
Abstract
Primary healthcare systems worldwide are under stress as increased demands during pandemic surges have exposed deficiencies in the system. Primary healthcare centers have significant responsibilities but are often underfunded and understaffed. Recent events, including the COVID-19 pandemic, have highlighted the importance of a strong primary health center network to promote community health and save lives. Most governments have multiple competing financial needs for scarce resources, ultimately limiting the advancement of government primary healthcare systems. Hence, various models involving collaboration and outsourcing have been evaluated and employed to improve primary health services. We propose and describe a sustainable and scalable government-society partnership model to bridge the gulf and rejuvenate primary healthcare with a focus on the Indian healthcare system. The involvement of key stakeholders, including society, non-government organizations, and corporate sponsors, is essential to rebuild the network.
Keywords
Introduction
According to the World Health Organization (WHO), healthcare is a fundamental human right, 1 and Developed countries have devoted vast sums of money to ensuring that these needs are met. A substantial portion of budgeted expenses is utilized to build infrastructure and fund public insurance schemes. 2 Private investment into hospital networks and insurance companies shoulder the remaining burden of healthcare delivery. Countries such as Canada, the United States, the United Kingdom, and Japan have varying degrees of private-sector participation. While the merits and demerits of systems in these countries have been extensively analyzed and debated, overall, developed nations tend to have efficient primary care delivery networks. 3
Most developing countries, on the other hand, do not have strong private-sector investments in healthcare, especially in rural and remote areas. Insurance and financial systems are not well established, and there is a greater reliance on the government to provide care. Free or Low-cost government healthcare is plagued with poor quality and often is not trusted by citizens. Despite governments’ best efforts over the decades, chronic underfunding and shortage of staff have led people to seek care elsewhere and not adequately trust the government healthcare system. 4 As a result, out-of-pocket payments for healthcare from private sources have pushed hundreds of millions into extreme poverty. 5 Overall health indices are subpar, and the economic impact of poor health is significant. 6
The COVID pandemic has brought a renewed focus on primary healthcare. The large population of India and the presence of varied healthcare systems allows us to evaluate new models and their impact.
There are many models to provide primary healthcare, such as private clinics, government PHCs, public-private partnerships (PPP), and the solution we propose: a government-society partnership (GSP). In developed countries, there are many care models for private primary care, including fee-for-service and value-based care models and different ownership structures. Of late, large corporations from the retail and insurance sectors have stepped in to acquire and provide primary healthcare in the USA and Canada. 7 In developing countries such as India, rural areas are often unable to pay for private care. The government, therefore, has to shoulder the financial burden of rural healthcare and ensure the effective delivery of services. In India, this is accomplished through government-run Primary Health Centers. However, this system has encountered many challenges. To overcome challenges in providing services in specific areas, such as staffing and management, the government has created the public-private partnership model. 8 It remains to be determined if different models can coexist and complement each other to enhance efficiencies and improve outcomes. For the purposes of this paper, we will focus on public-private partnerships and government-society partnerships.
Indian Healthcare Systems and Primary Health Centers
The Indian public-health sector encompasses 18% of total outpatient care and 44% of total inpatient care. 9 Since 2005, most of the healthcare capacity added has been in the private sector or in partnership with the private sector. The private sector consists of 58% of the hospitals in the country, 29% of beds in hospitals, and 81% of doctors. 9 Private services are concentrated in urban areas, and rural segments often lack even basic healthcare infrastructure. 10
Primary Health Centers (PHCs), created after the Bhore Committee report in 1946, are state-owned rural and urban healthcare facilities in India. 11 They are essentially single-physician clinics, usually with facilities for minor surgeries. Under the National Health Mission (NHM), PHCs are established to cover a population of 30 000 in rural areas and 20 000 in hilly tribal and desert areas—as of March 31, 2019, there are 30 045 PHCs in India, of which 24 855 are located in rural areas and 5190 are in urban areas. 12 In February 2018, the government of India announced the creation of 150 000 Health and Wellness Centers (HWCs) by transforming existing Sub-Centers and Primary Health Centers as the base pillar of the Ayushman Bharat Program. 13
A Renewed Emphasis on Primary Healthcare
India’s 2017 National Health Policy commits the government to invest a major proportion (>2/3rds) of resources in primary healthcare. The main mechanism to achieve this is the 150 000 HWCs, which are intended to become the main points of contact for communities within the public health system. 14 These centers will provide comprehensive healthcare, covering around 70% of out-patient care, including noncommunicable diseases and maternal and child health services. 14 These centers will also provide free essential drugs and diagnostic services as well as referral access to secondary and tertiary healthcare.
