
Abstract
Objectives:
To identify the proportion of young people experiencing homelessness who are immunized against vaccine-preventable diseases, and to evaluate the impact of a nurse-led immunization program to improve vaccination coverage in this population.
Methods:
A retrospective audit of electronic medical records included 400 participants aged 15 to 24 years who had an encounter with the Young People’s Health Service, a nurse-led clinic co-located with a specialist youth homelessness service in Melbourne, Australia, between February 2019 and May 2021.
Results:
Integrating an immunization nurse within a youth specialist homelessness service increased the percentage of young people who were up-to-date with routine vaccinations from 6.0% (n = 24) to 38.8% (n = 155). Intersecting social determinants of health that increased participants’ risk of vaccine preventable diseases, and of missing routine vaccines, were common.
Conclusions:
Incomplete coverage of routine vaccines is common in young people accessing homelessness services, and this coverage was improved when young people encountered an immunization nurse while accessing support from a specialist youth homelessness service. As a service model, nurse-led community health clinics co-located within homelessness providers can improve vaccination coverage, and therefore health outcomes, of young people experiencing or at risk of homelessness.
Introduction
Just over 53 000 young people aged 15 to 24 years accessed Australia’s Specialist Homelessness Services (SHS) in 2021-2022, of whom around 75% were unaccompanied. 1 Defined as young people who live in non-conventional accommodation (such as living on the street or “sleeping rough”), short-term temporary or emergency accommodation (such as staying in supported accommodation for the homeless, or “couch-surfing”) or in living arrangements that do not allow them to have control of, or access to space for social interactions (eg, in severely crowded dwellings), homelessness is correlated with a higher risk of mortality and morbidity.1,2 This relationship reflects complex intersections with health conditions and social determinants including disruptions to schooling, financial insecurity, and mental health disorders.3 -9 At the same time, these young people disproportionately engage in health risk behaviors (such as substance use) and are at increased risk of communicable diseases.3,5,10 Feelings of stigma and shame, and almost universal experiences of adverse childhood events, contribute to avoidance or delay in seeking health care.3,10 Previous negative experiences with health services are also common and harmful. 10 In this context, routine vaccinations (those that are recommended and funded as major public programs of the state and national government) are likely to be of low priority to young people at risk of homelessness and their service providers. 11
Both Australia and the United States of America (USA) boast strong population coverage for routine childhood and adolescent vaccines, and prioritize improving immunization coverage of populations at high risk of vaccine-preventable diseases (VPDs) and in areas with low vaccine coverage as part of their national strategies.11,12 In the USA, a federal entitlement program provides free vaccines to children who are eligible for Medicaid, differing slightly from Australia where all children are eligible for routine vaccines under the National Immunisation Program (NIP) and state (and territory) based programs.11,13 The Australian Immunisation Register (AIR), a nationwide database that reports vaccine coverage by postcode, suggests young people from the most advantaged suburbs of Australia have as much as a 13.2 percentage point higher course completion rate of the Human Papillomavirus (HPV) vaccine than those living in the least advantaged areas.14,15 However, determining the vaccination coverage of people accessing specialist homeless service is not discernible using the AIR, resulting in an unknown rate of vaccination coverage in young people experiencing homelessness.
Most research into routine vaccination coverage in children and young people experiencing homelessness is from the USA. 16 In Pennsylvania, only 37.2% of adolescents accessing a crisis housing service were up to date with scheduled vaccinations. 17 Across 7 cities in the USA, between 19% and 37% of youth experiencing homelessness were up to date with HPV vaccination. 18 Existing studies are often limited by the availability of records and sometimes rely on participant recall, which is recognized as an unreliable method of ascertaining vaccination status.16,19 A search of the scientific literature did not reveal any comparable Australian studies. Beyond routine vaccination, there is also some literature detailing largely reactive responses to vaccinating people experiencing homelessness during acute infectious disease outbreaks such as COVID-19, hepatitis A and B, and influenza.20 -26
Young people experiencing homelessness are not recognized as an “at-risk” group for missing routine immunizations in Australia’s National Immunisation Strategy, despite being a priority population in Australia’s National Action Plan for the Health of Children and Young People.9,11 This action plan, amongst other guidance, promotes co-located clinics as a mechanism to improve health equity across populations, with expectations that the structure of services in co-located clinics (e.g., model of care, health professional skills and attitudes, and young people’s knowledge of services) enhance access, engagement and navigation of health and social systems.5,8 -10,27 The Young People’s Health Service (YPHS) is an example of a co-located, nurse-led community clinic that aims to advance the health of young people experiencing homelessness in Melbourne, Australia. This service was established in 1991 following recommendations from the Burdekin Report, Australia’s first national enquiry into child and youth homelessness, that health services for young people should be free, youth-focused, and integrated with other homeless services. 8 In 2019, YPHS received funding from the Victorian Government for a pilot project to embed an immunization nurse within the service.
