
Abstract
Introduction:
Over the last 30 years, the adoption of health information technology and digital health tools (DHTs) into the US health system has been instrumental to improving access to care, especially for people living in rural, underserved, and underrepresented communities. Despite widespread adoption of DHTs by primary care clinicians, documented challenges have contributed to inequitable use and benefit. The COVID-19 pandemic necessitated rapid adoption of DHTs, accelerated by state and federal policy changes, in order to meet patient needs and ensure access to care.
Methods:
The Digital Health Tools Study employed a mixed methods approach to assess adoption and use of DHTs by primary care clinicians in southeastern states and identify individual- and practice-level barriers and facilitators to DHT implementation. A survey was conducted using a multi-modal recruitment strategy: newsletters, meeting/conference presentations, social media, and emails/calls. Focus groups were conducted to assess priorities, barriers, and facilitators and were recorded/transcribed verbatim. Descriptive statistics were calculated for survey results, produced for the whole sample, and stratified by state. Thematic analysis was conducted of focus group transcripts.
Results:
There were 1215 survey respondents. About 55 participants who had missing demographic information were excluded from the analysis. About 99% of clinicians used DHTs in the last 5 years, modalities included: telehealth (66%), electronic health records (EHRs; 66%), patient portals (49%), health information exchange (HIE; 41%), prescription drug monitoring programs (39%), remote/home monitoring (27%), and wearable devices (22%). Time (53%) and cost (51%) were identified as barriers. About 61% and 75% of clinicians reported being “satisfied” to “very satisfied” with telemedicine and EHRs, respectively. Seven focus groups with 25 clinicians were conducted and indicated COVID-19 and the use of supplemental tools/apps to connect patients to resources as major motivators for adopting DHTs. Challenges included incomplete and difficult-to-utilize HIE interfaces for providers and internet/broadband access and poor connectivity for patients.
Conclusions:
This study describes the impact adopting DHTs by primary care clinicians has on expanded access to healthcare and reducing health disparities in regions with longstanding health and social inequities. The findings identify opportunities to leverage DHTs to advance health equity and highlight opportunities for policy improvement.
Introduction
The US health system has seen a rapid increase in adoption of health information technology and digital health tools (DHTs) over the last 30 years.1,2 DHTs have the potential to ameliorate health disparities, but only if they are accessible and used by clinicians serving patient populations experiencing health inequities. Despite the rapid uptake of DHTs and accompanying investments, inequitable access to and use of DHTs by primary care clinicians and patients has remained a problem.3 -6
The COVID-19 pandemic amplified long-standing health inequities in rural, underserved, and underrepresented communities. Existing inequities in the arenas of access to broadband/internet for Black, Latinx, and rural communities, food insecurity, cultural insensitivity, and racial biases were exacerbated by the COVID-19 pandemic.7,8 The rapid adoption and use of DHTs served as a catalyst to reach patients who previously had obstacles to care. This rapid implementation was accelerated by state and federal policy changes, including enhanced reimbursement rates for telehealth, reduced or waived cost-sharing for patients, and the ability for federally qualified health centers (FQHC) and rural health clinics to offer telehealth services to offsite patients. The patients who have benefitted most from the greater availability of these services are those with mobility and transportation barriers due to chronic illness, distance to care, lack of transportation, paid time off, or affordable childcare. 9
Primary care practices, especially those serving underserved communities faced unique barriers and challenges adopting and using technology such as electronic health records and telemedicine, compared to specialists and other higher resourced health care settings. Similarly, African American and Latino/a/x patients in rural and underserved communities are less likely to be seen in primary care practices that have adopted digital technology programs and are therefore less likely to engage in patient portals and other patient engagement tools and consumer technologies. 3 These gaps severely limit the benefits enabled by technology to reach these populations, contributing to existing health disparities across these groups.
