
Abstract
This action research aimed to study the processes of public health policy toward salt reduction in food consumption. The processes were divided into 3 cycles as follows: 1) Public health policy formation; 2) Development of the policy to reduce dietary salt; and 3) Evaluation of the efficiency of the policy. Participants from the first group involved in policy formation; and a total number of 320 participants were recruited in the study with the criteria of a) age 18 years and above, b) having hypertension or at risk of having high blood pressure; c) overweight; and d) having underlying diseases such as diabetes and hyperlipidemia. The second group was government officials involved in policy development to reduce salt consumption, including the head of the village, assistants of the village head, community leaders, public health personnel, village health volunteers, and a group of housewives. In total, 50 participants were recruited to the study. The results showed that people with hypertension could better control blood pressure which increased from 36.02, 25.6, and 39.06% (in 2018-2020) to 47.32%; and community people could manage their health prevention and control toward non-communicable diseases. Analyzing a return on investment (ROI) found that the ROI was 49.7%; and a social return on investment (SROI) was found that every $1 invested could generate a return of $3.45.
Introduction
According to the World Health Organization (WHO), non-communicable diseases (NCDs) are one of the severe public health problems worldwide in terms of causing deaths and an overall burden on health economics. Globally, 41 million people die yearly from NCDs, accounting for 74% of all deaths. Deaths from NCDs are found in the age group of 30 to 69 years, known as “premature death,” which was reported 17 million in the age group died of NCDs, and 85% occurred in low-income and middle-income countries. 1 These problems cause the loss of life years and severely affect the economic and social development of many countries. The NCDs situation in Thailand is a significant health problem in line with the global situation. According to the report of Division of Non-Communication Disease, Ministry of Public Health, 2 between 2018 and 2020, the top 4 crude death rates from non-communicable diseases were: diabetes mellitus, hypertension, cerebrovascular disease, and ischemic heart disease which the death rates were 128.3, 134.0, and 131.8 per 100 000 population, respectively.
According to the Sixth National Health Examination Survey 2019 to 2020, 3 the numbers of Thai people have high blood pressure (24.7%). The prevalence of high blood pressure increases with age from 3.3% in the age group of 15 to 29 years. It was 76.8% in the age group of 80 years and over. In terms of health service access in the sixth survey, the result was not good compared to the fifth survey, and the number of people who were not diagnosed with hypertension the prior year had increased from 44.7% in 2014 to 48.8% in 2020. The proportion of health treatment decreased from 49.2 to 47.6%; in addition, patients received treatments and programs to control blood pressure decreased from 29.7 to 22.6%, respectively. Reducing salt and sodium consumption is 1 of the most cost-effective strategies for preventing chronic non-communicable diseases such as high blood pressure, stroke, and kidney failure. The amount of sodium recommended by the World Health Organization 4 was the amount of salt that should not exceed 2000 mg/day. However, a sodium consumption survey of the Thai population in 2009 found that Thai people consumed up to 4351.7 mg of sodium per day, considering consuming salt twice the recommended amount. In 2013 to 2017, it was found that the consumption of ready-made food tended to increase; however, there was no continuous survey after 2009. If people consume salt and sodium in the amount recommended by the World Health Organization, 4 this will prevent the deaths of over 2.5 million people worldwide annually.
Most food that contains high sodium content is salty. 5 However, there are foods that contain high sodium content but it does not taste salty which is known as hidden sodium such as bakery and processed food used in food preservation. Sodium-containing foods can be classified as follows: 1) Processed foods or food preservatives; 2) Seasonings such as salt, soy sauce, and soybean paste; 3) Monosodium glutamate; 4) Various canned foods such as canned fruits, canned fish, and ready-made meals; 5) Semi-finished food such as rice porridge or powder soup; 6) Various desserts with baking powder or baking soda; and 7) Electrolyte drink and fruit juice contained in boxes, bottles, or cans.