This research set out to evaluate if a nurse-led clinic was a practical solution to improving vaccine uptake as a measure of health equity. The primary objective of the study was to identify the proportion of young people experiencing homelessness who were protected against VPDs when first seen. Secondly, we sought to evaluate the impact of a nurse-led immunization service to improve vaccination coverage in this group. Health risk factors and social determinants of health were collated to further understand the population’s risk of VPDs.
Methods
The YPHS is a program of the Royal Children’s Hospital, Melbourne, Department of Adolescent Medicine. It is co-located with Frontyard Youth Services (Frontyard), a state-wide crisis housing access point for young people aged 15 to 25 years run by the Melbourne City Mission. The YPHS is staffed by a nurse practitioner, advanced practice nurses, administrative staff, and rotating hospital medical officers. Young people can drop-in to YPHS, be referred through Frontyard, or be seen on an outreach nursing visit at various youth refuges and flexible learning centers in Melbourne.
In 2019, YPHS established a nursing role to champion vaccines through direct patient care, consultancy to health and homelessness providers, and coordination of outreach clinics. When a young person was referred to YPHS, the immunization nurse assessed immunization status, developed a catch-up vaccination plan if needed, and when possible offered appropriate vaccines at that visit. At least three recall attempts (phone, SMS, and/or email) were made to contact patients for further appointments as required. If those contact attempts failed, a note was left in their Frontyard file that they were due to see the health team if they dropped in.
The eligible study population consisted of 948 people between 15 and 24 years old who had an encounter with a YPHS clinician documented on the RCH electronic medical record (EMR) between February 2019 and May 2021. This period allowed for time to complete immunization catch-up plans up to 12 months after the last attendance in May 2021. The age range reflects the age of young people eligible to access YPHS. Within the time and resources available, a retrospective EMR audit was undertaken (by BT) of 400 individuals (the sample). Case selection was done at random and all individuals had equal chance of being included. Data were entered into the REDCap database system and 10% of data extraction was cross-checked by another investigator (DH).28,29
A list of relevant risk-factors for VPDs and relevant social determinants of health (Tables 1 and 2) was adapted from 3 sources: the Australian Institute of Health and Welfare; the Australian Immunisation Handbook, “Vaccinations for Special Risk Groups”; and the National Centre for Immunisation Research and Surveillance (NCIRS), “Adult Vaccination Fact Sheet.”30 -34
Demographic Details of Participants (n = 400).

Includes “youth foyers” (where young people are provided with accommodation for 1 to 3 years if they are studying) and youth residential rehabilitation programs (where young people with mental health issues and homelessness are provided with supported accommodation for 12 months).
Social Determinants of Health, Health Risks, and Special Risk Groups That Place Young People Experiencing Homelessness at Greater Risk of Vaccine Preventable Diseases.

Vaccine coverage was assessed at initial contact with the immunization nurse until the end of May 2022 (12-36 months after their initial contact). Participants were considered up-to-date if they did not require any catch-up vaccines following review of the AIR by the immunization nurse. Some participants missed childhood vaccines which did not require catch-up vaccination in adulthood (reported separately in the results).
Descriptive data collected from the EMR included any reasons that participants provided for not receiving a vaccine offered by YPHS, or for not completing the catch-up schedule before the end of the study period. The number of visits required to complete vaccination, the number of recall attempts, and the length of time to complete the vaccination plan were also recorded.
Data analysis was conducted in Stata version 16.1. 35 Descriptive data are presented as numbers and proportions. Health risks and social determinants were reported as binary variables (yes/no) and in addition to the number and proportion, a total value was calculated to provide the mean number and standard deviation (SD). Vaccine coverage data were reported by vaccine as the number and proportion that required catch-up at their initial contact with YPHS, and at the end of the study period (May 2022).
