
Abstract
Introduction:
Social determinants of health (SDoH) influence health outcomes and screening for health-related social needs (HRSN) is a recommended pediatric practice. In 2018, Denver Health and Hospitals (DH) implemented the Accountable Health Communities (AHC) model under the Centers for Medicare and Medicaid Services (CMS) and began using the AHC HRSN screening tool during selected well child visits (WCVs) at a DH Federally Qualified Health Center (FQHC). The current evaluation aimed to examine the program implementation and identify key lessons learned to inform the expansion of HRSN screening and referral to other populations and health systems.
Methods:
Patients who completed a WCV between June 1, 2020 and December 31, 2021 (N = 13 750) were evaluated. Frequencies and proportions were used to describe patient characteristics of those that had a WCV, were screened, and received resource information. Multivariable logistic regression models with odds ratios (OR) and 95% confidence intervals (CI) were used to determine the association between patient characteristics and completing HRSN screening and provision of resource information.
Results:
The screening tool was completed by 80% (n = 11 004) of caregivers bringing children to a WCV at the DH Westside Clinic, with over one-third (34.8%; n = 3830) reporting >1 social need. Food insecurity was the most common concern (22.3%; n = 2458). Non-English, non-Spanish (NENS) speakers were less likely to be screened (OR 0.43, 95% CI 0.33, 0.57) and less likely to report a social need (OR 0.59, 95% CI 0.42, 0.82) than speakers of English, after adjusting for age, race/ethnicity, and health insurance.
Conclusions:
A high rate of screening indicates feasibility of administering HRSN screenings for pediatric patients in a busy FQHC. More than a third of patients reported one or more social needs, underscoring the importance to identity these needs and the opportunity to offer personalized resources. Comparatively lower rates of screening and potential underreporting among NENS may be indicative of the availability and acceptability of current translation procedures as well as how the tool translates linguistically and culturally. Our experience highlights the need to partner with community organizations and involve patients and families to ensure SDoH screening and care navigation is part of culturally-appropriate patient-centered care.
Keywords
Introduction
The social conditions in which individuals live, work, and play, or social determinants of health (SDoH), influence health at all stages of the lifecourse.1,2 Healthcare systems have become increasingly aware of the intrinsic association of these factors, influencing a call to action to both assess and address these drivers, also termed health-related social needs (HRSN), as part of the essential community-clinical care continuum to optimize health and mitigate health disparities. 3
Well-child visits (WCVs) can serve as a cornerstone for optimizing not only child, but family health and wellness. In addition to conducting routine screening, counseling, and preventive care, WCVs can serve as a critical touchpoint for families that may not otherwise be routinely accessing the healthcare system.4,5 This is particularly important for safety-net institutions/Federally Qualified Health Centers (FQHCs) who provide care to a large number of un- and under-insured persons.
The American Academy of Pediatrics first recommended screening for SDoH as part of patient-centered care in 2016; since that time several professional guidelines, recommendations, and toolkits have been developed to support the integration of SDoH screening and resource provision into healthcare. 5 Despite the evidence, health systems have been slow to adopt HRSN screening 6 due to demands for practitioner and staff time, limitations on knowledge and access to community based organizations, interoperability of electronic health records and social services, and concerns about ethical and unintended consequences of screening without training or capacity to adequately meet identified needs.7,8
In 2018, Denver Health and Hospital Authority (Denver Health: DH) partnered with Denver Regional Council of Governments (DRCOG) as one of multiple clinical sites to implement the Accountable Health Communities (AHC) model under the Centers for Medicare and Medicaid Services (CMS) and began using the AHC HRSN screening tool in one of the system’s FQHCs during selected WCVs. 2 The CMS Innovation Center, recognizing the integral association between social needs and health, has started to require HRSN screenings and referrals to resources in healthcare systems. 9 With the goal of equitable health outcomes, CMS is expanding this work through facilitating screening and coordination of resources with the AHC and other models.
This project aimed to evaluate the program implementation and identify key lessons learned to inform expansion of HRSN screening and referral to other populations and health systems.