The goal of the Digital Health Tools Study (DHTS) was to assess adoption and use of DHTs by primary care clinicians working in underserved communities in the Southeastern U.S. For this study, DHTs include but are not limited to telemedicine, home/remote monitoring, patient portal, health information exchange (HIE), electronic health records (EHR), prescription drug monitoring program (PDMP), wearable devices, mobile applications, and other tools/technologies used in healthcare settings. This paper describes the DHTS survey and focus group findings, characterizes adoption, and use of DHTs by primary care clinicians across the Southeastern US, and highlights the implications of these findings for efforts to achieve equity in access to and implementation of DHTs. This study fills a gap in the existing literature, as to our knowledge, there are currently no descriptive studies that focus on DHT implementation in primary care practices that serve populations disproportionately impacted by a wide range of health inequities in the Southeastern U.S.10 -15 This study can inform interventions on multiple levels to improve the adoption and use of DHTs to advance health equity.
Methods
A mixed methods approach was used to identify multi-level barriers and facilitators to DHT adoption and use; levels examined included the individual clinician, practice, population, and health system/policy. This paper focuses on the results from an electronic survey and a series of focus groups which assessed clinician characteristics and DHT use and implementation across multiple practice settings. The survey and focus group data were analyzed separately. The findings from both methods were synthesized and interpreted as a single study.
Participants and Recruitment
Participant recruitment for the survey and the focus groups began in September 2019. The recruitment approach was targeted towards practicing primary care clinicians. Recruitment activities focused primarily on 4 southeastern states (Georgia, Kentucky, North Carolina, and Tennessee), however, participants that practiced in any of the southeastern states were included in the study. Initially, recruitment was conducted at in-person state and regional primary care meetings and conferences, where the team set up exhibit tables and booths, made announcements during sessions, and relied on word-of-mouth to recruit clinicians to complete the survey and join a focus group. When the COVID-19 pandemic prevented travel and in-person events in mid-March 2020, the recruitment approach pivoted to virtual recruitment and engagement. The study team leveraged partnerships with state and local primary care organizations, hospital/health systems, rural health associations, state agencies, and other community organizations and clinician groups. Recruitment flyers for both the survey and focus groups were added to e-newsletters through internal and external e-mail listservs of primary care clinicians, website ads were purchased through state organized medicine partners, and marketing materials were shared on social media (Facebook, LinkedIn, and Twitter).
Surveys
The DHTS survey was conducted using the secure online database system Research Electronic Data Capture (REDCap; see Supplemental Appendix A). The survey included a total of 22 questions, and a combination of open-ended/Likert scale/ranking and branching logic to identify (1) prior/current use of DHTs; (2) reasons for adopting/using DHTs; (3) barriers and facilitators to adoption/use; and (4) clinician demographic and practice characteristics. The survey also asked participants which specific DHTs they used, and a series of questions related to each selected DHT. Detailed socio-demographic information, including state of practice, primary care discipline, practice setting, age, race, and years in practice was collected. In March of 2020, 1 question was added to the survey about use of DHTs due to the pandemic. Responses were anonymous and were not linked to identifying information. Participants received a $50 gift card upon completion of the survey as compensation for their time.
Focus Groups
The focus groups were facilitated using a semi-structured interview guide (see Supplemental Table 1) that focused on the following topics: (1) adoption and sustainability of DHTs; (2) impact of DHTs on patient health and practice workflow; and (3) facilitators and barriers related to the adoption and implementation of DHTs in primary care practice. Participants were recruited via internal and external listservs, survey participants, and social media. All focus groups were conducted in English. Focus groups were recorded via Zoom and transcribed verbatim using NVivo transcriptions. No identifying information was included in the transcripts. Informed consent was obtained, and participants received a $100 gift card for their participation.