This retrospective audit was prospectively registered with ClinicalTrials.gov (ID NCT0484678). Ethics approval was obtained from The Royal Children’s Hospital Human Research Ethics Committee. Informed consent was not required and confidentiality requirements were upheld.
Results
The sample consisted of 400 young people. The majority (68%, n = 272) were referred to YPHS from Frontyard, were born in Australia (76%, n = 303), and aged 18 to 24 years old (76.5%, n = 306). Five percent (n = 20) reported never attending secondary school, 35.5% (n = 142) reported leaving school in the early secondary years and 11.8% (n = 47) had completed the final year of secondary school (Year 12 or equivalent). Close to 50% (n = 192) were awaiting crisis housing support at their initial contact with YPHS (see Table 1).
Table 2 reports the proportion of participants with various social determinants, personal behaviors and population risks that increase the risk of VPD. The most common factor was disengagement from mainstream schooling (77%, n = 307). Substance use was common, including intravenous (13%, n = 52), and non-intravenous use (56%, n = 223). A small percentage (3.5%, n = 14) of the sample were known to be living with HIV, hepatitis B or C. Young people attending the service had an average of 3 factors that increased their risk of VPD, or of missing out on routine vaccines.
Initial assessment revealed that 94% (n = 376) of participants were not up to date with vaccines and required a catch-up vaccination plan (Table 3). Most commonly, the Varicella vaccine was missing (73% required vaccination), followed by the adolescent dose of Diphtheria, Tetanus and Pertussis (dTpa) (56% required catch-up), and Meningococcal ACWY (68% required catch-up).
The Change in the Number (%) of Participants Who Were Up-to-Date at Initial Contact, Who Were Found Not to Need Specific Vaccines, and Who Were Up-to-Date by the End of the Study Period.
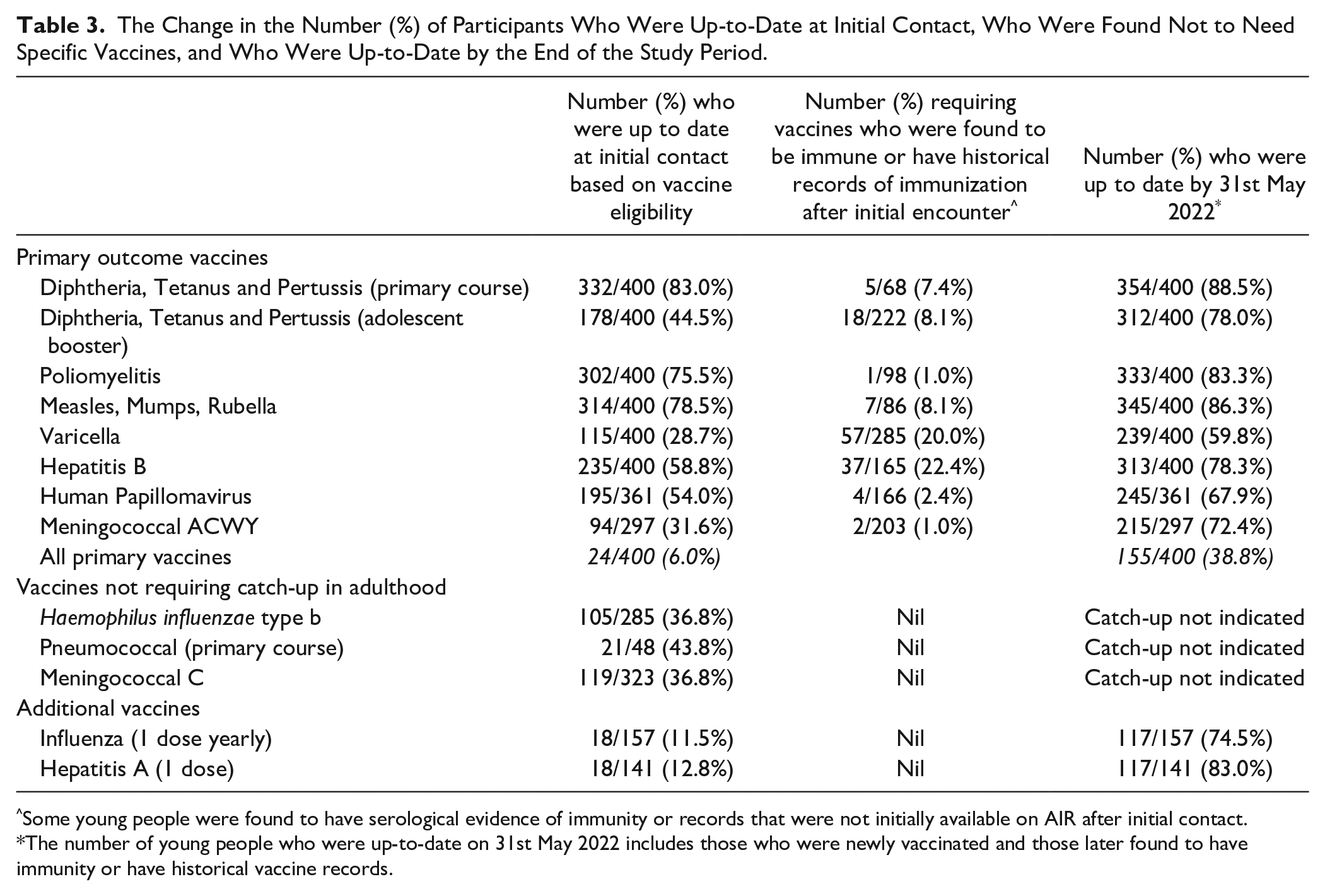
Some young people were found to have serological evidence of immunity or records that were not initially available on AIR after initial contact.
The number of young people who were up-to-date on 31st May 2022 includes those who were newly vaccinated and those later found to have immunity or have historical vaccine records.
At the end of the study period, two-thirds (66%, n = 249) of the 376 young people who had initially required a catch-up plan had received at least one vaccine. One third (35%, n = 131) had completed their plan, and 2 people were awaiting their final visit (Table 3). Varicella coverage increased 2-fold, from 29% to 60%. For the single dose Diphtheria, Tetanus and Pertussis (adolescent booster) and Meningococcal ACWY, 34% and 41% of participants, respectively, had completed their catch-up vaccine, resulting in coverage rates of 78% and 72% respectively by the end of the study period.