Methods
Setting and Population
DH is an integrated, academic, safety-net health system located in Denver, Colorado that includes a Level 1 Trauma Center, acute care medical center, and a network of 11 FQHCs and 19 school-based health centers. The current analysis included all pediatric (<19 years) patients who attended a well-child visit (WCV) between June 1, 2020 and December 31, 2021 at the DH Westside Pediatric Clinic (Westside), a division of an FQHC that serves approximately 35 000 children annually. During this period that coincided with the COVID-19 pandemic, DH Westside operated at usual capacity for well child visits of all ages. However, the volume of patients allowed in waiting rooms was limited. When possible, patients checked in, completed paperwork, and waited for room availability from their vehicle. Patients without vehicles completed check in with the usual in person process.
Program Implementation
In May 2018, DH Westside implemented screening for HRSN as standard care during WCVs occurring at 2 months, 1 year, and annually for children >1 year, to meet the AHC requirement of yearly screening 2 and to ensure consistent opportunities to support families with young children. AHC HRSN screening tool 10 was used to identify needs across 5 domains (living situation, food, transportation, utilities, and safety). DH Westside provided the tool in English and Spanish and administered to the child’s primary caregiver or accompanying adult via a paper survey during registration. When possible, medical interpreters from the language line, available in 240+ languages, administered the AHC HRSN to patient families with other preferred languages (non-English, non-Spanish: NENS).
Patient families indicating ≥1 social need were provided resource information as part of the After Visit Summary. In addition, 2 dedicated care navigators (CNs) familiar with many of the cultures and languages of the patient population conducted outreach to patient families who had ≥1 need and who had reported ≥2 emergency department (ED) visits for the child in the previous year. Together, the care navigators spoke 6 languages and leveraged the language line for any other languages to offer CN services, including referral assistance, care follow-up, and developing a personalized action plan. No further action or loop closure was done.
Data Sources
Data from the AHC HRSN served as the primary data source for the current analysis. Electronic data entry for HRSN screening from May 2018 to May 2020 was restricted to CMS Medicaid beneficiaries and only recorded within the CMS database. Systematic entry of the HRSN screening data for all patients into the DH electronic medical record (EHR), Epic, started in June 2020. Due to the greater reliability of patient sociodemographic and clinical information in Epic and inclusive patient population, the current analysis included patients with data in Epic between June 1, 2020 and December 31, 2021. Additional patient sociodemographic data including age, sex, race, ethnicity, preferred language, geographic residence, and insurance payor was also obtained from the EHR.
Statistical Analyses
Frequencies and proportions were used to describe the population and characteristics across all steps of the cascade: screening, identifying needs, offering resources, meeting eligibility for navigation, and offering care navigation services. Multivariable logistic regression models with odds ratios (OR) and 95% confidence intervals (CI) were used to determine the association between patient characteristics and each step in the cascade. All analyses were conducted using Stata version 17.0.
Ethics
This project was reviewed by the DH Quality Improvement Review Committee, which is authorized by the Colorado Multiple Institutional Review Board at the University of Colorado, Denver, and was determined not to be human subjects research, not requiring IRB review.
Results
Between June 1, 2020 and December 31, 2021 13 750 children had a WCV at DH Westside, and 80% (n = 11 004) completed the HRSN screening (Figure 1). Over one-third (34.8%; n = 3830) reported at least one social need. Of patients with a social need, 79.2% (n = 3032) were offered resource information. A small proportion (6.1% of those with ≥1 need, 2.1% of those screened; n = 232) were eligible for care navigation (≥2 ED visits in the past year). Care navigation services were offered to 60.3% (n = 140) of eligible patient families.

Patient population at Denver Health Westside Clinic by proportion screened and resources and services provided.
Almost one-third of WCVs were among children aged 0 to 4 (31.3%; n = 4302), with similar distribution among male and female patients (Table 1). Most (81.9%) children identified as Hispanic, Latinx, or of Spanish Origin (Hispanic) and were recipients of Medicaid (88.7%).
Sociodemographic Characteristics of Patients With Well-Child Visits (WCVs) Stratified by Health-Related Social Needs (HRSN) Screening Data.