This is part of the government’s effort to achieve universal health coverage through its flagship initiative, the Ayushman Bharat program. Launched in 2018, the program includes the health-insurance component, the Pradhan Mantri Jan Aarogya Yojna (PM-JAY). 13
THE Ayushman Bharat Digital Mission (ABDM) ECOSYSTEM
The ABDM is an ambitious program to develop the backbone necessary to support the integrated digital health infrastructure of India. It will bridge the existing gap among different stakeholders of the healthcare ecosystem through digital highways and improve efficiency and transparency through robust databases. This impressive program has the potential to revolutionize primary healthcare in India and provide an attractive framework for many developing countries (Figure 1). 15
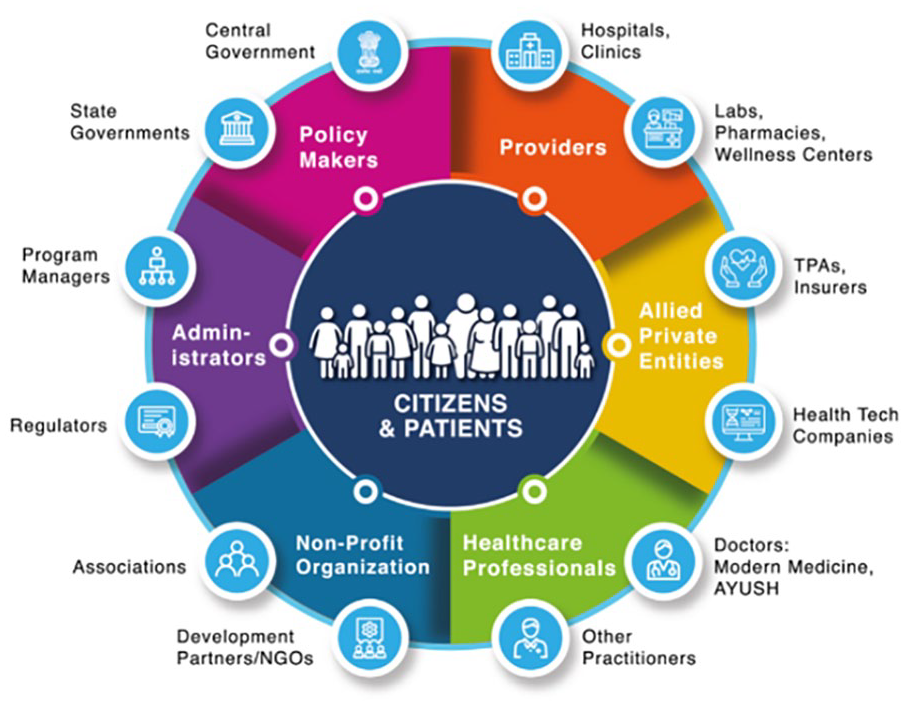
The ABDM model incorporates various stakeholders essential to the success of the system.
With the new NHM, the government has infused additional funds to run PHCs. In 2014, government healthcare expenditures as a share of GDP in India were 1.2%; this has increased to 2.1% in 2022 and is projected to rise to 2.5% in 2025. 16 However, this spending still lags behind other major countries. According to 2019 to 2020 data, developed countries like Japan, Canada, France, the United Kingdom, the Netherlands, New Zealand, Finland, and Australia spend over 9% to 10% of their total gross domestic product (GDP) on healthcare. The United States spends nearly 17% of its GDP on public healthcare, while South Asian countries, including India, Bangladesh, and Pakistan, spend about 3% of their GDP on healthcare. 17 These statistics clearly illustrate the acute shortage of funds in India despite the recent increase. Until these deficits are corrected, it is important to have sustainable partnerships that can fill the healthcare gaps.