The close relationship between hypertension and dietary sodium intake is widely recognized and supported by several studies. The reason for this is that sodium is an essential nutrient that helps to maintain fluid balance and regulate blood pressure. However, excessive sodium intake can cause the body to retain fluid, which increases the volume of blood in the bloodstream, leading to an increase in blood pressure. When blood pressure remains elevated over a long period of time, it can cause damage to the walls of the blood vessels and increase the risk of developing hypertension. 6
Literature review7-11 showed that if the population reduced salt consumption by 3 g/day, it would increase quality of life (Quality-Adjusted-Life-Year: QALYs) to approximately 194 000 to 392 00 health years and savings in medical expenses of approximately 10 000 to 24 000 million dollars per year. This means a return of $6 to $12 per $1 spent on salt and sodium intake control measures and results in 15% reduction in mortality rate from heart diseases and a 40% reduction in cerebrovascular accidents. There are many implementation plans and strategies overseas, and several measures are taken simultaneously, for example public education, health communication, modifying food recipes to use less salt and sodium, and taking strong action on salt and sodium warning labels in many food products.
In Thailand, 12 the Eight National Health Assembly of 2015, the committees have adopted a policy to reduce salt and sodium consumption for the prevention and control of non-communicable diseases (NCDs). The strategic plan to reduce sodium intake among Thailand was established in Thailand during 2015 to 2025 with the aim that the average amount of sodium consumption among population aged 18 years and over is to be reduced by 30% in 2025 compared to 2010, and Thai population should not consume no more than 3046 mg of sodium per day. All provinces are required to find strategic plan to reduce sodium consumption among their population as follows: 1) Modifying or developing local food products to reduce sodium content. 2) Promoting health knowledge and awareness toward health impacts on excessive amount of salt and sodium consumption. 3) Environmental modifications for healthy food choices and food alternatives to avoid excessive sodium intake, and 4) The use of community mechanism and resources to improve quality of life and set policy and measures to reduce salt consumption at community level.
Based on the follow-up data of patients with high blood pressure who registered for health service at a sub-district health-promoting hospital in Muang District, Phayao Province, Thailand (2018-2020). 13 The morbidity rate was 47.23, 46.28, and 56.91%, respectively. The trend was higher in the age group of 40 to 49 years old, and it was also found that the patients had blood pressure less than 140/90 mm Hg, 36.02, 25.6, and 39.06% from the year 2018 to 2020, which was found lower than the target goal at more than 50%. Prevention and control of risk factors toward non-communicable diseases should be driven by all organizations, including public sectors, private sectors, government officials, and public health sectors. Creating and expanding collaborative networks from all stakeholders and everyone in the community would drive the public policy toward salt reduction in food consumption to be put into practice. Salt and sodium intake is 1 of the major risk factors to NCDs; therefore, if people can reduce the use of salt, it will bring positive benefits to health and save money on health expenses. Health promotion, such as educating health knowledge, health communication regarding the dangers of consuming too much “salty” food, creating low-sodium food consumption culture, and monitoring the use of salt-sodium intake among the people in the community should be taken into consideration.
Public health policy development emphasizes on creating a collaborative learning process among people in the community, which makes people aware of their health problems leading to goal and collaborative approach toward better health. Putting policies into practice and monitoring performance to improve or change will promote and encourage people in the community to express their potential and power, realizing their role in health promotion, giving them ability to solve problems, maintain good health, and sustain their knowledge toward health.
Objectives
To study the processes of the policy formation, implementation, and evaluation toward salt reduction in food consumption.
To evaluate the efficiency of the policy on stakeholders at a community level.
Methods
This action research aimed to study the processes of public health policy toward salt reduction in food consumption. The processes were divided into 3 cycles as follows: 1) Public health policy formation; 2) Development of the policy to reduce dietary salt; and 3) Evaluation of the policy efficiency.
Cycle 1: This process emphasized forming the public health policy toward salt reduction in food consumption. Participants aged 18 years and above, living with hypertension and/or at risk of having high blood pressure, were recruited to the study. Sample size calculation was calculated using Yamane’s 14 formula, with a confidence level at 0.05. The total number of 320 participants were obtained and recruited using random sampling draw a lottery. Participations’ names were taken from the list of patients in hospital registration and patients in a risk group with hypertension of the sub-district health-promoting hospital. Their names were written in each label, and drawing a lottery method was performed. The amount of salt in food was randomly checked from fresh market food, ordered food from a village shop, food in the banquet of the village for making merit events, and food eaten in the household.