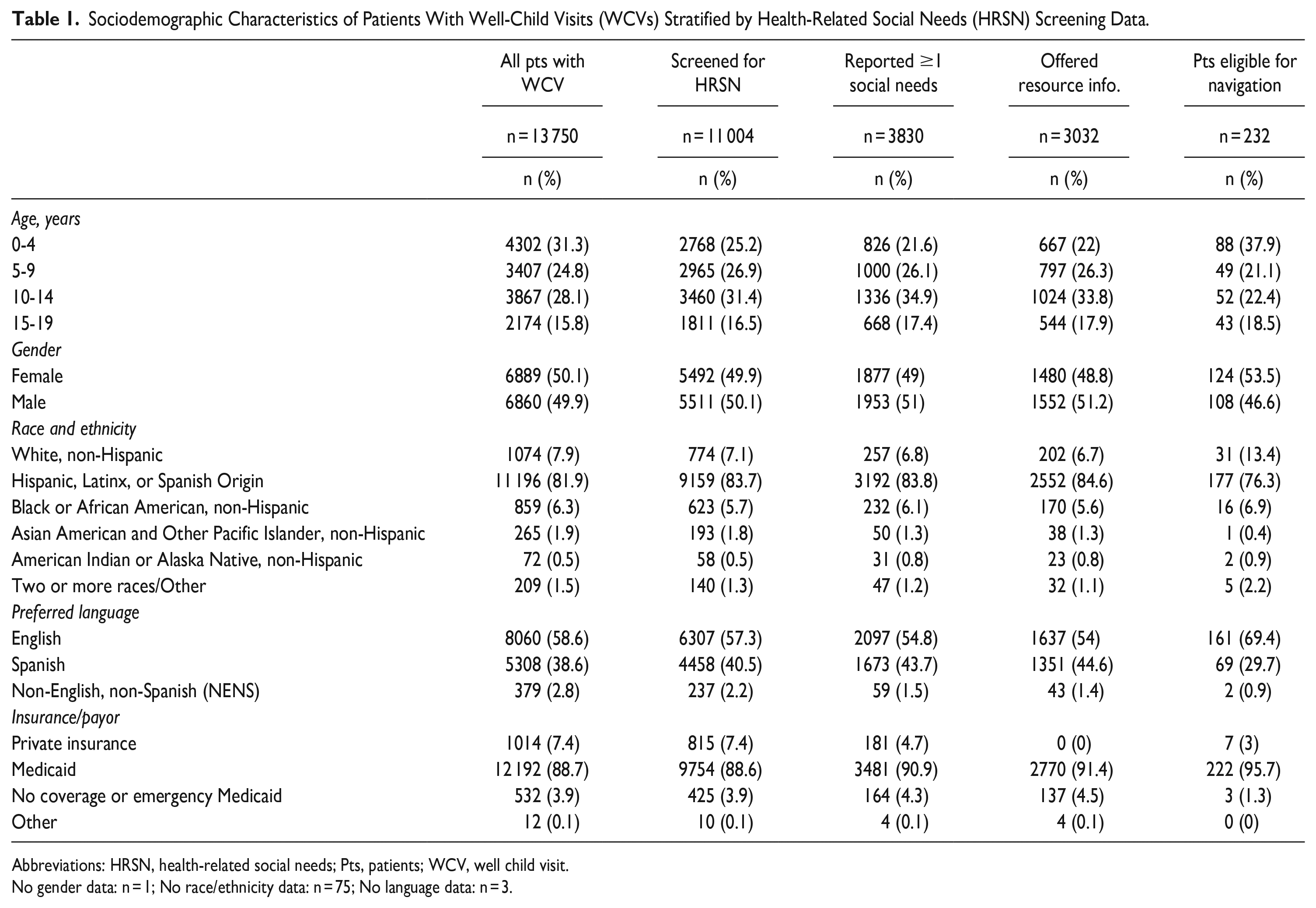
Abbreviations: HRSN, health-related social needs; Pts, patients; WCV, well child visit.
No gender data: n = 1; No race/ethnicity data: n = 75; No language data: n = 3.
HRSN Screenings
Multivariable analysis identified that older children were 2.63 to 4.59 times more likely to be screened than children 0 to 4 years of age, and patients who identified as Hispanic completed screenings 34% more often than individuals who identified as White, non-Hispanic (ORadj 1.34, 95% CI 1.15, 1.57) (Table 2). NENS patient families were also significantly less likely to be screened compared to patients with English as their preferred language (ORadj 0.43, 95% CI 0.33, 0.57). Patients with no insurance or who relied on emergency Medicaid completed screenings 30% less often than patients with private insurance (ORadj 0.70, 95% CI 0.53, 0.92) when controlling for age, race/ethnicity, and language.