Public-private partnership model
When governments are unable to shoulder the burden on their own, the involvement of private organizations has proven effective in rendering services under Public-Private-Partnership (PPP) frameworks. These are contractual frameworks for the outsourcing of healthcare operations primarily due to either funding or staffing deficits. Studies have been conducted to determine factors that enhance PHC utilization. A recent review has evaluated 12 different models and reported on key factors that promote utilization. 18
Public-Private Partnership models have been implemented in different countries. There are 3 distinct models, each emphasizing a particular focus: infrastructure, clinical services, or an integrated approach, which encompasses infrastructure, clinical services, finance, and nonclinical services (Figure 2). 19

The key characteristics of the PPP models are shown above.
Based on the level of services, complexity, and reach, the costs can rise significantly, but the World Economic Forum has projected this model as a potential long-term solution. 20 In some countries, these models have, however, faced hurdles and have not gained widespread acceptance. 8 However, in well-defined situations, the PPP models have proven successful. 21 Karuna Trust, a non-profit organization established in 1986, currently manages 61 Healthcare Centers in 6 states of India: Karnataka, Odisha (formerly Orissa), Arunachal Pradesh, Meghalaya, Uttarakhand, and Tamil Nadu, and serves a population of over 1.5 million. 22
Limitations of the PPP model
Aligning the interests of both public and private entities can be a significant challenge. The private sector, driven by profit motives, may prioritize high-profit services, while the public sector’s objective is to provide equitable access to a wide range of health services. 8 In addition, PPP contracts depend on the government to provide most (if not all) of the funding, which can be a major constraint in less developed countries.
PPP models often necessitate complex contracts and long-term commitments. The process of contract negotiation, monitoring, and enforcement can be challenging. In contexts where public-sector capacity for oversight is limited, ensuring the private sector adheres to agreed-upon standards can be difficult. 8
PPP models may exacerbate health inequities if the private sector is reluctant to invest in areas with low-income populations or remote locations where profitability is less likely. Furthermore, PPP models have centralized operations and would encounter difficulties in scaling up to reach a population of 1.4 billion.
Government-society partnership model
The government-society partnership (GSP) model we propose differs from the PPP and National Digital Health Mission (NDHM) ecosystem models to include village/community representatives, educational institutions such as medical colleges, and corporate sponsors. Crucially, while the PPP model focuses on providing more services for PHCs, the GSP model is focused on improving trust in the government’s primary-care system and bringing in external funds and volunteers. In comparison to the NHDM ecosystem, the GSP model is relatively simple but incorporates vital elements to ensure success. This model is created with a focus on sustainability and scalability. Unlike the PPP model, the GSP model is simply a framework for already existing community members to adopt. Rather than relying on one private company to manage multiple PHCs, different stakeholders in the community assist the government in improving their local PHC. This decentralized approach is what makes the GSP model highly scalable (Figure 3).

The GSP model proposed by the Collaborative Healthcare Foundation.
Role of Government Entities
The most important player in each PHC system is the doctor and his/her staff. District health administrators and the collector must monitor the performance at each of the PHCs. The nearest medical college (both government and private) can provide valuable staffing assistance and post trainees to provide care. Medical colleges often provide critical equipment and supplies to maintain operations. An important role of the government is soon to provide robust support for Information technology and electronic medical records. In addition, governments must incorporate operations within the healthcare system to mitigate the wastage of money and material.
Role of Society and Volunteers
Collaboration with village/tribal heads allows for increased engagement with the community in order to increase PHC usage. Providing a platform for village and community representatives to articulate their needs is important.
At each PHC/HWC, monthly community events should be conducted to enhance participation. Even non-clinical events or health and wellness events can lead to improved utilization. Diet, nutrition, exercise, avoidance of smoking, alcohol consumption, etc., can be agenda items for monthly events. Serving food and conducting simple health screenings at the monthly health events will be effective in improving participation and trust in the healthcare system.