Research tools for data collection are consisted of:
General demographic characteristics information including age, occupation, health status, and history of hypertension.
Questionnaire on salt and sodium food consumption behavior obtained from the Division of Non-Communicable Diseases, Department of Disease Control. 12
Salinity level detector in food used in this research was Dretec Salt Meter Digital EN900 with an accuracy of ±2%. The working principle of this machine is that the sensor at the tip measures the electrical charge resulting from the conductivity of sodium salt (NaCl) in the liquid. The more salty, the more positively charged the liquid is, and the reading value is higher. It measured as a percentage as follows: volume of watery food (grams) × salinity level (percent) = salt content (grams). The machine reads the value into 7 levels: 0.3, 0.5, 0.7, 0.9, 1.1, 1.3, 1.5
Cycle 2: This process emphasized on the policy development to reduce salt used in food consumption. Participants were head of the village, assistants of the village head, community leaders, public health personnel, village health volunteers, and housewives who involved in the policy development. A total of 50 persons was recruited and participated in this process. The collaborative process started by building mechanism partners using the community mobilization process. Community mobilization is a process of bringing people in the community together as much as possible to raise people’s awareness about a particular program to assist delivery of resources and services to strengthen community participation for sustainability and self-reliance. People in the community came together to discuss and take the policy into consideration. They seek support from community members through village meetings or group discussion. Information obtained from prior process would be presented to community members, such as harmful health effects of salt, mobility rate from high blood pressure and hypertension complications, and relevant NCDs issues. Stakeholders involved in the policy formation and development would listen to each other, share opinions and participate in making rules and agreements in the community, and join hands to comply with the agreement (Policy Implementation).
Cycle 3: This process emphasized on the evaluation of the policy to reduce salt in food consumption. Data collection was obtained from key informants using group discussion including patients with hypertension, community leaders, health personnel from health promoting hospital, village health volunteers, a group of housewives, and village community representatives who joined the public policy advocacy forum.
Data Analysis
Quantitative data, including sex, age, occupation, health status, history of hypertension, illness with high blood pressure, food consumption behavior toward salty food consumption, and level of Salinity in food (Salt meter) were calculated using frequency, percentage, mean, and standard deviation.
The analysis of return on investment (ROI) and social return on investment (SROI).
Rights and Privacy of Participants
This research was endorsed by the Human Research Ethics Committee University of Phayao, number UP-HEC1.2/031/64, dated of certification 20 August 2021. The researcher conducted data collection and strictly complied with research ethics by clarifying the purpose of the research study, process, duration, and expected benefits. The researcher allowed participants to ask questions regarding the research and its process. All participants were clarified about their right and privacy prior to participating the study. They had the right to remain or withdraw from the research at any time. They were ensured that by withdrawing from the study would not affect any received treatment from health care providers. Codes were used in data logs instead of using their real name. In addition, the information obtained from this research would be kept confidential; and presented the data without reference to the name of the sample in any way.
Results
The results showed general characteristics information that majority of participants were female (56.87%), in the age range of 40 to 49 years (49.69%). Almost half of the participants obtained elementary school level (49.69%), having hypertension (14.06%), treatment with medication (100%), and taking medication 1 tablet per day, as shown in Table 1.
General Demographic Characteristics Information of the Participants.

