
Abstract
Objectives:
To investigate the prevalence and predictors of excessive polypharmacy in geriatric inpatients in Indonesia.
Methods:
This retrospective cross-sectional study included 1533 inpatients over the age of 60 years at Universitas Airlangga Hospital, Indonesia. Effects of a patient’s baseline characteristics on excessive polypharmacy were evaluated using logistic regression analysis.
Results:
Excessive polypharmacy was observed in 133 (8.67%) patients. Ulcer (OR 8.151,95% CI 2.234-29.747, P = .001), cancer (OR 5.551, 95% CI 1.602-19.237, P = .007), and renal diseases (OR 3.710, 95% CI 1.965-7.006, P < .001) were the 3 strongest predictors of excessive polypharmacy. An association between hospital stay of more than 3 days and excessive polypharmacy was identified (OR 2.382, 95% CI 1.109-5.115, P = .026).
Discussion:
One in 12 elderly Indonesians was found to practice excessive polypharmacy. Several chronic conditions and increased length of hospital stay were the factors associated with excessive polypharmacy.
Introduction
The aging population has become a research focus worldwide. Owing to its large population of over 260 million people, the size of the aging population (>60 years of age) in Indonesia is staggering. According to the World Health Organization (WHO), the elderly population in Indonesia is expected to reach 38 million by 2030 and 61 million by 2050. 1 Moreover, Indonesia has the highest number of elderly individuals living on limited old-age income security compared to other low-to-middle-income countries. 1 Although increased longevity indicates an improvement in the overall healthcare status, it also poses challenges with an exponential rise in various chronic and non-communicable diseases. With multiple chronic conditions, the practice of excessive polypharmacy is increasing rapidly. Globally, the prevalence of excessive polypharmacy in the aging population has been reported to vary widely from 7.4% to 43.4%.2,3
Individuals practicing polypharmacy have a higher risk (odds ratio [OR] = 1.86) of experiencing a medication-related problem than those taking fewer medications. 4 Moreover, polypharmacy, especially excessive polypharmacy, has been shown to be associated with an increase in potentially inappropriate medications, medication errors, adverse events, hospitalizations, increased cost of care, and mortality.5,6
Several risk factors of excessive polypharmacy have been identified. Chronic illnesses, diseases, and depression are reported among the risk factors of excessive medication use. 6 Additionally, the diagnosis of 8 or more diseases, frailty, and mental health issues are predictors of excessive polypharmacy. 7 Furthermore, poor self-reported health, diabetes mellitus, depression, pain, heart diseases, and obstructive pulmonary diseases have been identified as risk factors. 8 However, most studies on polypharmacy were conducted in developed countries, while data from low-to-middle-income countries, including Indonesia, are scarce.
Excessive polypharmacy is the most severe form, with the highest effect on patient outcomes. Moreover, previous studies in Indonesia have focused on the prevalence of polypharmacy.9,10 However, no study focusing on excessive polypharmacy in Indonesia has been reported. Additionally, given the higher risk of adverse health outcomes in older patients taking 10 or more medications, it is crucial to investigate the factors contributing to excessive polypharmacy. Therefore, this aimed to investigate the prevalence of excessive polypharmacy and the associated predominant factors in geriatric inpatients in Indonesia. A better understanding of the predictors could help guide prescribing strategies or policies to prevent or mitigate the adverse outcomes of excessive polypharmacy.
Methods
Study Design, Setting, and Participants
This retrospective, cross-sectional study involved geriatric inpatients admitted to the Airlangga University teaching hospital, among Indonesia’s largest university-affiliated teaching hospitals in Surabaya City, the capital of the Indonesian province of East Java and the second-largest city in Indonesia. The hospital serves approximately 12 million people and is also a referral hospital for the East Java region. The chosen hospital is a class B general hospital with at least 200 beds with the facilities and capabilities of specialist and sub-specialist medical services. The hospital has facilities such as general medical services, emergency services, basic specialist medical services, specialist medical support services, other specialist medical services, oral dental specialist medical services, sub-specialist medical services, nursing and midwifery services, clinical support services, as well as non-clinical support services. As the hospital is a university-affiliated teaching hospital, it was more convenient to collect data from the hospital. We screened all the geriatric patients’ medical records to minimize selection bias. We included all patients aged ≥60 years who were admitted to the hospital, receiving ≥5 oral medications simultaneously during the patient’s stay in the hospital 11 from July 2018 to October 2019 and had complete medical records included in the study. Patients who underwent surgery and were admitted to the intensive care unit (ICU) were excluded because they typically require more medications for recovery.12,13 We also excluded patients whose medical records were incomplete. The above criteria were determined considering the study time and resources. Of 17 329 patients, 15 796 were excluded (age <60 years: n = 13 705; patients taking <5 medications, admitted to the ICU, or undergoing surgery: n = 2011; patients with incomplete medical records: n = 80). In total, 1533 patients met the inclusion criteria of the study. The cohort selection flow chart of the study is presented in Figure 1.

