
Abstract
Introduction/Objectives:
Safe fish consumption is important for people who are or could become pregnant. A health system in Minnesota partnered with the Minnesota Department of Health to develop and disseminate messages to promote safe fish consumption for this population via the ChooseYourFish initiative. The ChooseYourFish message was delivered through 5 channels: the Healthy Pregnancy Program (HPP) with phone-based coaching, a clinic brochure, in the clinic after visit summary (AVS), direct mailing of the brochure with a letter, and in images on clinic waiting room monitors.
Methods:
We designed a pragmatic evaluation to understand the likelihood that each channel would result in awareness of the message and increase a recipient’s intent to act on the information. We surveyed 1050 women aged 18 to 40 in March-May 2020. Results are reported with descriptive statistics.
Results:
The survey was completed by 524 respondents (51%). Respondents receiving the ChooseYourFish message through any channel except clinic monitors reported a higher awareness of recommendations about eating fish (42%-56%) than respondents in the no-message comparison group (21%). The after visit summary and Healthy Pregnancy Program channels had more confidence in following recommendations (50%-54%) and showed more intention to eat fish (61%-62%) compared to lower-intensity channels (24%-31% and 19%-32%, respectively).
Conclusions:
Messages delivered by an often-trusted source (eg, healthcare provider) were more likely to increase confidence and intent. Despite the trend toward online health information, physical brochures still have large reach. Repetition of exposure may be important. Because all communication channels have advantages and drawbacks, using multiple delivery channels is appropriate in communication campaigns.
Introduction
Although fish contains eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA), essential nutrients for fetal visual and cognitive development, 1 fish may also contain mercury, a neurotoxin. 2 Because mercury levels vary by species, size, and source, 3 selecting fish that is low in mercury (hereafter referred to as “safe fish”) is challenging. This leads many who are or could become pregnant to simply avoid eating fish. 4 Because patients tend to trust health and nutrition information that they receive from their care providers, 5 health care systems are well-positioned to promote fish consumption and help individuals select fish that are safe to eat.
Source, style, format, accessibility, and repetition of health information influence how and whether messages are received.6,7 Even well-crafted messages are useless if the intended audience does not notice and respond to them. 8 Exposure to public health messages is a “central issue” in designing public programs. 6 Therefore, it is wise to evaluate health promotion campaigns with feedback from the intended recipients to assure that the messages are accessible, salient, relevant, and actionable. 9
To promote eating safe fish, a consumer-governed, integrated health system in Minnesota that serves 2 million patients and members nationwide partnered with the Minnesota Department of Health to develop messages for the organization’s patients and members, and the community at large, who are or could become pregnant. This initiative, ChooseYourFish, features a brochure and a mobile-responsive website. 10 The brochure contains information about the mercury content of various fish species and consumption guidelines for people who are or could become pregnant. It also answers common questions and contains a recipe and the website address (www.chooseyourfish.org). The website provides additional recipes, a fish flavor and texture guide, videos, and an interactive shopping list.