Qualitative and Quantitative Analysis
Survey data was collected and stored in REDCap and exported to Microsoft Excel for analysis. Participants with missing or incomplete demographic information were excluded from the analysis (n = 55). Descriptive statistics were calculated for the overall sample and stratified for each of the following states: Georgia, North Carolina, Kentucky, and Tennessee. Multivariate logistic regression models were developed using each of the DHTs (telemedicine, HIE, EHR, remote monitoring, and patient portal) as outcomes, demographic characteristics (sex, age, race, and ethnicity), and practice-relevant features (credential, specialty, years in practice, technology enthusiasm, practice setting, ownership, Medicaid acceptance, urban/rural status of practice location, quality reporting programs enrolled, and number of quality programs enrolled) as predictors. Adjusted odds ratios, 95% confidence intervals, and P-values were calculated and reported. P-values <.05 were considered statistically significant.
Focus group transcripts were analyzed for themes independently and a codebook was then developed by group consensus. The coding scheme was applied to the transcripts and a thematic analysis conducted both by-hand and using NVivo 12 Plus. Facilitator notes from focus groups were uploaded into NVivo 12 Plus and analyzed. Key themes were reviewed and then narrowed down to major themes for analyses in NVivo 12 Plus. Based on the quotations and/or other phrases selected in the documents, major codes and/or sub-codes were assigned. At the conclusion of coding all the documents, outputs were generated to identify the frequencies of codes and quotes, or phrases associated with the codes.
Results
Survey Respondents and Demographics
A total of 1215 surveys were completed by clinicians who practice in the Southeast and 1160 responses with complete demographic information and survey responses were included in the analysis. Of these, 40 surveys were completed prior to March 15, 2020, when COVID-19 stay-at-home orders were starting to be implemented. Most respondents held Doctor of Medicine/Doctor of Osteopathic Medicine (MD/DO; 63%) and Nurse Practitioner (NP)/Physician Assistant (PA)/Certified Nurse Midwife (CNM; 24%) credentials. Clinicians specialized in family and internal medicine, geriatrics, and pediatrics, which were collectively defined as primary care (85%) and practiced in urban areas (91%). About 90% of clinicians accepted Medicaid in their practice and 35% indicated they participated in the Medicaid EHR incentive program. The highest proportion of clinicians practiced in large practices with more than 5 clinicians (31%) and hospital/outpatient care settings (31%), followed by community health centers (17%), small practices with less than 5 clinicians (8%), and solo practices (7%). Full sample characteristics are presented in Table 1.
Demographic Characteristics and Survey Responses for the Overall Sample and 4 Major States.

Abbreviations: FQHC, Federally Qualified Health Center; MD/DO, Doctor of Medicine/Doctor of Osteopathic Medicine; NP/PA/CNM, Nurse Practitioner/Physician Assistant/Certified Nurse Midwife; PhD, Doctor of Philosophy; VA, Veterans’ Affairs.
Multiple responses can be selected, thus total of column percentages >100%.
DHT Use
99% of clinicians surveyed reported using DHTs in the last 5 years. Respondents used the following DHTs: telemedicine (66%), EHRs (66%), patient portals (49%), HIE (40%), PDMP (39%), remote/home monitoring (27%), and wearable devices (22%). Telemedicine was most used by Family Medicine physicians, clinicians who practice in FQHCs, and clinicians practicing adult general medicine; 66% and 73% of clinicians reported being “satisfied” to “very satisfied” with telemedicine and EHRs, respectively. About 76% of respondents were connected to their State HIE, yet 41% reported using it.
90% of all survey participants reported using DHTs because of the COVID-19 pandemic. About 76% have used or plan to use telehealth because of the COVID-19 pandemic, followed by EHRs (50%), HIE (35%), patient portals (34%), remote monitoring (27%), PDMP (24%), wearable devices (22%), and mobile apps (18%). A full description of respondent use of DHTs can be found in Table 2.
Demographic Characteristics of Survey Respondents by DHT Usage.