Flow chart of study cohort selection.
Data Source and Collection
The hospital database served as the primary information source. An electronic master file of patients admitted to the hospital was screened based on the inclusion and exclusion criteria (Figure 1). The profiles of the patients who met the inclusion criteria were recorded in a structured record form for data analysis. Data obtained for this study included age, sex, marital status, education level, employment status, city of residence, admitting diagnosis, length of hospital stay, and the number and names of medications used during the hospital stay. The names of medications used were extracted and subsequently coded with the Anatomical Therapeutic Chemical (ATC_level 1) classification system of the WHO (updated November 25 2022). 14
Variables
Demographic and clinical variables
Demographic and clinical variables were obtained from the patient’s medical record profile. For the demographic variables age, the cutoff values used as 60 or more years, as individuals aged 60 or more are considered elderly in Indonesia, 15 that is further grouped to 60 to 74 years as young old, 75 to 84 years as old, and 85 years or above as oldest- old. The other variables include sex, marital status (single, married, or divorced), education level (no school, school, or university), employment status, and city of residence (Surabaya or outside Surabaya). Clinical variables of interest included patients’ reason(s) for admission to the study setting, presence of comorbidity, length of hospital stay, and Charlson comorbidity index (CCI) score, a total score of assigned values based on the number and severity of a patient’s diseases.16,17 Furthermore, diagnoses of myocardial infarction, chronic heart failure, peripheral vascular disease, cerebrovascular accident, plegia, chronic obstructive pulmonary disease (COPD), diabetes mellitus, diabetes with end-organ damage, renal disease, mild liver disease, severe liver disease, ulcer, cancer, metastases, dementia, rheumatoid arthritis, human immune deficiency virus, hypertension, and other conditions at the time of admission were recorded from the patient’s medical records profile.
Excessive polypharmacy
The medical profiles of the patients were thoroughly reviewed, and the number of drugs administered to the patients during their hospital stay was recorded. The key dependent variable of the study was excessive polypharmacy. Although the term’ excessive polypharmacy’ is commonly used, there is a lack of consensus on its exact definition. We defined excessive polypharmacy as the use of 10 or more medications in accordance with previous studies.11,18,19
Statistical Analysis
First, we analyzed the descriptive statistics of all patients, and the results were presented as the number of patients and percentages. The patients were divided into non-excessive polypharmacy and excessive polypharmacy groups. The demographic and clinical variables of the patients were compared between the 2 groups. Pearson’s chi-squared test or Fisher’s exact test was used where appropriate to determine the significance of the relationships between the variables and excessive polypharmacy. The use of ATC_level 1 substances was also compared between the non-excessive and excessive polypharmacy groups. Pearson’s chi-squared test was used to evaluate the relationship between the use of ATC_level 1 substances and excessive polypharmacy. A simple bivariate logistic regression analysis (crude model) was performed to determine the direct influence of patients’ baseline characteristics on excessive polypharmacy. A multivariate binary logistic regression analysis (adjusted model) was performed to assess the correlation of the patient’s demographic and clinical characteristics with polypharmacy. The crude odds ratio (COR) for the crude model, adjusted odds ratio (AOR) for the adjusted model, and the 95% confidence interval (CI) were calculated. For all tests, the statistical significance was set at P < .05. We used the statistical package IBM SPSS, version 25 for Windows 10 (IBM Corp., Armonk, NY, USA), to analyze the data.