In addition to routine vaccines, 141 young people were found to be eligible for the hepatitis A vaccine as part of short-term, state-funded programs for rough-sleepers, people who use drugs, adult prisoners, and men who have sex with men. At initial encounter, only 13% had received the hepatitis A vaccine. Similarly, only 11% of the 157 young people who were medically at risk for influenza had received their annual influenza vaccine. By the end of the study period, coverage of Hepatitis A and influenza vaccines had improved, with 83% (n = 117) and 75% (n = 117), respectively, being up to date.
The main reasons for not receiving a vaccine or not completing the plan (Table 4) was the belief by the young person that their record was incorrect and/or that they had immunity. Fear of injections (n = 20) and pregnancy (n = 17) were other reasons for delaying vaccination. Anti-vaccination views were uncommon, documented on only 2 occasions (1%). The most common reason for not completing a catch-up plan (215 of 243 people) was not being able to contact the young person (eg, their phone line was disconnected or they did not reply to recall messages after a mean of 3.2 attempts). The median time from referral to completion of plan was 78 days (IQR 5-235).
Reasons Documented on Medical Record That Vaccine Was Not Administered at Time of Encounter.

Discussion
This is the first study to detail the extent of under-immunization in young people experiencing homelessness in Melbourne, Australia of whom only 6% were up-to-date with routine childhood and adolescent vaccination at their initial encounter. There were prevalent social and behavioral risks for VPDs and clear benefits of an embedded nurse-led immunization clinic within a specialist homelessness service which resulted in a 6-fold improvement in vaccination coverage.
These findings strengthen the evidence base for nurse-led programs delivering opportunistic vaccinations targeting young people experiencing homelessness. A hallmark of the model reported here is its integration across multiple services where the nurse can build strategic relationships, improve communication with multi-disciplinary professionals, and enhance health service experiences for the young people.8,36 While young people experiencing homelessness can be better engaged in preventative health care when access barriers are reduced,18,37 at 38.8%, the rate of complete vaccine coverage remained well short of the Australian government target of 95% immunization coverage for routine childhood vaccines. 11 This highlights the complex barriers to vaccination faced by young people experiencing homelessness, especially the difficulty homelessness creates in following up individuals, which reinforces the value of opportunistic vaccination when accessing other services.