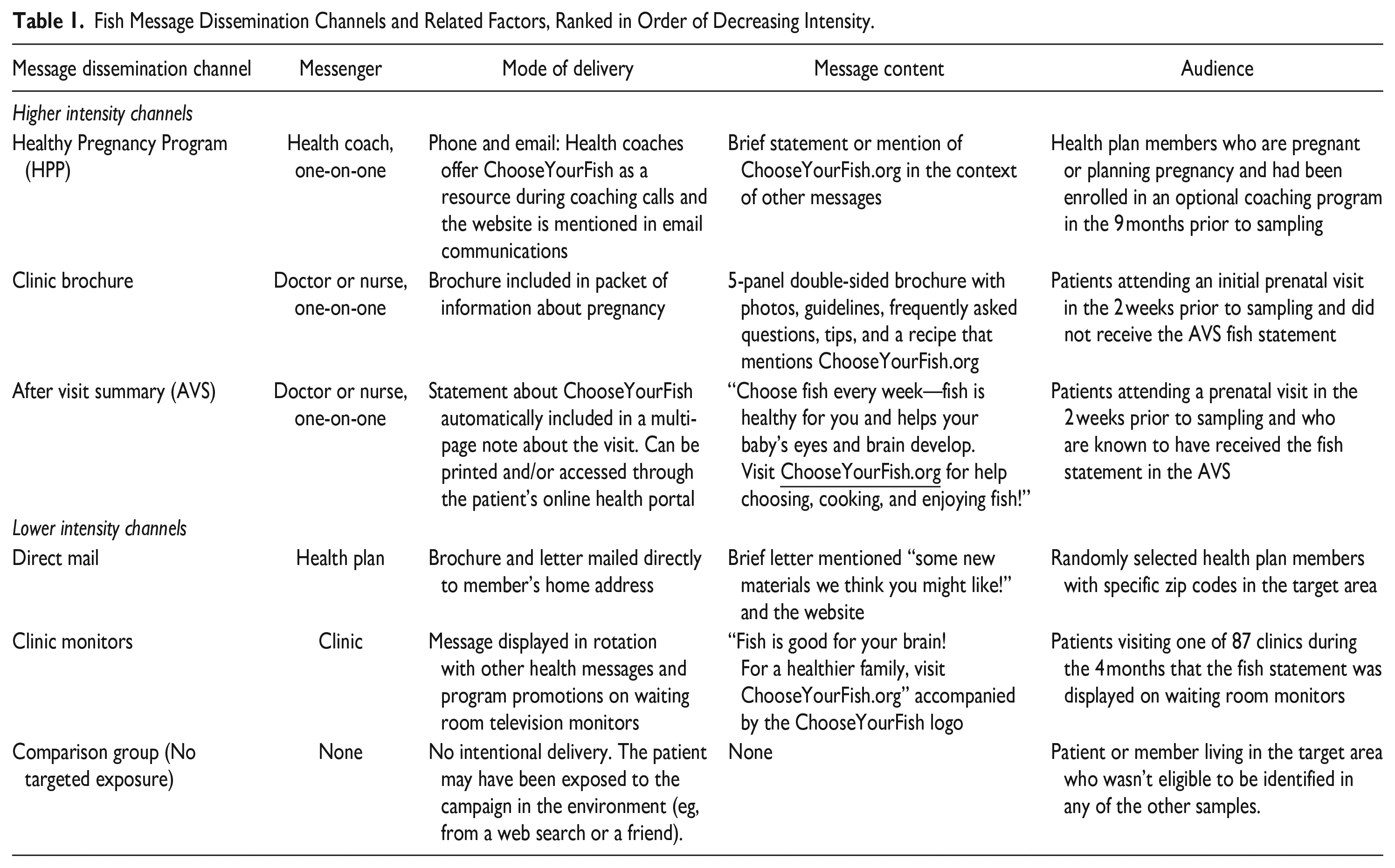
ChooseYourFish information is disseminated through 5 main channels: the Healthy Pregnancy Program (HPP) with phone-based coaching for insurance members; a brochure distributed in an information packet during a prenatal clinic visit; an after visit summary (AVS) shared at the conclusion of a clinic visit; by direct mail; and on clinic waiting room monitors (Table 1). Each channel varies across factors relevant in communication literature including messenger, mode, and message content. 6 Dissemination channels were ranked by intensity based on these factors and are listed in Table 1 from highest to lowest intensity. Higher-intensity strategies were delivered in a one-on-one setting by a healthcare provider, compared to lower-intensity strategies which were not.
Fish Message Dissemination Channels and Related Factors, Ranked in Order of Decreasing Intensity.
To understand the success of each dissemination channel, we conducted a pragmatic evaluation. 11 This manuscript summarizes the findings, revealing which channels were most successful in reaching people with the message, promoting fish recommendation awareness, and generating intent to change behavior.
Methods
Due to the need to hear directly from our target audience, a cross-sectional survey was used. For this pragmatic evaluation, individuals were not purposely selected to receive the message through a single specific channel, but rather, in most cases, were categorized according to the channel by which they would have organically encountered the information. The exception to this is the direct mail channel, in which individuals were purposely, yet still randomly, selected to receive a mailing with the materials. Surveys were fielded in March-May 2020, coincidentally at the onset of the COVID-19 pandemic, though exposure to campaign materials was before pandemic onset. The project was reviewed by the health system’s institutional review board and determined not to be human subjects research, thus exempt from oversight (determination date: 11/26/2018). Though formal consent was not required due to the IRB determination of non-human subjects research, the survey was clearly described as being voluntary and used informed consent language best practices.