Results
Patient Characteristics
The patient characteristics are shown in Table 1. A total of 1533 patients, 769 (50.2%) males and 764 (49.8%) females, were included in the data analysis. The majority of patients (78.2%) were in the age group of 60 to 74 years. Most (87.2%) of the patients received education at a high-school diploma or lower level. More than half of the population (61.8%) was unemployed. There were 500 (32.6%) patients whose CCI scores were ≥3. Comorbidity was found in 908 (59.2%) patients. Most patients (89.2%) stayed in the hospital for 3 or more days. The mean (± standard deviation [SD]) number of medications consumed was 6.29 ± 2.095. Excessive polypharmacy was observed in 133 (8.67%) patients. The sociodemographic and clinical characteristics of all patients are shown in Table 1, with separate data and analysis for patients practicing and not practicing excessive polypharmacy. The patients in the excessive polypharmacy group had significantly higher comorbidities (72.2%vs 57.4%, P < .001). Renal diseases also significantly correlated with excessive polypharmacy, with a higher proportion of patients diagnosed with renal disease practicing excessive polypharmacy (14.3%vs 6.1%, P < .001).
Demographic and Clinical Characteristics of Geriatric Inpatients According to the Use of Excessive Polypharmacy (n = 1533).

Abbreviations: COPD, chronic obstructive pulmonary disease; HIV, human immune deficiency virus.
Pearson’s chi-squared test.
Fisher’s exact test.
Patterns of Drug Use
The ATC classification of drugs used by the study population is presented in Table 2. Overall, drugs related to the alimentary tract and metabolism were the most commonly used (80%), followed by drugs acting on the cardiovascular system (77.4%). In the excessive polypharmacy group, the 3 most frequently used drug types were those serving on the cardiovascular system (88%), alimentary tract and metabolism (88.7%), and anti-infective drugs for systemic use (65.4%).
Percentage of Patients Using Substances, by Function of the Anatomical Therapeutic Chemical Classification System (ATC_1), According to Excessive Polypharmacy Status (n = 1533).
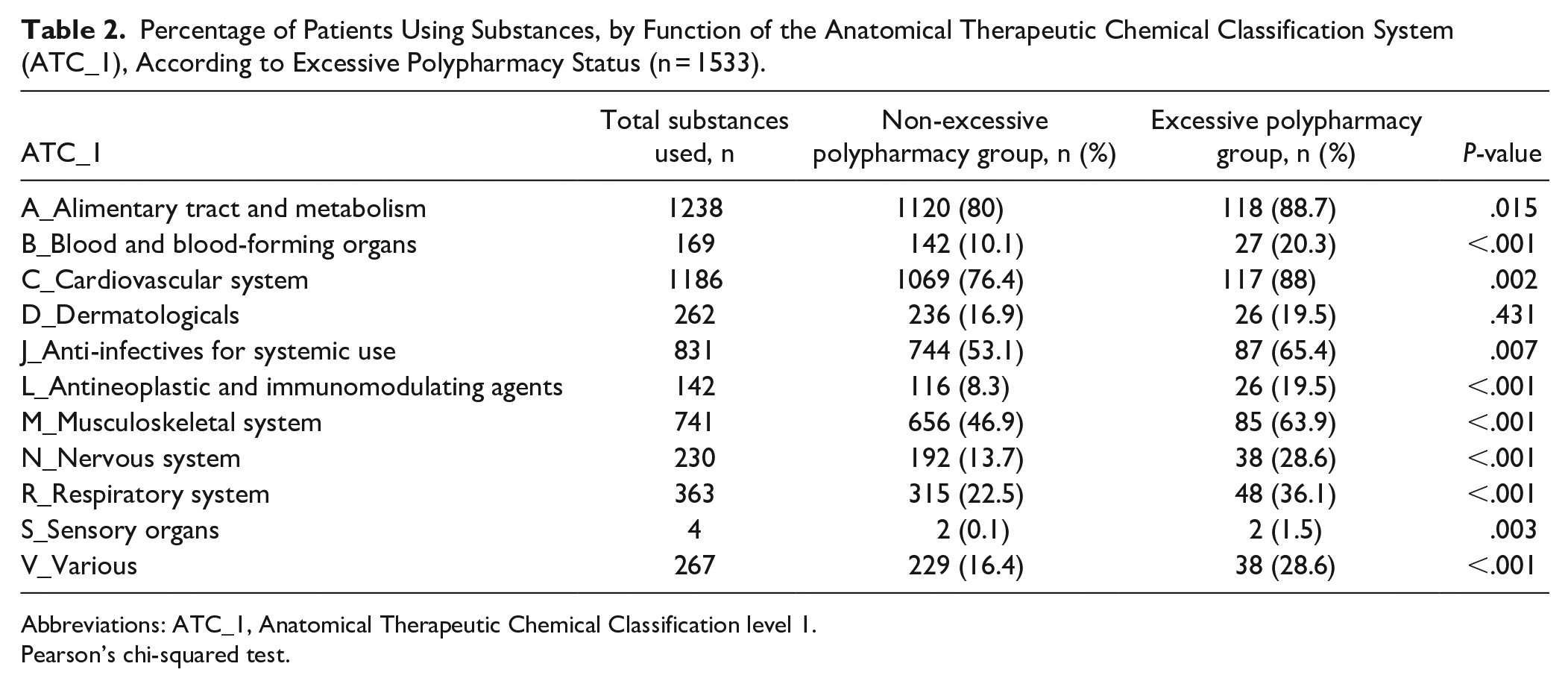
Abbreviations: ATC_1, Anatomical Therapeutic Chemical Classification level 1.