Community volunteers can be allotted specific roles with the prior approval of the district health officer. Student volunteers should be given a high priority in PHC/HWC activities as they represent a large and energetic population already incentivized to help through community service requirements at colleges and universities.
Role of Corporate Sponsors
In addition to their primary economic roles, business corporations bear significant social responsibility. In India, the government has effectively incorporated this concept into a formalized Corporate Social Responsibility (CSR) scheme. 23 As per recent data from the National Institution for Transforming India (NITI Aayog), to reach its Sustainable Development Goals (SDGs), India needs to allocate approximately 13% of its GDP toward social causes, a considerable leap from the current average of about 7%. 24 A portion of this gap is being addressed through the CSR scheme, which has maintained a consistent 15% growth rate year on year (excluding pandemic years) and is projected to account for nearly a third of all private giving by fiscal year 2026. 24
Interestingly, the allocation of CSR funds across sectors has shown notable variation. In fiscal year 21, CSR funding for education, environment, and sustainability decreased by 18% and 36% respectively. However, the healthcare sector witnessed a 30% increase in CSR funds, 24 highlighting its growing importance in the CSR scheme. Notably, in 2022, the top 200 companies listed on the Bombay Stock Exchange (BSE) contributed a hefty 121.22 Billion Indian rupees to CSR initiatives. 25
Primary Healthcare has emerged as a significant beneficiary of this CSR scheme, and there is a continued need for increased funds. Local businesses, being influential members of the community, can leverage their goodwill and resources to ensure the success of these programs. Therefore, their central role within the CSR and broader healthcare funding landscape is crucial. By being a part of this socially responsible initiative, these businesses can contribute significantly to community health and the broader attainment of SDGs.
Role of Non-Government Organizations
Trusted organizations such as Rotary and Lions Clubs have important roles in society and are familiar with the healthcare landscape. They can be useful intermediaries in drawing together corporate sponsors and society representatives to work synergistically.
Smaller non-governmental organizations (NGOs) internationally have played an important role, often with support from donors. Some NGOs backed by corporations such as the Tata Trusts and the Bill & Melinda Gates Foundation can play an important role at a larger level.
Synergy between ABDM and GSP
The GSP model’s robust framework of community participation can make the ABDM more successful. By fostering community involvement and trust, the GSP model can ensure that more people use the digital health IDs and telemedicine services provided by the ABDM, increasing the reach and effectiveness of these tools. For example, the involvement of village/community representatives can encourage the utilization of the ABDM.
Additionally, the GSP model’s focus on corporate social responsibility (CSR) funding can provide valuable financial support to the ABDM. By incentivizing local businesses to contribute to primary healthcare initiatives, the GSP model can help to ensure the sustainability and expansion of the digital health services provided under the ABDM.
Regular community events, a key feature of the GSP, can familiarize communities with the ABDM, boosting its adoption. Further, the GSP’s collaboration with educational institutions and volunteers can aid in training for the ABDM, enhancing user understanding and engagement.
The roles of GSP and ABDM are not mutually exclusive but, in fact, synergistic. Once the ABDM is implemented, the impact of the synergy could be measured by comparing health metrics between PHCs utilizing both models and ones utilizing only the ABDM.
Collaborative healthcare foundation
The Collaborative Healthcare Foundation (CHF) was founded by Siddarth Kasi in 2020. The Collaborative Healthcare Foundation is a registered 501(C)(3) non-profit and tax-exempt organization in Orlando, Florida, USA with an affiliate organization: CHF India. Initial projects began in the Nilgiris, Coimbatore, and Erode districts of Tamil Nadu and have expanded to other Indian states, now reaching nearly 50 PHCs. Now programs have expanded internationally to other countries such as Ethiopia, South Africa, Colombia, Jamaica, and Guyana.
CHF has over 100 members and volunteers, who are primarily high school and college students based in the United States. These members adopt a PHC and focus on its development. They donate equipment and supplies, improve and create new infrastructure, develop and implement special health programs, conduct specialty medical camps, community awareness and outreach programs, and educate and train students in India. These activities are intended to support existing infrastructure and services provided by the government and not replace them.