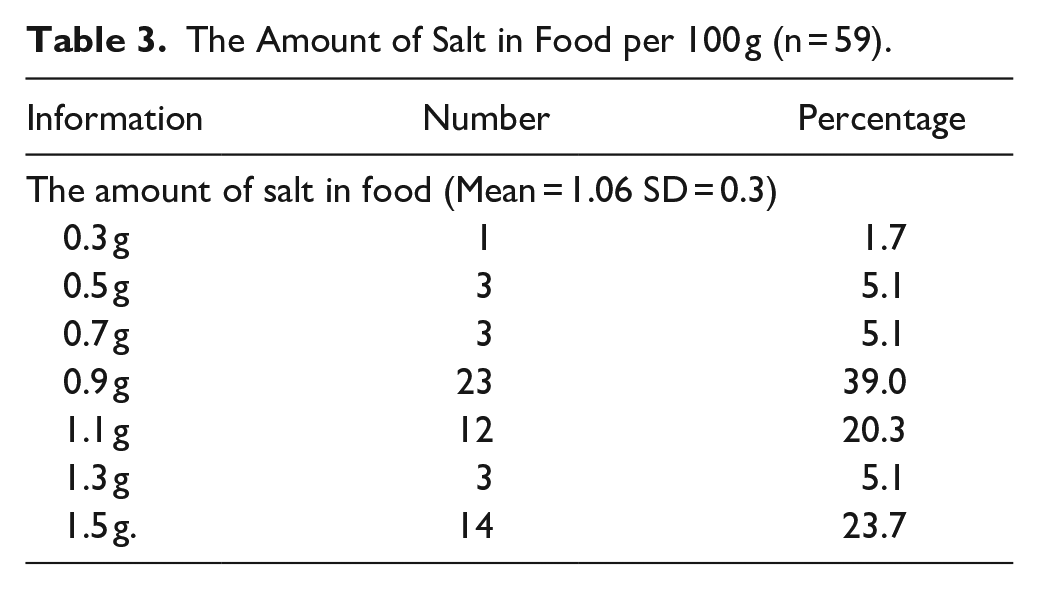
The result showed that participants had high salt and sodium consumption. They added salty condiments to food when eating at a restaurant; for instance, noodles, rice topped with curry, and a single dish (17.8), as shown in Table 2. The highest amount of salt added in food per 100 g was 0.9 g (39.0%), followed by 1.5 g (23.7) as shown in Table 3. The type of food with the highest salt content of 1.5 g per 100 g was self-cooked, as shown in Table 4.
1. Public policy formation process 15 started from identifying the problems with information obtained from health statistics data and from the data collection in the prior process. Information was presented to the community to raise awareness regarding salt and sodium consumption and its health consequences.
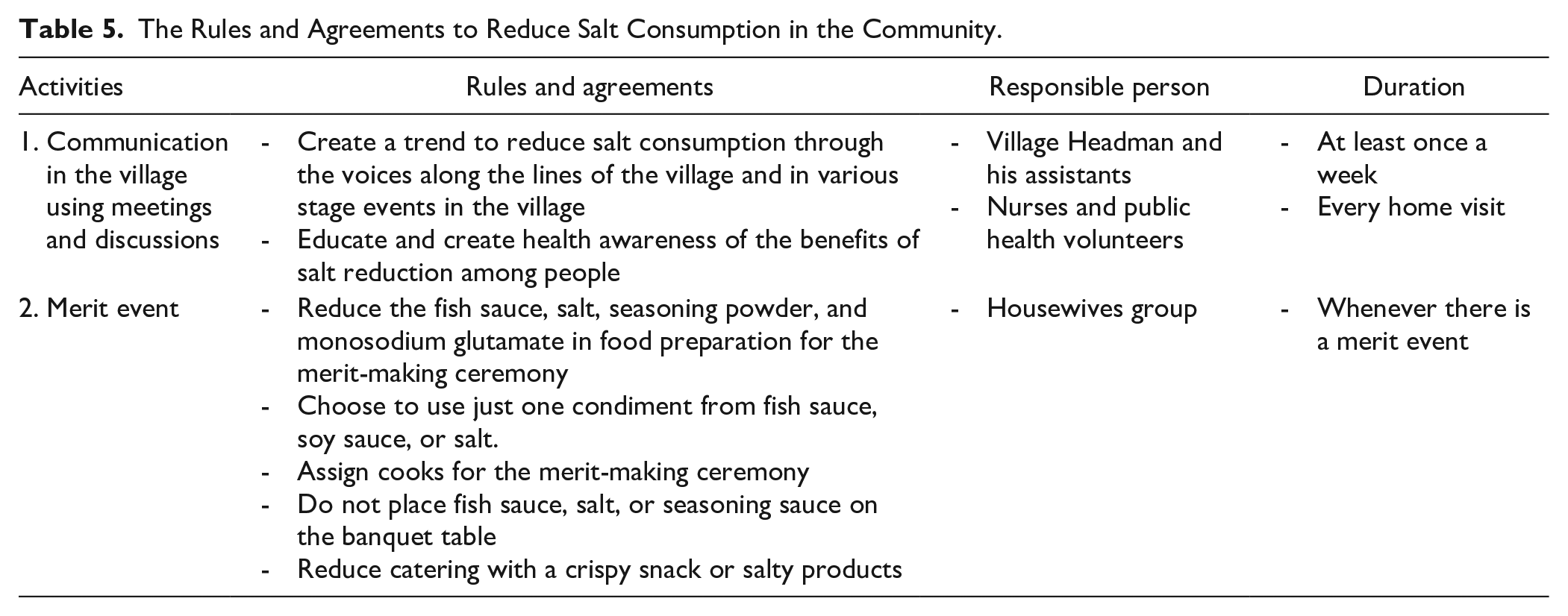
2. The policy was developed with the cooperation of people in the community. Stakeholders were allowed to discuss about health, eating behaviors, salt consumption, and the formation of policy, rules, and agreements through community meeting and group discussions as shown in Table 5.
3. Empowering people including the village head, community leaders, and village health volunteers in the community through health promotion strategies, education and communication on reducing salt consumption to prevent non-communicable diseases. These key people could act as a good role model in the community.
4. Initiated a salt reduction campaign to drive the public health policy and collaborated with local government organizations and related government agency.
5. Monitoring, supervising, and evaluating salt consumption of the people in the community.
Food Consumption Behaviors Toward Food With High Salt and Sodium Content.

The Amount of Salt in Food per 100 g (n = 59).
The Amount of Salt in the Sample Food per 100 g.

The Rules and Agreements to Reduce Salt Consumption in the Community.
From the objective to evaluate the efficiency of the public health policy toward salt reduction in food consumption on stakeholders in the area, to supervise and monitor the progress, problems, and obstacles in the implementation process, it was found that the use of community mechanism to drive the policy employed activities such as to create public space for knowledge sharing and discussion through meetings and group discussion; this allowed various parties in the community to meet, talk, discuss, and share experience. Information obtained from such activities as consumption behaviors, numbers of people with hypertension, numbers of people with high blood pressure and inability to control salt intake, and