Pearson’s chi-squared test.
Figure 1 shows the 6 major classes of drugs prescribed frequently during hospital stays. A therapeutic class anti-hypertensive was prescribed 1231 times, followed by anti-ulcer and antibiotic classes, 1156 and 986 times, respectively (Figure 2).
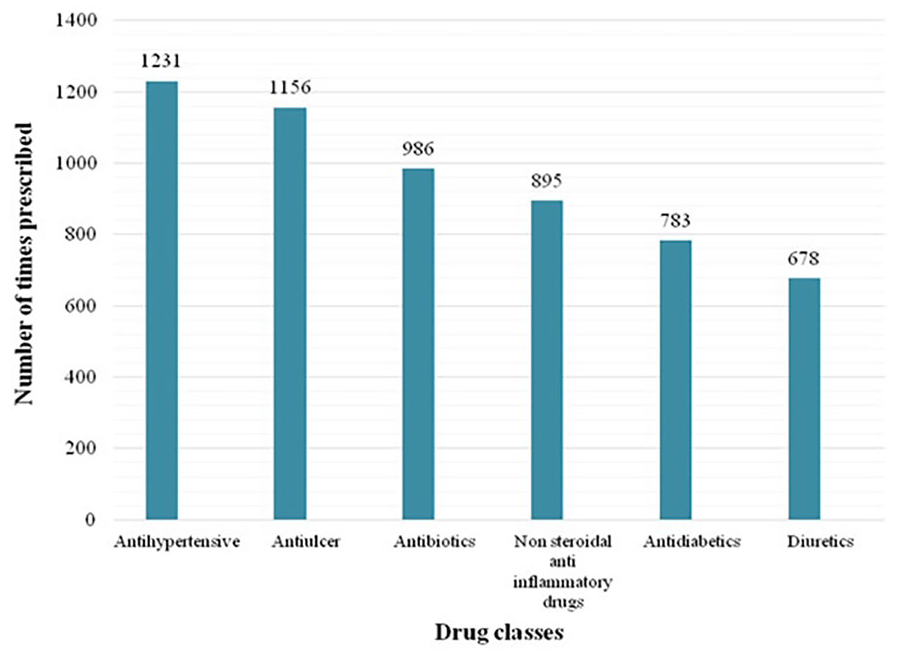
Top 6 frequently prescribed drug classes during the hospital stay.
Factors Associated With Excessive Polypharmacy
The factors associated with excessive polypharmacy are shown in Table 3. The results of multivariate binary logistic regression (adjusted model) showed that patients who stayed in the hospital for 3 or more days had a high risk (OR = 2.382, 95% CI = 1.109-5.115, P = .026) of practicing excessive polypharmacy. In addition, different diseased conditions were found to be associated with excessive polypharmacy. Ulcers (OR = 8.151, 95% CI = 2.234-29.747, P = .001) and cancer (OR = 5.551, 95% CI = 1.602-19.237, P = .007) were associated with a very high risk of excessive polypharmacy. Among the more common chronic diseases, renal diseases (OR = 3.710, 95% CI = 1.965-7.006, P < .001), diabetes with end-organ damage (OR = 2.914, 95% CI = 1.147-7.405, P = .025), diabetes mellitus (OR = 2.395, 95% CI = 1.514-3.790, P < .001), cerebrovascular disease (OR = 2.330, 95% CI = 1.426-3.808, P = .001), hypertension (OR = 1.951, 95% CI = 1.174-3.244, P = .01), and COPD (OR = 1.815, 95% CI = 1.014-3.250, P = .045) were identified as significant predictors of excessive polypharmacy.