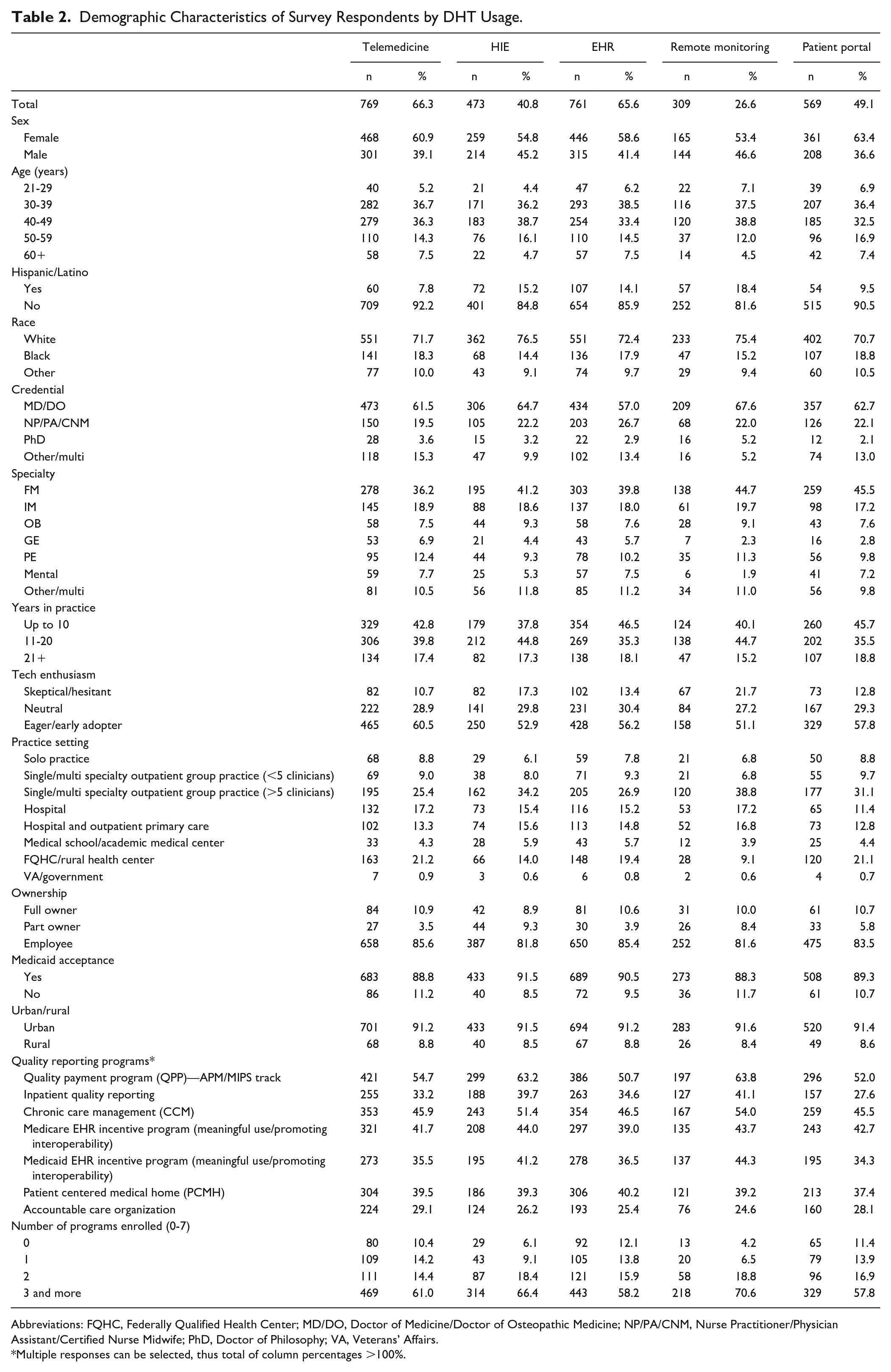
Abbreviations: FQHC, Federally Qualified Health Center; MD/DO, Doctor of Medicine/Doctor of Osteopathic Medicine; NP/PA/CNM, Nurse Practitioner/Physician Assistant/Certified Nurse Midwife; PhD, Doctor of Philosophy; VA, Veterans’ Affairs.