Multivariable Associations Between Pediatric Patient Sociodemographic Characteristics and Screening for HRSN; Reporting ≥1 Social Need; Being Offered Resource Information. Values are Odds Ratios (OR) and 95% Confidence Intervals Adjusted for All Other Variables in the Model.

Abbreviation: HRSN, health-related social needs.
Identified Social Needs
Food insecurity was the most common social need (22.3% of those screened; n = 2458). The proportion of patients indicating a need in each of the 5 domains significantly varied by patient racial/ethnic group (all P < .01; Figure 2).

Proportion of patients screened that reported ≥1 social need listed by need type and race/ethnicity.
In multivariable models, compared to patients aged 0 to 4, older patients were more likely to report a social need (range ORadj 1.18-1.45) (Table 2). Patients who identified as American Indian or Alaska Native, non-Hispanic were almost 2 times more likely to report a social need compared to White, non-Hispanic patients (ORadj 1.94, 95% CI 1.13, 3.33). Speakers of Spanish were 17% more likely (ORadj 1.17, 95% CI 1.07, 1.27) and NENS were 41% less likely to report a social need (ORadj 0.59, 95% CI 0.42, 0.82) when compared to speakers of English. Patients insured by Medicaid and those with no coverage or emergency Medicaid were 2-fold more likely to report a social need than those using private insurance.
Resource Information
Patients aged 10 to 14 were 33% less likely to be provided resource information than those aged 0 to 4 (ORadj 0.77, 95% CI 0.61, 0.95). Individuals covered by Medicaid were 88% more likely (ORadj 1.88, 95% CI 1.35, 2.61) and individuals with no coverage or emergency Medicaid were 2-fold more likely (ORadj 2.41, 95% CI 1.41, 4.13) to be provided resources than patients with private insurance.
Care Navigation
When comparing patients aged 0 to 4 to other groups, patients aged 5 to 9 and 10 to 14 were significantly less likely to be eligible for care navigation services (respectively, ORadj 0.54, 95% CI 0.38, 0.77; ORadj 0.53, 95% CI 0.37, 0.75). Patients identifying as Hispanic (compared to White non-Hispanics: ORadj 0.52, 95% CI 0.34, 0.78) and whose preferred language was Spanish (compared to English: ORadj 0.71, 95% CI 0.53, 0.97) were significantly less likely to be eligible for care navigation. Individuals who used Medicaid were 3-times more likely to be eligible for navigation than those using private insurance (ORadj 3.3, 95% CI 1.53, 7.09). Among eligible patients, there were no significant associations identified between patient characteristics (age, race/ethnicity, language, insurance type) and offering care navigation services (data not shown).
Discussion
These findings demonstrate that it is possible to achieve a high level of HRSN screening (80%) in a busy FQHC pediatric practice. This rate of screening is slightly higher than what has been previously reported in pediatric practices (range 46%-63%)6,11,12 and may be partially attributable to standardized practice to include screening as part of registration and supplemental grant funding to support clinic care navigation. In addition, our analysis included the peak of the COVID-19 pandemic and lockdown, during which time the unemployment rate rose exponentially, and families faced substantial economic and social challenges. 13 Over a third of patients reported one or more needs, underscoring the importance of collecting this information and ensuring healthcare personnel are equipped with resources to effectively provide information to address identified needs. Food insecurity was the most reported need (22.3%), though needs varied by demographic group. The proportion of patient families reporting food insecurity was slightly higher than the US population (10.2%) 14 and other pediatric settings (range 15.8%-19.6%).15,16
Children 0 to 4 comprise the largest proportion of WCVs but had lower rates of screening. Lower screening may be due to prioritizing completion of developmental screenings and minimizing paperwork burden for caregivers. Many social support programs, including Women, Infants, and Children (WIC), 17 focus on families with younger children (<5), so there may be a perception of less need for screening and when screened, fewer needs identified. In addition, young children (0-4) were more likely to qualify for navigation (≥1 more social need and ≥2 ED visits); more frequent ED usage among this age group has been reported previously. 18
While patients identifying as Hispanic and speakers of Spanish were more likely to report ≥1 social need, they were less likely to be eligible for care navigation than White non-Hispanics and speakers of English. This may be more representative of differential ED usage than true patient needs. Care navigation eligibility was based on reporting 2 or more ED visits in the previous year in combination with an identified social need. Both a systematic review and pooled cross sectional suggest less emergency system usage among Hispanics than non-Hispanic Whites.19,20
NENS speakers were less likely to be screened and to report a need. This lower completion rate and potential underreporting may be due to availability of translation services, process of asking for translation, method of administration (if translated verbally), and how the screening tool translates linguistically and culturally. Our findings are similar to a previous pilot study integrating SDoH screening and navigation in pediatric primary care for immigrant families that reported less engagement and follow-up among patients with limited English proficiency. 21