Determinants of Excessive Polypharmacy Based on Logistic Regression Analysis (n = 1533).

Abbreviations: OR, odds ratio; CI, confidence interval; CCI, Charlson comorbidity index; LOS, length of hospital stay; COPD, chronic obstructive pulmonary disease; HIV, human immune deficiency virus.
P value <.05.
The results of the simple binary logistic regression analysis (crude model) showed that cerebrovascular diseases (OR = 1.840, 95% CI = 1.224-2.765, P = .003), diabetes mellitus (OR = 1.857, 95% CI = 1.277-2.614, P = .001), renal diseases (OR = 2.578, 95% CI = 1.513-4.394, P = < .001), ulcer (OR = 3.308, 95% CI = 1.063-10.293, P = .039), and hypertension (OR = 1.694, 95% CI = 1.181-2.430, P = .004) are the independent factors associated with excessive polypharmacy.
Discussion
This is the first study to focus on the prevalence and predictors of excessive polypharmacy among geriatric inpatients in Indonesia. Our study’s prevalence of excessive polypharmacy (8.67%) is consistent with reports from different countries. Extensive, cross-sectional studies from Ireland (using electronic pharmacy claims), Scotland (using electronic primary healthcare records), and Sweden (a register-based cohort study) have reported a prevalence of excessive polypharmacy (defined as the use of >10 medications) in the range of 7.4% to 11.7%.20,21 Data from a large observational cohort study of patients presenting at the emergency department in Italy indicated that 17.8% of the patients practiced excessive polypharmacy.3,4 Another study from Italy on patients admitted to 12 different hospitals reported a 13% prevalence of excessive polypharmacy. 22 However, reports from Asian countries showed varied results. A recent analysis based on the national claim database of Taiwan reported that the prevalence of excessive polypharmacy among ambulatory patients was 5.4%. 23 Another study from Japan based on national pharmacy claims data reported a prevalence of 12.3%, 35.8%, and 43.3% among those aged 50-64, 65-79, and >80 years, respectively. 24 The discrepancies in the prevalence of excessive polypharmacy among various studies may partially be explained by differences in the study setting and characteristics of the study populations, especially age. One factor that may contribute to differences in the results of various studies is access to medications. Economically advanced countries may have a higher prevalence of excessive polypharmacy due to easier drug access.
The most commonly used drug types in the excessive polypharmacy group were those acting on the cardiovascular system in line with the studies conducted in Belgium and Finland.25,26 The Alimentary tract and metabolism and anti-infective drugs for systemic use were the second and third most prescribed drugs in line with the previous study in Canada, where the use of these drugs was relatively higher. 27 In addition, anti-hypertensives were the most prescribed drugs during a hospital stay in our current study, followed by anti-ulcers, consistent with the study conducted in Japan. 28 The American College of Cardiology and the American Heart Association stated that it is reasonable to use anti-ulcers in elderly patients receiving anti-hypertensive drugs. 29 Therefore, the current study also supports using anti-ulcers with anti-hypertensive medications.
We did not find any apparent positive relationship between increasing age and excessive polypharmacy; however, a previous study showed that excessive polypharmacy increased with increasing age. 30 As the current study comprised 4.4% of patients aged 85 years or older, this number is relatively small, potentially leading to an insignificant relationship between old age and excessive polypharmacy. Similar to another study, 31 we found that the CCI score and comorbidity correlate with polypharmacy. The findings support prior studies showing that a high CCI score increases the number of drugs needed. 32 We found that hypertension was the most common chronic disease in our population, consistent with national disease statistics showing that more than one-third of Indonesians are afflicted by hypertension. 33 These findings corroborate those of a previous study on elderly individuals on polypharmacy.34,35 Numerous chronic diseases are associated with excessive polypharmacy.36,37 Similar to the findings of previous studies from developed countries,20,38 our study confirms that chronic diseases, including renal diseases, diabetes, cardiovascular diseases, and COPD, are prominent among Indonesian patients receiving excessive polypharmacy. Additionally, we identified ulcers (OR = 8.151) and cancer (OR = 5.551) as potential excessive polypharmacy predictors, similar to the findings of a large population study conducted in Japan. 39 Differences in disease epidemiology between Western and Asian countries might partially explain this result.