As with extant research into vaccine hesitancy, specific reasons for not receiving a vaccine when offered were more likely to be because of an acute medical contraindication rather than “anti-vax” ideologies.37,38 In the context of high rates of victimization and unequal provider-client relationships, young people experiencing homelessness commonly distrust service providers, a known barrier to regular and consistent primary health care.3,10 Arguably, improving health literacy and building confidence in health services is also a beneficial outcome, even if young people did not receive a vaccine. These findings are consistent with prior studies among marginalized adolescents in which creating an atmosphere of respect, building trust, and utilizing a team with advanced qualifications and expertise, enhances engagement with health services.8,10,36 While physically located with other services, YPHS maintains confidential health records that do not effect housing decisions.
Homelessness creates health vulnerability. Our data confirm that mainstream services (eg, school vaccination programs) are not effectively reaching this group, which is also at the detriment of the wider Australian population. Our findings suggest national strategies and action plans need to consider the particular needs of young people experiencing homelessness and implement evidence-based interventions that improve access to routine vaccinations and other community health care services. The Australian Immunisation Handbook does not list people experiencing homelessness as a special risk group for vaccination. 32 Likewise, Australia’s National Immunisation Strategy and the National Action Plan for the Health of Children and Young People fail to describe the risk of VPDs in young people experiencing homelessness.9,11 This oversight limits the strength of evidence that can influence policy and the strategic direction of vaccine resource allocation in Australia.
The findings of this study are highly relevant for services which are responsible for children and adolescents who share risks for poor health and homelessness, such as the child welfare and youth justice systems.7,39 Concerningly, most students attending flexible learning centers (alternatives to usual schools) were not up-to-date, despite local councils having responsibility for immunizations in these schools. 40 While future research is indicated to identify the degree of under-immunization in these overlapping cohorts of young people, it is disappointing that Victoria’s Youth Justice Strategic Plan for 2020-2030 does not include a plan for vaccination. 41 At the very least, our findings suggest that any young person who has disengaged from mainstream schooling, or who has contact with child welfare or youth justice systems warrants specific efforts to promote access to routine vaccines. Pragmatically, nurse-led clinics within child protection offices and outreach to residential care units, custodial and non-custodial youth justice settings are a practical solution to reach these children and young people who are also at greater risk of presenting to specialist homelessness services later in life.
This study has several limitations. Our reliance on self-reported data for health risks and social determinants of health is likely to underestimate these, given some young people who attended YPHS and consented to a vaccine history check did not complete a comprehensive psychosocial assessment, resulting in their health risk factors and social determinants of health being unknown. The rate of completion of the HPV vaccine schedule is also likely to be underestimated because at the time of data collection, 2 or 3 doses of HPV vaccine were required to be considered up-to-date, while only one dose is now required. 42 Prior studies have discussed various limitations in the accuracy of the AIR. 43 In some cases during the data collection process, historical vaccine records or natural immunity were identified following initial referral. Future accuracy would be enhanced were nurse immunizers permitted to enter laboratory-confirmed immunity records to the AIR.
In conclusion, homelessness creates health vulnerabilities around VPDs that places individuals and the wider community at risk. While Australians generally benefit from high rates of immunization for childhood and adolescent vaccines, young people who experience homelessness are failing to sufficiently benefit from this important preventative health measure. A co-located nurse-led clinic within existing services is one approach to improve vaccination coverage of young people experiencing homelessness.
Footnotes
Acknowledgements
We wish to acknowledge Melbourne City Mission, the Youth Support and Advocacy Service, Bolton Clarke Homeless Persons Program, Salvation Army Youth Services, and Mind Australia for their collaboration in this nurse-led model, which was funded by the Immunisation Department of the Victorian Government.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Belinda Tominc was awarded the 2021 Elizabeth Fearon Scholarship by the Royal Children’s Hospital League of Former Trainees (LOFT) to support this study. A/Prof Jess Heerde is supported by a National Health and Medical Research Council (NHMRC) Emerging Leadership Investigator Grant (GNT2007722). She holds a Dame Kate Campbell Fellowship awarded by the Faculty of Medicine, Dentistry and Health Sciences at The University of Melbourne. Professor Susan Sawyer is supported by the Geoff and Helen Handbury Chair of Adolescent Health, Department of Paediatrics, The University of Melbourne and an NHMRC Investigator Grant (GNT1196999).