
Abstract
Symptoms of anxiety and depressive disorders have been increasing substantially among adults in the United States (US) during the COVID-19 pandemic, particularly for low-income populations. Under-resourced communities have difficulties accessing optimal treatment for anxiety and depression due to costs as well as the result of limited access to health care providers. Telehealth has been growing as a digital strategy to treat anxiety and depression across the country but it is unclear how best to implement telehealth interventions to serve low-income populations. A narrative review was conducted to evaluate the role of telehealth in addressing anxiety and depression in low-income groups in the US. A PubMed database search identified a total of 14 studies published from 2012 to 2022 on telehealth interventions that focused on strengthening access to therapy, coordination of care, and medication and treatment adherence. Our findings suggest that telehealth increases patient engagement through virtual therapy and the use of primarily telephone communication to treat and monitor anxiety and depression. Telehealth seems to be a promising approach to improving anxiety and depressive symptoms but socioeconomic and technological barriers to accessing mental health services are substantial for low-income US populations.
Introduction
The use of telehealth to deliver mental health services has become increasingly popular in light of the coronavirus (COVID-19) pandemic. Telehealth involves the use of telecommunications and information technology to provide access to consultation, intervention, and exchange of digital information. 1 Digital communication includes audio and video conferencing equipment. The telehealth care delivery process, particularly in a mental health setting, typically connects a patient or client with a physically distant licensed mental health provider such as a psychiatrist, psychologist, therapist, or clinical social worker. In this context, telehealth has the potential to significantly improve access to mental health treatment by overcoming barriers such as transportation costs to clinical visits. 2
Mental health care poses a unique challenge to low-income groups, with chronic stressors linked to socioeconomic challenges. Limited access to providers, poverty, exposure to crime, and poor housing conditions are common upstream factors that impact the risk for anxiety and depression.3-5 Barriers to mental health care access perpetuate the risk of common mental health conditions such as depression and anxiety, which are associated with low-income status.3-5
Existing literature on anxiety and depression has highlighted a relatively high prevalence of depression among low-income groups.6-8 Several mechanisms have been suggested to understand this phenomenon; for example, financial insecurity and negative emotions associated with economic status contribute to social isolation and the risk for depressive symptoms.5,9,10 Moreover, suicide is a pressing public health concern and one of the leading causes of death in the United States. 11 Prevention efforts have identified key risk factors to predict suicide; depression and anxiety are the most commonly cited risk factors associated with suicide. 12
This review assesses the value of telehealth as an evidence-based intervention to deliver mental health services in low-income populations. Telehealth is rapidly evolving and growing, and the demand for mental health services is increasing in light of the COVID-19 pandemic. As such, this review aims to report and summarize the evidence in the scientific literature on the use of telehealth to address anxiety and depression in low-income groups. The study also provides some insights on the expected outcomes and benefits of mental health care delivered through telehealth while considering the current state of the mental health care delivery infrastructure in the United States (US).
Materials and Methods
A PubMed database search was conducted to identify scientific articles published from 2012 to 2022 addressing the use of telehealth for the delivery of health care services related to depression and anxiety in low-income populations. A cut-off date of 2012 was used for this review to consider changes to health care delivery and insurance enrollment for low-income populations after the Affordable Care Act (ACA) was enacted in 2010. 13 The PubMed database was selected as the most appropriate search engine to identify telehealth studies in health science, social science, and information systems research. Although some telehealth studies are included in engineering and technology databases, we focused only on articles abstracted in PubMed because we were interested in the use of telehealth to provide health care services for a specific vulnerable population rather than the technology-oriented aspects of telehealth (eg, bandwidth, reach, technical specifications).
Selected articles were included based on title and abstract only. Articles were considered for inclusion if they focused on a telehealth intervention to address anxiety and/or depression among low-income populations in the US. Studies using the terms telemedicine and telepsychiatry were also included in the PubMed search. For the purposes of this study, telehealth interventions were defined as those providing virtual mental health services. Low-income populations were defined based on income. Articles were excluded if they were systematic reviews, did not focus on telehealth services for anxiety and/or depression for low-income individuals, were not written in English, and were not conducted in the US.
Figure 1 summarizes the narrative review study selection process. Boolean operators (AND, OR, and NOT) were used to combine the following keywords: “tele,” “low-income,” “depression,” and “anxiety.” The search results retrieved 87 articles using the above-mentioned keywords. Duplicates were removed, resulting in 21 articles. The remaining 21 articles were assessed against the inclusion and exclusion criteria, which resulted in the removal of 7 articles; hence, 14 articles were included in this narrative review (Figure 1). Articles included randomized controlled trials (RCTs), quasi-experimental studies, observational studies, and qualitative studies.