Limitations
This evaluation was conducted in a single pediatric clinic in a health system and not necessarily generalizable to the entirety of the health system, other clinics, or populations. A key limitation was the reliance on documentation in the EHR for each step of the evaluation; it is possible that some processes were completed without documentation. The discrepancy between those who reported a need and were provided resource information (79.2% of those with a need) may be due to a few reasons including delays in reviewing screen information until after the visit, AVS documentation occurring at a family level when multiple children were brought for visits, or provision of resources through verbal or alternative means (e.g. organization business cards), and/or removal of resources from the AVS after discussion during the visit. Those that were missed due to delay in review were subsequently contacted by care navigators, however there may also have been omissions in documenting subsequent contacts. The process of offering resources and care navigation services was tracked in accordance with the AHC model, which didn’t require reporting on the success of resources connections and navigation. This limited our ability to evaluate the model as a closed loop and it is unclear if resources or services were accepted, utilized, or effective in addressing needs.
Lessons Learned
Our experience highlights opportunities for improvement and expansion of HRSN screening in pediatric care. Following the AHC model, we required 2 or more ED visits in the previous year to qualify for navigation. However the discordance observed between identified needs and ED usage (younger children had higher ED visits yet identified fewer needs and Hispanic/Spanish speaking children identified higher needs and fewer ED visits) suggests that navigation services should be offered more broadly. A large, randomized trial demonstrated care navigation produced more favorable resolution of social needs and child health at 4 months following screening compared to those provided written resources. 22 Because of an intimate understanding of community resources and ability to develop rapport with families, navigators can tailor both the content and delivery of information to family preferences. 23 Since these positions are often non-revenue generating, it is essential that policy makers consider their important impact on the health and SDoH of communities for sustainability.
Since NENS speakers were less likely to be screened or report a need, further examination is needed to better understand how diverse communities perceive HRSN screening and comprehend the relevance to health and healthcare. Screening tools need to be trans-created with and for populations served so that they are culturally and linguistically appropriate. 24 This will allow families to better understand the why behind these sensitive questions and enable them to feel safe and understand the utility in completing the screen.24,25
Finally, although we had experienced navigators we were unable to reliably evaluate resource connections. Identification of needs and provision of resource information do not guarantee connection to resources or mitigation of needs. To effectively determine success of resource connections, it is critical to cultivate relationships with community organizations to develop systems for referrals and data sharing.
A critical understanding of process and outcomes at DH Westside has informed the larger organizational implementation of HRSN screening and provision of resource information in pediatric care and for adults with high healthcare needs. Next steps involve partnering with patients and families to help ensure that further expansion is truly patient centered and culturally sensitive, avoiding stigma and ensuring privacy. Further understanding of existing health disparities will help inform prioritization for screening and expanding relationships with community partners. Future study will aim to establish the role of HRSN identification and connection to community resources and impact on clinical health outcomes.
Footnotes
Acknowledgements
We would like to extend our appreciation to the excellent staff at DH Westside Pediatrics Clinic for supporting the integration of HRSN screening and resource provision into our standard clinical workflow, and to our wonderful patients for sharing their information so that we can continue to improve our work to provide high-quality, comprehensive, patient-centered care.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Thomas Gray, Laura Podewils, Rasulo Rasulo, Randie Weiss, and Margaret Tomcho are current employees of Denver Health and Hospital Authority. The authors have no other relevant conflicts of interest to disclose.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The project described was supported by Funding Opportunity Number CMS-1P1-17-011 from the U.S. Department of Health and Human Services, Centers for Medicare and Medicaid Services. The contents provided are solely the responsibility of the authors and do not necessarily represent the official views of HHS or any of its agencies.