Multiple responses can be selected, thus total of column percentages >100%.
Barriers/Facilitators to DHT Implementation
Time (53%), cost (51%), and limited workflow integration (40%) were the top barriers to adoption of DHTs (see Figure 1). Barriers were clinician-focused and highlighted challenges clinicians face with integrating DHTs into the workflow and infrastructure of their practices. Clinicians in large practices (OR = 1.835, 95% CI = 1.173-2.878) were almost 2 times more likely to report time as a barrier compared to those in a community health center. Early adopters of DHTs (OR = 1.452, 95% CI = 1.095-1.927) were one and a half times more likely to report cost as a barrier compared to those of neutral enthusiasm. Additionally, those who participated in a quality payment program (QPP; OR = 1.445, 95% CI = 1.035-2.023) were one and a half times more likely to report limited workflow integrations as a barrier compared to those who did not participate. Focus groups highlighted COVID-19 as a catalyst for adoption of DHTs among primary care clinicians.

Top 3 barriers to adopting DHTs.
Ease of workflow integration (58%), meeting patient needs (55%), and improving patient health (50%) were the top facilitators to adoption of DHTs (see Figure 2). Facilitators tended to be patient-focused as opposed to barriers. Clinicians who identified as Black (OR = 1.505, 95% CI = 1.069-2.132) and any other race (OR = 1.932, 95% CI = 1.243-3.058), to be eager and early adopters (OR = 1.468, 95% CI = 1.104-1.952), and participated in a QPP (OR = 1.422, 95% CI = 1.006-2.017) were more likely to report ease of workflow integration as a facilitator. Meeting patient need was more likely to be reported as a facilitator by clinicians who possessed a NP/PA/CNM (OR = 1.861, 95% CI = 1.295-2.685), PhD (OR = 2.319, 95% CI = 1.106-4.999), or any other or combination of credentials (OR = 1.779, 95% CI = 1.065-2.994) than MD/DO, identified as Hispanic/Latino (OR = 1.759, 95% CI = 1.114-2.817) than non-Hispanic/Latino, and participated in the Medicaid EHR Incentive Program (OR = 1.818, 95% CI = 1.314-2.533). People were more likely to have reported improving patient health as a facilitator to their adoption of DHTs if they identified as Hispanic/Latino (OR = 1.636, 95% CI = 1.041-2.592), possessed an NP/PA/CNM (OR = 1.777, 95% CI = 1.239-2.559) compared to MD/DO, specialty of practice was Obstetrics (OR = 1.749, 95% CI = 1.038-2.985) compared to family medicine, and participated in these quality payment programs: Inpatient Quality Reporting (OR = 1.499, 95% CI = 1.065-2.116), Chronic Care Management (COR = 1.392, 95% CI = 1.007-1.930), Patient Centered Medical Home (OR = 1.387, 95% CI = 1.016-1.898), and Accountable Care Organization (OR = 1.769, 95% CI = 1.272-2.471). Focus group participants discussed patients’ need for continued services, such as mental/behavioral health therapy, forced clinicians to adapt quickly to DHTs. A major benefit was the use of supplemental tools/apps to connect patients to resources. Challenges included care coordination between providers and internet/broadband access and poor connectivity for patients (see Supplemental Table 2 for full results).

Top 3 facilitators to adopting DHTs.