Flowchart of studies included in narrative review.
The study design, data sample, and summary of telemedicine services were captured as part of the data extraction process. The selected articles were then reviewed in detail, and relevant data were synthesized based on their relevance to the utilization of telemedicine for anxiety and depression in low-income populations. Study findings from the narrative review were used to assess the value of telehealth in treating anxiety and depression, patterns in telehealth use, and implications for future interventions to address current gaps in digital health care for low-income populations residing in the US.
Results
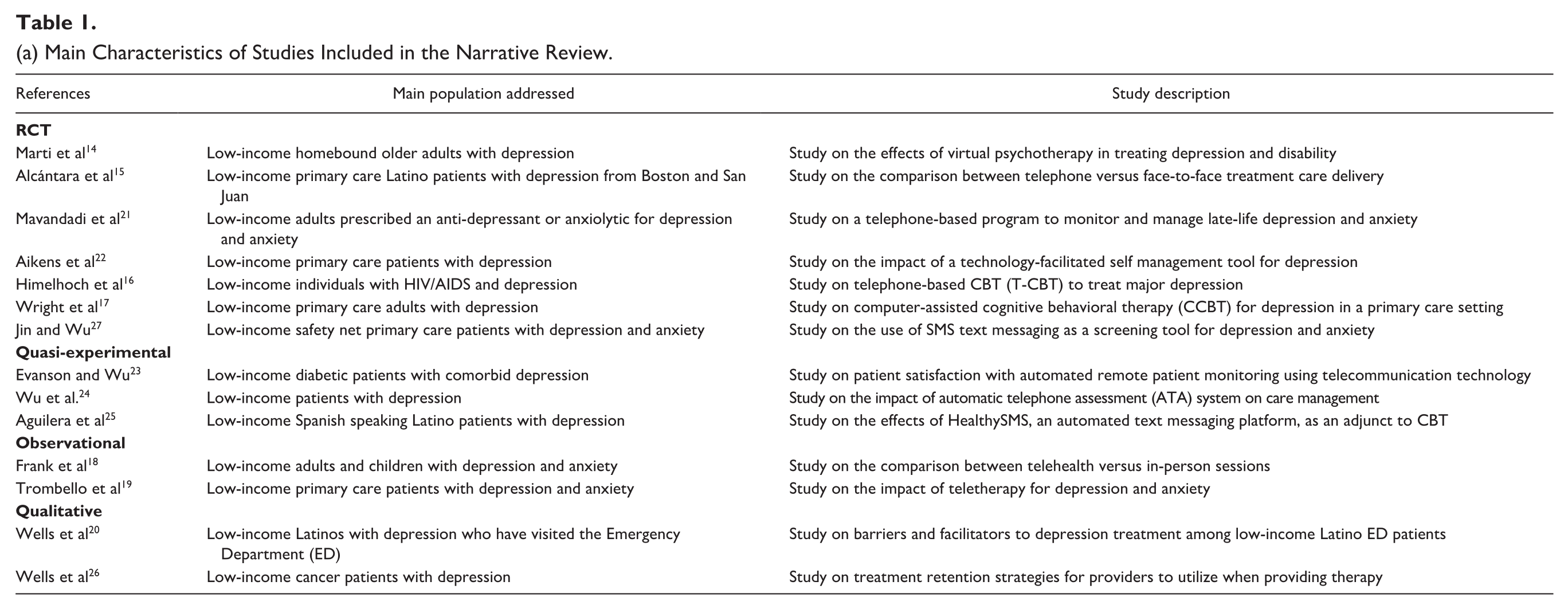
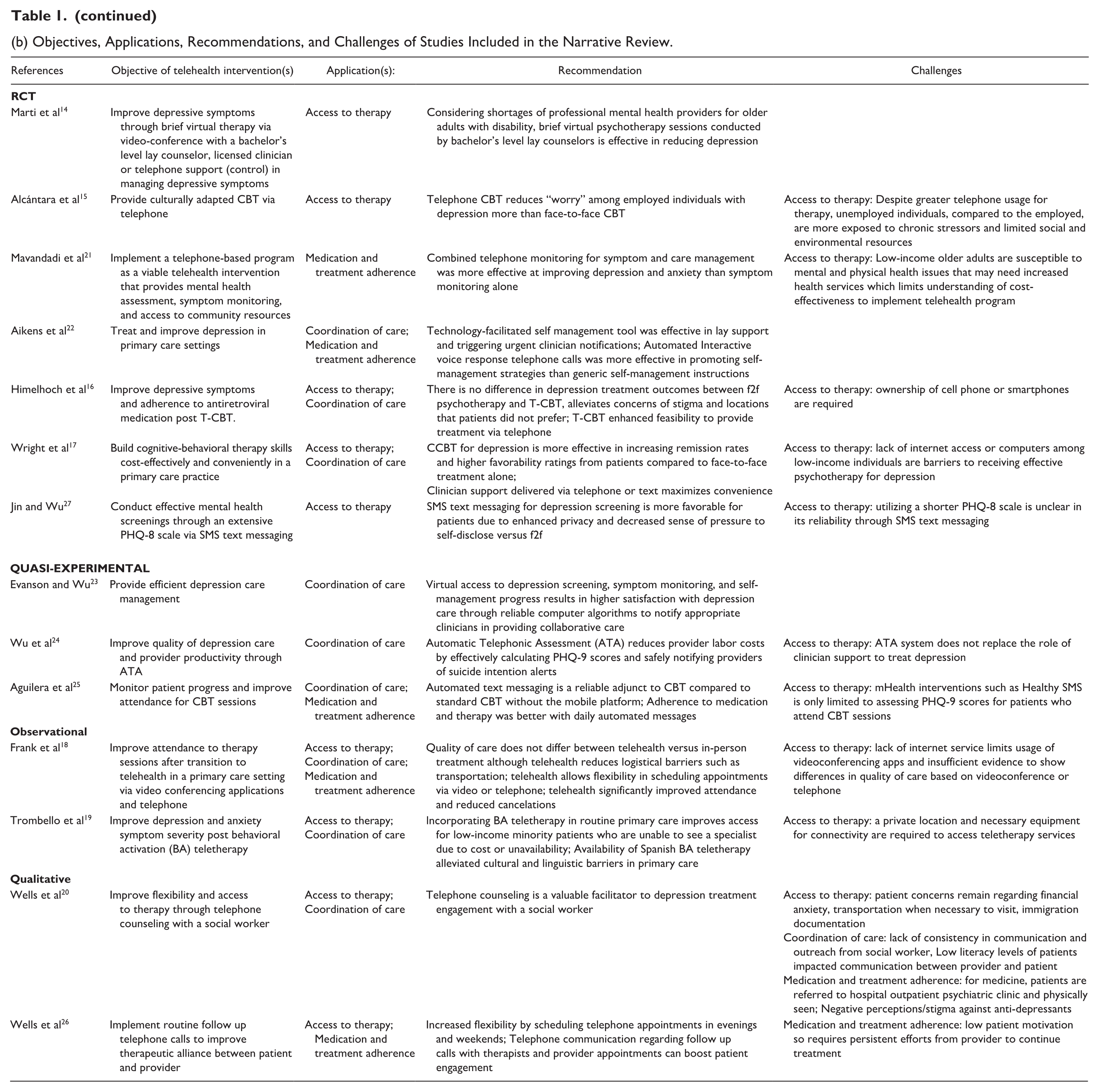
Table 1(a) reports the main characteristics of the studies that were included in the narrative review. Areas evaluated for each study included its research design, population served, and study description. Seven of the articles reviewed utilized an RCT design while the remaining articles included 3 quasi-experimental studies, 2 observational studies, and 2 qualitative studies. Table 1(b) reports the telehealth intervention objectives, its applications, recommendations, and challenges. Through a narrative synthesis approach, summarized in Table 1(b), findings converged into 3 main applications for telehealth interventions: (1) access to therapy, (2) coordination of care, and (3) medication and treatment adherence. Access to therapy and coordination of care were the main applications described in the articles, with 9 out of 14 articles (64.3%) reporting the use of telehealth for therapy access and care coordination. Medication and treatment adherence were the focus of 5 out of 14 articles (35.7%). There was a broad consensus on how being of low-income status is associated with access barriers to optimal mental health care services. While all reviewed studies converged on the need to implement a digital strategy to provide mental health care services for persons with anxiety or depression symptoms, there were differing approaches to applying specific telehealth interventions to improve mental health care delivery.
(a) Main Characteristics of Studies Included in the Narrative Review.
(b) Objectives, Applications, Recommendations, and Challenges of Studies Included in the Narrative Review.