CHF has adopted an open, decentralized model with public and youth participation. It does not operate PHCs on a day-to-day basis like the Karuna Trust. In terms of social networking comparison, Karuna Trust follows a client-server model with centralized operations, whereas CHF follows a peer-to-peer model with interconnected nodes of youth volunteers, corporate sponsors, and NGOs to address the needs of a vast network of PHCs.
Pilot Program to improve PHCs by implementing the GSP model
In order to improve existing PHCs, we developed a 6-step process, as shown below, to implement the GSP model and track outcomes (Figure 4).
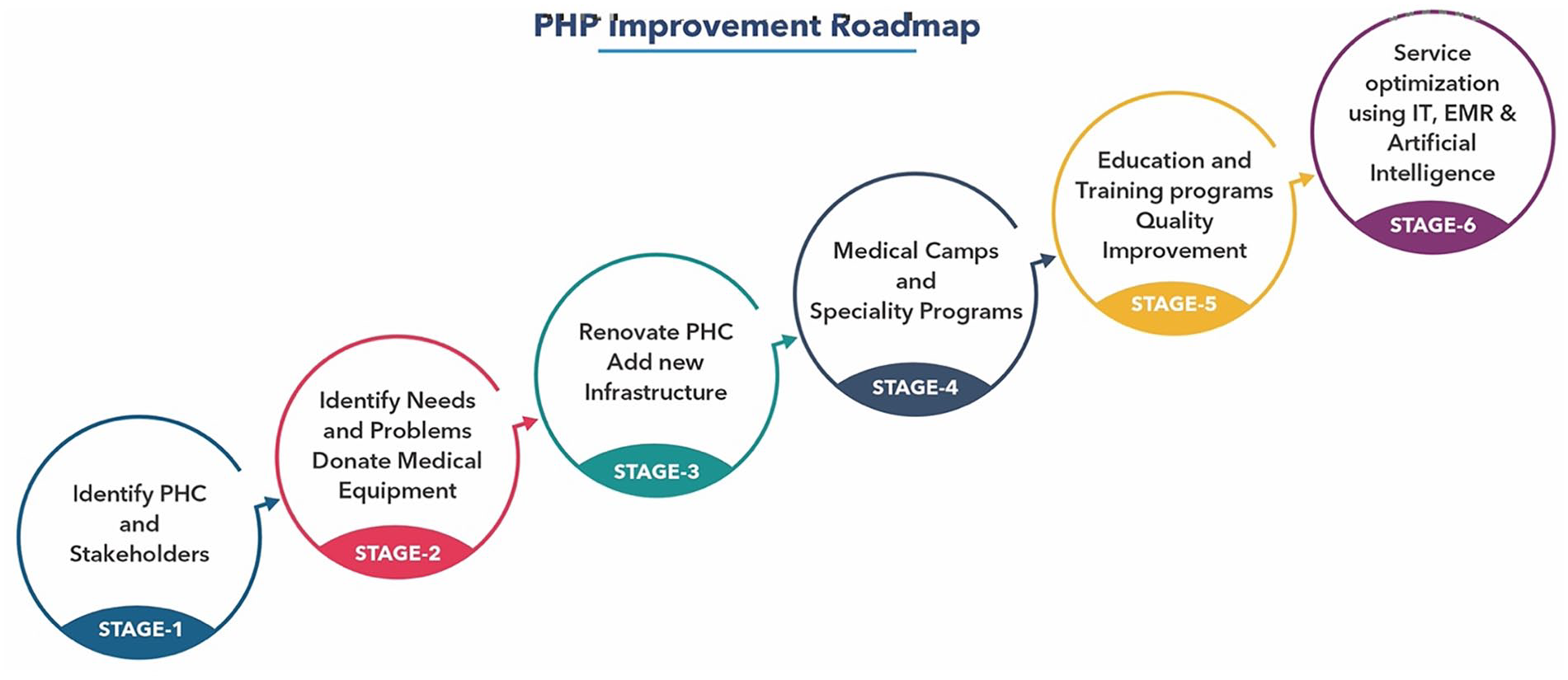
The 6-step process to redevelop PHCs proposed by Collaborative Healthcare Foundation.