Model Results on Factors Associated With Different DHT Usage
Full results of models are reported in Table 3. Clinicians who reported using DHTs in the last 5 years were significantly less likely to use telemedicine if they were Hispanic/Latino (OR = 0.338, 95% CI = 0.209-0.543); they were significantly more likely to use telemedicine if they were in specialties of internal medicine (OR = 2.056, 95% CI = 1.336-3.193 ), geriatrics (OR = 2.100, 95% CI = 1.034-4.400), pediatrics (OR = 3.696, 95% CI = 2.053-6.957), mental (OR = 2.317, 95% CI = 1.158-4.783), and other/multiple specialties (OR = 1.748, 95% CI = 1.035-2.996); eager/early adopter of technology (OR = 1.792, 95% CI = 1.295-2.480); enrolled in Medicare EHR Incentive Program (OR = 1.592, 95% CI = 1.093-2.331) or Accountable Care Organization (OR = 1.891, 95% CI = 1.278-2.831). If participants were in specialty of other/multiple specialties (OR = 1.733, 95% CI = 1.088-2.768), or enrolled in Quality Payment Program (QPP; OR = 1.409, 95% CI = 1.009-1.972) or Chronic Care Management (OR = 1.513, 95% CI = 1.110-2.068), they were significantly more likely to use HIE. Being Hispanic/Latino (OR = 1.666, 95% CI = 1.014-2.796), having a credential for NP/PA/CNM (OR = 1.910, 95% CI = 1.271-2.903), being an eager/early adopter of technology (OR = 1.506, 95% CI = 1.108-2.049), accepting Medicaid (OR = 1.641, 95% CI = 1.031-2.612), and enrollment in Chronic Care Management (OR = 1.467, 95% CI = 1.047-2.066) or Patient Centered Medical Home (PCMH; OR = 1.463, 95% CI = 1.051-2.045) were positively associated with EHR utilization. Participants were significantly more likely to use remote monitoring if they were Hispanic/Latino (OR = 2.411, 95% CI = 1.525-3.819), or enrolled in 2 (OR = 3.303, 95% CI = 1.453-7.866) or 3 and more (OR = 4.989, 95% CI = 1.803-14.307) quality reporting programs. Female participants (OR = 1.385, 95% CI = 1.056-1.818) were significantly more likely to use patient portal than males.
Multivariable Logistic Regression Results for Different DHT Usage.

Abbreviations: FQHC, Federally Qualified Health Center; MD/DO, Doctor of Medicine/Doctor of Osteopathic Medicine; NP/PA/CNM, Nurse Practitioner/Physician Assistant/Certified Nurse Midwife; PhD, Doctor of Philosophy; VA, Veterans’ Affairs.
Focus Group Respondents and Demographics
Seven focus groups and listening sessions with 25 clinicians were facilitated to have in-depth conversations about their use of DHTs, including any barriers and facilitators to use. Participants practiced in Georgia (28%), Kentucky (28%), North Carolina (24%), and in states outside of our area of interest including: Arizona (4%), Florida (4%), Louisiana (4%), Texas (4%), and Virginia (4%). The most common overall themes identified were barriers and facilitators to DHT use, use of tools and technology, access to care, and the impact of the COVID-19 pandemic on providing care to patients. Table 4 provides selected quotations from focus group participants relevant to the identified themes. Clinicians highlighted challenges with engaging patients with DHTs due to language barriers. For some clinicians serving in areas with patients whose first language was not English, their EHR or patient portal did not have the ability to translate information for patients to utilize without assistance. There was also discussion about the importance of the patient-clinician relationship and how much it matters—“technology is an aid to care, not a substitute for it.” Discussion about telemedicine use accounted for an average of 20% of the conversation across all focus groups. These conversations focused on telemedicine use in low income/rural settings, its use for mental and behavioral health encounters, and the barriers to accessing telehealth specifically including but not limited to lack of internet access/connectivity, the need for broadband infrastructure, and the need for patient access to phones for audio and video appointments (in which cost was a major-cited barrier). The high costs associated with purchasing, integrating, and training on the use of new DHTs placed a huge financial burden on some clinicians, especially for early adopters and those in small practices and rural settings. Clinicians also highlighted the lack of autonomy by those in non-leadership positions in the decision-making process and implementation of technology int their practice setting compared to clinicians in leadership positions. See Supplemental Appendix B for a list of all coded themes and sub-themes.
Most Common Overall Themes of Clinician Perceptions and Example Quotes.