health complications of hypertension were used to reflect the outcomes. People in the community were together to find solutions using their wisdom and reconciliation to drive the policy into practice under the principle of the synergistic driving force based on knowledge creation of the university and social movement of people in all sectors including public, private, and government sectors linking with the support of local health promoting hospital. This has strengthened the community and created community empowerment through a learning process and decision-making together from all sectors. From monitoring and evaluating the salt consumption of people in the community, it was found that in 2021, patients with hypertension were able to better control their blood pressure which has increased to 47.32%. When the return on investment (ROI) was analyzed, it was found that the ROI was 49.7%; and social return on investment (SROI) was found that every $1 invested could generate a $3.45 (Table 6).
Return on Investment and Social Return on Investment.

Discussion
From the implementation of public health policy toward salt reduction in food consumption, the actions are based on collaboration and mobilization of people in the community. Moreover, an improvement in environment that is conductive to sustainable behavioral change are as follows: 1) Creating a social trend (Social Advocacy) to drive the policy into practice through the announcement from an appointed leader who acts as a role model for health in reducing salt consumption; 2) Providing health information regarding health effects salt consumption and continuous communicating through a public channel such as village news tower, personal social media, public health volunteers, community networks, and a group of housewives in the community; 3) Built strong networks within the community; and 4) Monitoring the process of policy implementation. It was found that the community could manage the health problems by themselves and sustain self-reliance in preventing and controlling of non-communicable diseases. The percentage of hypertension patients with reasonable blood pressure control increased from 36.02, 25.6, and 39.06 to 47.32% (in 2018-2020). This is consistent with the actions of the Nan Municipality, Nan Province. The province has initiated community measures to reduce salt and sodium seasoning in food catering at religious ceremonies, weddings, and cooking in the household. The previous result found that the number of hypertensive patients tended to decrease from 27.50% in 2015 to 26.34, 23.17, 18.70, and 18.50% in 2016 to 2019, respectively.