Setting
This cross-sectional survey-based evaluation took place in a large consumer-governed integrated health system that provides clinical care and health insurance primarily in Minnesota and Wisconsin. It has over 90 clinics and hospitals serving 1.2 million patients, insures 1.8 million members, and has over 26,000 employees.
Sample
Health insurance plan enrollment data and electronic health records were used to randomly select 18 to 40 year old women who had been exposed to the ChooseYourFish message through 1 of the 5 delivery channels described above. A sixth group meeting age and gender inclusion criteria, but not purposely targeted with the ChooseYourFish message, was sampled as a no-intervention comparison group. To avoid overlap, the samples were drawn in the following order: HPP, direct mailing, clinic brochure, AVS, clinic monitors, and comparison group. In this analysis, providing the information through a healthy pregnancy coach, in a brochure given out by the clinic in an information packet, or on the AVS are referred to as higher intensity channels; the direct mail and clinic waiting room monitors are lower-intensity channels.
To achieve a 5% margin of error for point estimates, it was estimated that 50 completed surveys per channel would be required. Because a 35% response rate was expected, 1050 women (150 per channel) were sampled. Contamination, defined as self-reported message receipt via an unintended channel, is reported using responses from the second survey question.
Measures
A 9-question survey that required 5 min to complete (appended) was designed with questions assessing whether and where the respondent received the ChooseYourFish message; whether they were aware of fish consumption recommendations; their confidence in following consumption recommendations; their intention to eat fish if pregnant or planning pregnancy; their awareness of the ChooseYourFish campaign; and their demographic information. Because no established scales existed to meet our needs, questions were written using best practices in question writing, question and response option alignment, response option sets, and the use of plain language.12-14 A senior physician reviewed the initial draft for content alignment. The survey was then revised and shared with a stakeholder panel comprising healthcare providers, survey methodologists, behavior change experts, public health professionals, and fish consumption experts. These individuals reviewed the survey and gave feedback, either in a meeting or through email, on content, format, face validity, and ease of completion. The survey was again revised and approved by the same stakeholders. Finally, the survey was pre-tested on a sample of individuals similar to the subjects who would be receiving the survey.
The first 2 survey questions asked whether the individual had recently received information about eating fish (yes or no), and where the individual had received the fish information, with check all that apply response options including all dissemination channels. The 4 key outcome questions included: whether the individual knew about fish consumption recommendations (yes definitely, yes somewhat, or no); whether the individual was confident in following the fish recommendations (very confident, somewhat confident, or not at all confident); whether the individual would eat fish if they were pregnant or planning to be pregnant (yes definitely, maybe, or no); and whether the individual was aware of the ChooseYourFish campaign (yes or no).
A paper survey was mailed to all sampled individuals along with a $2 bill and a letter signed by the project lead and a physician (TEK). The letter described the survey, asked them to complete and return it, stated that participation was voluntary, and offered the option to decline the entire survey or leave individual questions blank. If, after 3 weeks, an individual either did not return a completed survey or indicate their intent not to complete one, interviewers from the organization’s survey research center made up to 5 attempts to contact the individual to complete the survey by phone.
Analysis
The results are described as means, standard deviations, frequencies, and percentages as appropriate. Responses to the 4 key outcome questions were dichotomized as the top response versus all others. To test the relationship between delivery channel and fish guideline awareness, pairwise differences in proportions were conducted and absolute risk differences with confidence intervals are presented. The pairwise differences in proportions were estimated using generalized linear models with a binomial distribution and identity link function. Statistical significance was defined as a P-value < .05.
Results
Respondent Characteristics
There were 524 individuals (51%) who completed the survey (AAPOR minimum response rate 1 15 ). The largest portion of respondents was from the comparison subsample (24.2%), and the smallest portion was from the direct mailing subsample (11.5%). On average, the respondents were 30 years old. The majority identified as non-Hispanic and white and were covered by commercial insurance. About 20% of the respondents were only members of the health plan and did not receive clinical care from the health system. The number of respondents who were patients but not covered by the health system’s insurance and the number of respondents who were patients and covered by the health system’s insurance (patient-members) were approximately equal (Table 2).