Discussion
This study found widespread adoption and use of DHTs, consistent with other studies. However, challenges related to workflow integration, the digital divide, policy and/or insurance barriers, time, and cost continue to pose barriers to meaningful use of DHTs and have implications for health equity. Clinicians reported challenges with adoption and use of DHTs because many DHTs were not designed with the users in mind.1,3,16,17 The digital divide has posed a longstanding barrier to health equity, as nearly half of Americans without at-home internet were Black and Hispanic households.18 -20 The reported gap between connection to a HIE and the actual use of that technology is problematic, as meaningful, real-time, and clinically relevant exchange of health information could support better outcomes in chronic disease management for patients and populations. If implemented and utilized in meaningful ways, HIE could support better health outcomes, and overcome health disparities among underserved communities.13,21 -23 Language barriers can also exacerbate other health inequities, including access to care. Some non-native English speakers prefer text or email with providers so they can have more time to interpret and respond to communication. DHT literacy and use is impacted by language literacy. 24
If the adoption and use of DHTs by primary care clinicians is to improve, with the intention of advancing health equity, our findings suggest workflow barriers faced by clinicians must be addressed. The multi-click nature of EHRs or the lack of reliable, usable reporting data of HIEs are time-consuming and resource-intensive.25 -27 It is apparent that clinicians need to be involved in the development of DHTs to be more aligned with their workflows and tailored for the needs of their patients. Clinicians in non-leadership positions reported feeling disconnected to the technology and disempowered by leadership decisions forcing clinical staff to use DHTs when they were not included in the decision-making process. Clinicians who had leadership roles, were more likely to feel connected to the tools and bought in to the purchasing decisions. Clinicians reported that the lack of access to internet, Wi-Fi, broadband, phone, computers, and other technologies posed many barriers to providing equitable access to care to their patients. However, clinicians were resilient and highly creative during the pandemic, as exemplified by stories presented during focus groups of clinicians using tablets and taking them out to patients’ cars who were in the office’s parking lot to conduct a telehealth appointment. This study also identified a need for culturally tailored technology.
Although reimbursement was not one of the top facilitators for DHT adoption and use, cost was one of the top barriers. Payment policies related to DHTs, for example equal reimbursement for services delivered via telehealth as those same services delivered in-person (parity), could reduce the cost burden on clinicians. DHTs may positively impact patient outcomes, but only if there are appropriate incentive and payment models and long-term investments into clinician feasibility. Private insurance companies have begun leveraging wearable devices and health applications to incentivize individuals to adopt healthy lifestyle habits aligned with evidence-based wellness and preventative research. 28 Payment models, such as chronic care management (CCM), complement the value-based care model while offering healthcare providers an additional revenue stream. CCM supported by remote patient monitoring has shown to improve quality outcomes for conditions such as hypertension. 29 Such payment policies should support the current workforce by reducing burnout, provide meaningful tools for clinicians to improve relationships with patients, and engage patients. Technology standards, routine guidelines, and protocols for DHTs that become standard of care and support primary care clinicians and patients are also needed.
Limitations and Caveats
There are several limitations to this study, including conducting it in the height of the COVID-19 pandemic. The pandemic restrictions eliminated in-person survey recruitment and focus group opportunities, required substantial changes to the recruitment strategy, and impacted the demographics of the study population. Additionally, our survey underwent several iterations. COVID-19 specific questions were added during the pandemic, which increased the length of the survey. This potentially increased the rate of incomplete survey responses. Lastly, there was a small sample size of focus groups, which were not inclusive of all states. Focus groups were conducted across years with several updates to the focus group guide and different facilitators.
Conclusion
This study offers nuanced information and analyses related to adoption, use, and satisfaction with DHTs by primary care clinicians in the Southeastern US in the context of a global pandemic and unprecedented multi-sector efforts to advance health equity. Improved access to care can be achieved by addressing workflow barriers, closing the digital divide, expanding access to broadband/wireless internet, and improving health literacy through resources, user-centered design, and training. The increasing use of DHTs has the potential to improve outcomes for many chronic conditions, reduce racial/ethnic health disparities and address other social determinants of health, and catalyze health care transformation. Further research is needed to examine the adoption and use of DHTs by patients and the implementation of pre-and-post COVID-19 era policies and their long-term impact on health outcomes.