Biofeedback reflection on salt intake using a salt meter, a tool that shows the amount of sodium in food, is important to raise people’s awareness. It is consistent with the study of Wiriyatanakorn et al 16 that using self-checking tool in conjunction with having an education on dietary salt reduction. Hypertension patients could control their blood pressure better than those who were educated on dietary salt reduction alone.
Using community rules and agreements to reduce salt in food consumption was found to be efficient and cost-effective. Studies in many countries have consistently shown cost-effectiveness and demonstrated the health effects of reducing salt intake, and saving the cost of the health service. According to the research results, when analyzing the return on investment (ROI), it was found to be 49.76%; and the project’s social return on investment (SROI) was found to be every $1 invested generates a return of $3.45. This is consistent with the report of the United States that reducing salt intake in the population by 3 g/day would increase quality of life 194 000 to 392 000 or quality-adjusted life years (QALYs); moreover, it helps saving medical expenses 10 000 to 24 000 million dollars per year. 17 That means using control measures in investing 1 dollar will get a return of 6 to 12 dollars, and reducing salt intake is more cost-effective than taking antihypertensive drugs. In low- and middle-income countries, a 15% reduction in salt intake in the population, 13.8 million deaths will prevent over 10 years at the cost of only $0.4 per person per year.7,18-22
The use of social power to drive solutions is consistent with the recommendations of the World Health Organization. 23 It shows that 3 main strategies that are likely to be the key to success in reducing the amount of sodium consumption among the population are as follows: 1) Modification and development of products to reduce the amount of sodium salt; 2) Educating and creating awareness regarding health and excessively used of dietary salt; and 3) Environmental modification that facilitates healthy food choices and create mechanisms and management processes to reduce salt and sodium consumption.
Conclusion
Using community mobilization is the key to strengthen and empower local communities toward health development, self-reliance, and self-management. It obtains information to reflect the facts or called management by fact and the use of national strategies and relevant plans at different levels as a framework for operations with the help of key person in the community through social mobilization. Such an action allows people in the community to join hands and decide on various problems. These strategies are the driving force for public policies to be put into practice. Community people, including leaders, health personnel, government officers, and people from related agencies, could collaborate through social actions. This creates mutual awareness using a community master plan for salt reduction in food consumption. It is a strategy to promote the health of the people in the community. Effective actions in reducing dietary salt are addressed. Another important lesson learned from this study is the continuous supervision and monitoring people’s performance, including follow-up, returning information to community members, and exchanging experiences from role model who could reduce salt intake at the meetings and group discussions. This enables community people to be aware of their actions toward health. These strategies, including health promotion, health education, environmental modification, and women empowerment, are driving force for social development and implementation of policies practically.
Limitation of the Results
There are some limitations in this study. This research development was performed in area-level mechanisms, the food and the use of salt and sodium may be different from region to region within the country; therefore, the results cannot be generalized to all regions; however, it can be used as a reference considering in a similar context.
Recommendations
There should be education program or health lesson to raise awareness about health impacts of an excessive salt and sodium consumption and non-communicable diseases (NCDs) in all level of educational institutions including child development center, elementary school, secondary, and high schools.
Community health volunteers should be assigned as task to monitor ad measure salt and sodium intake during home visits of their responsible household or at least once a year.
To measure salt and sodium in cooking food in educational institutions and merit event in the community.
There should be an accessible, inexpensive, and simple use of salinity test kits in food, and urine.
To study innovations related salt replacement that is healthier and taste better than actual salt.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was support by a grant from Program Management Unit on Area Based Development (PMUA), Thailand.