Patients who stayed in the hospital for 3 days or longer were more likely to receive excessive polypharmacy, consistent with a previous study’s findings.38-40 Patients in the hospital for an extended period may have been more seriously unwell, requiring many drugs simultaneously. A recent study in New Zealand demonstrated a direct relationship between the mean number of medicines prescribed and the increased duration of hospital stay. 41 Understanding the clinical characteristics of elderly patients practicing excessive polypharmacy and evaluating the risk factors contributing to excessive polypharmacy are highly relevant due to Indonesia’s rapidly growing geriatric population. The current study contributes to our understanding of the factors associated with excessive polypharmacy, which may help the development of target strategies to reduce excessive medication use in vulnerable populations.
This study has some limitations. First, this was a single-center study conducted in a relatively metropolitan area. Therefore, the generalizability of this study for a country as large and diverse as Indonesia may be limited. A multi-center nationwide survey may be needed to understand the extent and pattern of excessive polypharmacy in the country. To reduce selection bias, a multicentered randomized hospital study including different category hospitals like primary care, secondary care, and tertiary care needs to be conducted. Second, due to the study’s retrospective nature, we could not investigate adverse polypharmacy outcomes as limited information was available in the patient’s record profiles.
Besides, as the study investigates the factors associated with excessive polypharmacy, thus we exclude patients with less than 5 medications as the number of included patients might be much higher, keeping in mind the study timeline and resources that might be another shortcoming of the study. Furthermore, incomplete information, inaccurate data, or miscoding might have potentially occurred, despite our best efforts to minimize these problems. Additionally, we could not capture other relevant information such as patients’ lifestyles, self- and home-used medication, or medication received from other healthcare providers. Thus, an underestimation of excessive polypharmacy could have occurred. Future research with a prospective or concurrent design may help solve this issue by comprehensively capturing the overall medications used by the patients from various sources.
Moreover, the patient’s records were extracted and screened from the electronic medical records based on the inclusion criteria; therefore, we did not have information about the excluded patients. Hence, it is not possible to compare the characteristics of the included and excluded participants. However, we believe that the study results provide fruitful information about the use of excessive polypharmacy in the Indonesian elderly population, although multicentered research about excessive polypharmacy is warranted.
The study concluded that one in 12 elderly Indonesians admitted to the hospital practice excessive polypharmacy. The problem may become more severe with the increasing elderly population and the increased availability of pharmaceutical products in the country. Certain diseases, such as ulcers, cancers, renal disorders, and other common chronic diseases like diabetes and hypertension, were strongly linked to excessive polypharmacy. A hospital stay of more than 3 days was also a predictor of excessive polypharmacy in this population. Further research on the effects of excessive polypharmacy on clinical, economic, and humanistic outcomes is warranted to gauge the burden of this critical issue on Indonesia’s health system. Such studies’ results can guide the medication policy and optimize prescribing for geriatric patients.
Footnotes
Author Contributions
All authors contributed to the study conception and design. Material preparation, data collection, and analysis were performed by SF, JK, and EZ. EZ managed to secure the funding for this study. The first draft of the manuscript was written by Shah Faisal, and all authors (EZ, JK, SN, SAK, and GN) have commented on the previous versions of the manuscript. All authors have read and approved the final version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported from Universitas Airlangga for the research grant (Hibah Riset Mandat NO: 722/2021). The authors thank all medical record staff at Universitas Airlangga Hospital, Surabaya, Indonesia, for assistance in data collection.
Ethics Statement
This study protocol was approved by the Research Ethics Committee of Airlangga University Hospital, Surabaya, Indonesia (reference number: 164/KEP/2020). The requirement to obtain written informed consent was waived due to the retrospective nature of the study.
Data Availability Statement
The data supporting this study’s findings are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.