and family support.
Conclusions
Guidelines for caring for patients with CKD integrate care with health personnel, patients, and family members and reinforce a system of self-care that allows patients to change their behaviors, resulting in better care outcomes. Health professionals who provide services for CKD patients, including those with comorbidities, must be able to assess their care needs promptly, which requires continuing, designed education programs that focus on controlling chronic care. Providing this continuing education via a mobile telephone appears to be an effective way of increasing the positive effects on their disease control and their ability to continue to live with their own families, increasing chronic care professionals’ ability in this area. However, due to the limited research in this area, more research needs to be conducted to evaluate the effectiveness of mobile health, particularly in the field of chronic care evaluation in the community care of patients with CKD. Healthcare organizations, education organizations, and researchers must work together to ensure that chronic care professionals are able to apply technology in care services. Technology for chronic care should be embedded in curricula and continuing education programs.
Footnotes
Acknowledgements
The authors thank the patients who generously participated in this study. We would also like to thank the staff at the study’s sub-district health-promoting hospitals for their cooperation during the data collection period.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported by Praboromarajchanok Institute, Thailand.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.