Descriptive Characteristics and Key Survey Question Responses from Women Responding to the ChooseYourFish Survey, N = 524. a

N for individual items may vary due to item nonresponse.
Survey Responses
Over 1/3 of survey respondents reported they were “definitely aware” of fish consumption recommendations. Almost half of respondents who reported being at least somewhat aware of recommendations also reported confidence in following them. A somewhat smaller proportion of respondents indicated that they intended to eat fish if they became pregnant (41.2%). Only 9% of respondents reported that they were aware of ChooseYourFish.
Receipt of the ChooseYourFish Message
Only a few respondents (6%) who had participated in the HPP reported receiving fish information from a coach. Nearly all respondents (87%) in the clinic brochure sample reported receiving information from this channel. However, 26% of the clinic brochure sample also reported receiving fish information in an AVS and 2% reported receiving information in the mail. Among those who should have gotten fish information in the AVS, 40% reported receiving it there; most of these patients (84%) also reported receiving a brochure from a doctor or in a clinic waiting room, but a few (2%) reported receiving a brochure in the mail. In the direct mailing sample, 65% reported receiving information in the mail, and a few (13%) reported receiving information from a doctor or nurse. No one in the clinic monitor sample reported receiving fish information from clinic monitors. Among the comparison group, 50% reported that they had recently seen, heard, or been given information from some source about eating fish.
Guideline Awareness
Awareness of recommendations about which fish to eat for health benefits while avoiding harmful chemicals is in the expected order: higher channel intensity was associated with greater awareness (Figure 1). Being given the ChooseYourFish message by any method other than clinic monitor resulted in higher awareness that recommendations exist (42-56%, P ≤ .004) than not being given the message by any channel. Those who received the message via HPP (56%, P < .001) and clinic brochure (50%, P = .016) also had higher awareness than those who received the message via clinic monitors (32%). There were no other statistically significant differences between intended delivery modes.

Relationships between Intended Dissemination Channel and ChooseYourFish Outcomes.
Confidence
The response pattern for confidence in following the recommendations differed from those for awareness of the recommendations. Most higher-intensity channels (AVS and HPP) had more confidence in following recommendations (50%-54%) compared to less intensive channels (24%-31%). There were no differences in confidence between lower-intensity channels.
Intention to Eat Fish
The patterns associated with intention to eat fish if pregnant or planning pregnancy were similar to the patterns associated with confidence to follow recommendations. Higher intensity channels (HPP and AVS) showed more intention to eat fish (61%-62%), while lower intensity channels (ie, direct mailing, clinic monitors, and comparison samples) showed significantly less intention (19%-32%). There were not significant differences within the higher or lower intensity channels.
ChooseYourFish Awareness
The AVS had the highest campaign awareness (25%). HPP, direct mailing, clinic monitor, and comparison samples all had significantly lower program awareness (8.3%-1.6%). Program awareness in the clinic brochure sample (14%) was significantly higher than those in the clinic monitor and online ad samples (1.6%-2.4%), but not significantly different from other samples.
Discussion
In this evaluation to increase awareness of recommendations to eat safe fish and increase intentions to follow the recommendations while pregnant, individuals who received the ChooseYourFish message via the clinic brochure sample had highest intended message receipt, followed by direct mailing, AVS, HPP, and finally clinic monitors. Interestingly, our 2 most-received channels involved brochures. Despite the push to move health information online for ease of access, our findings suggest that brochures delivered to the intended audience may still be the best way to reach individuals. This aligns with literature showing that educational brochures are the preferred method of pregnant people for receiving health information from providers.16,17 However, effective health communication must go beyond basic message receipt; individuals need to understand the information and act on it. While there is some indication that brochures may be effective in increasing health behavior knowledge among pregnant people, 18 others have found that brochures alone may not be enough, 19 leading authors of a systematic review to recommend written information in combination with verbal information for patients, albeit in a different setting than pregnancy.18,20
Going beyond message receipt to knowledge and intent, all forms of communication, except for clinic waiting room monitors, increased awareness of fish consumption recommendations. However, respondents who had been exposed to a high intensity channel were significantly more likely to report confidence in being able to follow the recommendations and intention to eat fish while pregnant. Consistent with literature, this suggests that directly-delivered messaging approaches paired with an opportunity for tailored discussion are more likely to increase knowledge and intent compared to those where the message is not directly delivered.21,22 Increased intent could stem from trust in the provider’s recommendations,17,23 the setting in which the information was received, 23 and/or topic salience, among other factors.