Supplemental Material
sj-docx-1-jpc-10.1177_21501319231184789 – Supplemental material for Opportunities and Challenges to Advance Health Equity Using Digital Health Tools in Underserved Communities in Southeast US: A Mixed Methods Study
Supplemental material, sj-docx-1-jpc-10.1177_21501319231184789 for Opportunities and Challenges to Advance Health Equity Using Digital Health Tools in Underserved Communities in Southeast US: A Mixed Methods Study by Mitchell A. Blount, Megan D. Douglas, Chaohua Li, Denita T. Walston, Phoebe L. Nelms, Carmen L. Hughes, Anne H. Gaglioti and Dominic H. Mack in Journal of Primary Care & Community Health
Supplemental Material
sj-docx-2-jpc-10.1177_21501319231184789 – Supplemental material for Opportunities and Challenges to Advance Health Equity Using Digital Health Tools in Underserved Communities in Southeast US: A Mixed Methods Study
Supplemental material, sj-docx-2-jpc-10.1177_21501319231184789 for Opportunities and Challenges to Advance Health Equity Using Digital Health Tools in Underserved Communities in Southeast US: A Mixed Methods Study by Mitchell A. Blount, Megan D. Douglas, Chaohua Li, Denita T. Walston, Phoebe L. Nelms, Carmen L. Hughes, Anne H. Gaglioti and Dominic H. Mack in Journal of Primary Care & Community Health
Supplemental Material
sj-docx-3-jpc-10.1177_21501319231184789 – Supplemental material for Opportunities and Challenges to Advance Health Equity Using Digital Health Tools in Underserved Communities in Southeast US: A Mixed Methods Study
Supplemental material, sj-docx-3-jpc-10.1177_21501319231184789 for Opportunities and Challenges to Advance Health Equity Using Digital Health Tools in Underserved Communities in Southeast US: A Mixed Methods Study by Mitchell A. Blount, Megan D. Douglas, Chaohua Li, Denita T. Walston, Phoebe L. Nelms, Carmen L. Hughes, Anne H. Gaglioti and Dominic H. Mack in Journal of Primary Care & Community Health
Supplemental Material
sj-xlsx-4-jpc-10.1177_21501319231184789 – Supplemental material for Opportunities and Challenges to Advance Health Equity Using Digital Health Tools in Underserved Communities in Southeast US: A Mixed Methods Study
Supplemental material, sj-xlsx-4-jpc-10.1177_21501319231184789 for Opportunities and Challenges to Advance Health Equity Using Digital Health Tools in Underserved Communities in Southeast US: A Mixed Methods Study by Mitchell A. Blount, Megan D. Douglas, Chaohua Li, Denita T. Walston, Phoebe L. Nelms, Carmen L. Hughes, Anne H. Gaglioti and Dominic H. Mack in Journal of Primary Care & Community Health
Footnotes
Acknowledgements
The study team would like to extend a special thanks to all study participants; without their consent to participate in the surveys, focus groups, and presentation, this study would not have been possible.
Author Contributions
All the authors participated in the study concept and design, analysis, and interpretation of data, drafting and revising the paper, and have seen and approved the final version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported in partnership with the United Health Foundation, grant number 6479.
Ethical Approval and Consent to Participate
In accordance with the Declaration of Helsinki, this study was reviewed by Morehouse School of Medicine Institutional Review Board (IRB) and determined to be approved by expedited IRB review under section 45 CFR 46.101, item 2. Morehouse School of Medicine IRB approved informed consent for all study participants prior to study participation. Participants included in this report approved use of their demographic and response data for the purposes of research. All authors assert that all procedures contributing to this work comply with the ethical standards of Morehouse School of Medicine.
Availability of Data and Materials
All data supporting the study findings are contained within this manuscript.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.