Identifying suitable PHCs is a multi-step process. Adequate interest, collaborative spirit, and timely approvals are important to ensure success. It is important to secure the buy-in of key stakeholders prior to the implementation of major projects. The intentions and expectations of this collaborative effort have to be clearly defined, and often a meeting can help to discuss and chart out the path. Identifying the needs of the people is essential to prevent wasteful expenditure. Sustainability is the underlying theme as various steps are implemented. Outcomes and utilization have to be tracked to ensure optimal return on investment.
Pilot GSP model implementation project
The pilot project was taken up at Karadimadai PHC in Thenkarai Taluk, Coimbatore District, Tamil Nadu, India. This site was chosen as a sample rural area, and we were able to incorporate all major elements of the GSP model.
Village representatives were very involved and participated right from the outset in defining the needs of the community. They identified the lack of essential medical equipment and shelter from inclement weather while waiting outside for their turn to see the doctor. The physician in charge was very motivated to improve the facilities and provide more services at his PHC. The District Health Director and the Collector of Coimbatore expressed their full support and gave the necessary approvals.
RPP Infra Projects volunteered to be the corporate sponsor and provided generous contributions. The upgrades included a new 600 sq ft. patient waiting area that serves as a multipurpose hall for conducting medical camps and patient education that can be partitioned to ensure privacy while treating patients. The laboratory facilities were upgraded, and a biowaste room was added. In addition, CHF donated essential equipment, including wheelchairs, surgical lamps, water heaters, stethoscopes, sphygmomanometers, and other critical supplies. Avinashilingam University adopted the villages surrounding this PHC, and its students are active in promoting community health as a part of their National Service Scheme (NSS) activities. The Pelamedu Samanaidu Govindasamy College of Technology (PSG) Institute of Medical Sciences & Research staff conducted medical camps and provided enhanced medical services to patients at the PHC. Rotary International coordinated meetings with key stakeholders. At the inauguration of the new facilities, community members who attended were provided snacks and small gifts made possible via contributions from CHF volunteers.
Additional work is underway to enhance and upgrade labor and delivery facilities. Utilization of services and patient satisfaction will be assessed at the 1-year mark.
Scope of future expansion
Based on this pilot project, a larger 20 PHC project is being evaluated in Tamil Nadu to expand the program. This model implemented in South India will form a template for primary health clinics run by governments in developing countries globally.
Limitations of the GSP model
The GSP model relies on the active participation of multiple stakeholders, each with its own interests, resources, and limitations. Coordinating projects and ensuring alignment among these entities may be a significant challenge.
The model relies on the willingness and capacity of village and tribal heads, community representatives, and student volunteers to actively participate. Changing priorities may diminish levels of participation, and alternate members may have to step in to continue the collaborative effort. Issues such as cultural differences and disparities in health literacy could affect engagement levels and, subsequently, the overall efficacy of the model.
The role of corporate sponsors, while vital, could potentially be inconsistent due to market fluctuations and changes in business priorities. The allocation of CSR funds may not always align with the needs of PHCs, and there might be disparities in fund distribution across different regions. 26
Therefore, while the GSP model represents a novel and potentially effective approach to primary healthcare, its success depends on effectively addressing these potential limitations.
Conclusion
The GSP model provides a novel framework for improving the performance of primary health centers and providing care. The proposed model focuses on fostering society and business participation, while ABDM focuses on digital infrastructure to revolutionize healthcare delivery. We envision significant synergism between the GSP model and ABDM proposed by the Government of India.
Footnotes
Acknowledgements
We would like to thank P. Arulsundaram, MD. RPP Infra Projects; Dr. T. Radha PhD, Avinashilingam College, Mahalakshmi, Village Councillor, Karadimadai, Coimbatore, Mr. Kamal Kumar, Rotary Club of Texcity, Coimbatore, Dr. G S Sameeran, District Collector, Coimbatore, Dr. P. Aruna, Deputy Director of Health Services, Coimbatore.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.