Among all 3 of our high-intent groups, the individuals were pregnant or planning pregnancy and were actively seeking care by signing up for a coaching program or by attending a clinic visit. In all of these cases, the messenger combined with topic salience may have led more of these individuals to be receptive of this information. This aligns with literature showing that pregnant people trust healthcare providers for information and are more likely to change behavior when urged to do so by a provider.24,25
Repetition may also contribute to these modes’ success. All 3 highest-intent groups may have received the message from multiple sources. Literature from smoking cessation shows that repeated messages in different modalities delivered by different messengers are associated with higher intervention success. 26 Fjeldsoe et al also show that more intervention strategies result in better maintenance of behavior change. 7 Rather than focusing on the single best dissemination strategy, future health dissemination approaches should focus on breadth rather than depth.
This pragmatic evaluation produced actionable project-specific results. Learnings were applied back to the program to inform future dissemination strategies. The mixed-mode survey approach resulted in a moderately high response rate, but mode differences may complicate the ability to draw conclusions given the survey topic of messaging channel. Other limitations include potential messaging overlap, though we pulled each sample to be mutually exclusive. We could not control for selection into dissemination channel, so it is possible that individuals in one group are different from another. The high level of message exposure among the control group was surprising but promising for our initiative overall. The sample was from a single, regional health plan and care group. We measured intent to change behavior rather than actual behavior change. Due to survey design, we could not isolate the factors that led to reach, guideline awareness, or behavior change outcomes. Finally, it is possible that the COVID-19 pandemic had some effect on our survey response, though all samples and message exposure should have happened before the pandemic hit Minnesota.
Conclusions
Message delivery through low impact channels (eg, direct mail and clinic waiting room monitors) can increase patient awareness of a recommendation. However, higher-intensity channels that deliver health messages directly from a credible source are more effective at increasing confidence in following recommendations and intent to eat fish during pregnancy. Altogether, it may be best to deliver messages via many channels to increase likelihood that an individual receives the message at least once, if not more.
Supplemental Material
sj-pdf-1-jpc-10.1177_21501319231169998 – Supplemental material for Survey-based Evaluation of a Fish Consumption Information Dissemination Campaign Within an Integrated Health System: Learnings From ChooseYourFish
Supplemental material, sj-pdf-1-jpc-10.1177_21501319231169998 for Survey-based Evaluation of a Fish Consumption Information Dissemination Campaign Within an Integrated Health System: Learnings From ChooseYourFish by Jennifer M. Dinh, Meghan M. JaKa, Thomas E. Kottke, Jacob Haapala, Rachael Rivard, Abigail S. Katz, Patricia McCann and Jeanette Y. Ziegenfuss in Journal of Primary Care & Community Health
Footnotes
Author Contributions
Jennifer Dinh: Conceptualization, Methodology, Investigation, Writing—Original Draft; Meghan JaKa: Conceptualization, Writing – Original Draft, Visualization; Thomas Kottke: Conceptualization, Writing—Review & Editing, Supervision, Funding acquisition; Jacob Haapala: Methodology, Software, Data Curation, Formal analysis, Writing—Review & Editing; Rachael Rivard: Methodology; Software, Resources, Writing—Review & Editing; Abigail Katz: Conceptualization, Writing—Review & Editing, Supervision; Patricia McCann: Conceptualization, Writing—Review & Editing, Project administration, Funding acquisition; Jeanette Ziegenfuss: Conceptualization, Methodology, Writing—Review & Editing, Supervision, Project Administration
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Environmental Protection Agency’s Great Lakes Restoration Initiative through the Minnesota Department of Health [grant number GL00E01161].
Ethical Approval
The project was reviewed by the health system’s institutional review board and determined not to be human subjects research, thus exempt from oversight (11/26/2018, #A15-174).
Consent to Participate
Not required.
Clinical Trial Registration
Not applicable.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.