The articles, dated from 2012 to 2022, discussed telehealth interventions based across various regions of the US, and all of them focused on low-income individuals with either anxiety or depression symptoms as the target population for the study. All the articles identified examined telehealth interventions to address depression, and 4 articles examined telehealth and both anxiety and depression. None of the studies solely examined anxiety. All articles utilized at least 1 telehealth intervention to treat depression or anxiety but were carried out in various health care settings such as primary care clinics, safety net health facilities, and emergency departments. Mental health professionals that were referenced throughout the articles included psychiatrists, lay counselors, licensed clinicians, coordinating staff members, and social workers.
Virtual therapy was the most commonly used telehealth intervention,14-20 and it included psychotherapy, cognitive behavioral therapy (CBT), and post behavioral activation (BA) therapy. The second most referenced telehealth intervention was virtual patient monitoring and self-management tools.21-26 Self-management tools included a self-reported questionnaire form to monitor changes in symptoms, medication intake, contact information for professional help, and reviewing provider messages for patient empowerment. These approaches were also used through telephone monitoring via call, text, or both. Automated telecommunication technology was also referenced as a service to improve the ability of providers to monitor symptoms of anxiety and depression,23,24 in addition to self-care strategies related to promoting healthy behaviors affecting mood.22,25 Only one study focused mainly on virtual mental health screenings for anxiety and depression. 27 Mental health screenings were primarily conducted using the Patient Health Questionnaire-2 (PHQ-2) and PHQ-9 scales, which are self-reported, evidence-based tools widely used for depression screening, assessment, and monitoring.28,29
Virtual therapy was an alternative solution to face-to-face therapy to improve access to mental health care among low-income groups. Computer-assisted CBT (CCBT) was a common intervention, particularly in a primary care setting that targeted low-income individuals who could not see a specialist due to cost, health insurance coverage status, and unavailability due to geographic location. 17 The primary care setting represented a commonality for low-income individuals to participate in either telephone CBT (T-CBT) or CCBT.15-17
One major barrier to accessing therapy was the shortage of mental health providers. To alleviate this barrier, virtual therapy was provided by social workers or lay counselors.14,20 Traditional mental health providers were psychiatrists and licensed clinicians for conducting virtual therapy through video or telephone. An emphasis on telephone interactions was noted in many of the studies. In particular, Short Message Service (SMS) text messaging 27 was encouraged to enhance privacy and alleviate the fear of self-disclosing uncomfortable information to a provider.
Coordination of care entailed facilitating treatment provision and receipt for the clinical and patient, respectively. In this context, reliable computer algorithms were crucial to facilitate technological tools to coordinate clinician-to-patient messages. Support and guidance were emphasized in symptom monitoring processes, including the use of automated technological assessment (ATA), which monitored suicidal ideation or significant changes in symptoms.22,24 The use of ATA maximized convenience and ultimately lowered the time of intervention for providers during emergency cases. Alongside ATA, T-CBT16,19 maximized convenience for low-income individuals with barriers such as transportation and internet issues. Coordination of care was also made possible by emphasizing the use of bilingual therapists who can provide therapy. 19 Bilingual therapists were useful in addressing gaps in health communication and tailoring culturally-competent care based on familiarity, language, and overall comfort.
Multitasking was a major aspect of coordination of care in mental health care delivery. Technology-facilitated tools encompassed depression screening, symptom monitoring, and self-management progress. All 3 aspects of coordination of mental health care reinforced the convenience of independently accessing services on 1 online site or mobile platform. 23 Although these initiatives increased a sense of convenience, this form of telehealth intervention was seen as a supplement to therapy and direct face-to-face treatment.
Mental health providers were susceptible to patient cancelations or treatment dropouts. To improve medication and treatment adherence, telehealth interventions catered to widening access to digital care by increasing availability to schedule appointments through video and telephone.18,20 Telehealth was shown to improve overall patient attendance at appointments and lower cancelation rates. It should be noted that the studies included did not compare the effectiveness of video versus telephone for mental health services. Increasing availability for appointments in the evenings and weekends boosted patient engagement and increased telephone communication. One study specifically explored improved attendance for CBT after implementing daily automated messages using a mobile platform. 25
Telehealth was intended to improve access to mental health services by deferring in-person visits due to access barriers for low-income populations. Despite that, several challenges were noted in many of the included studies. The biggest challenge to telehealth continued to be access to therapy due to barriers of being low income.15-17,21 There were differences in employed versus unemployed individuals concerning exposure to chronic stressors and limited resources despite increased access to telephone and virtual therapy. 15 Other challenges or barriers to accessing virtual mental health services included a lack of accommodation for mental and physical health issues or disability, which would require increased use of health care services. 21 Therefore, access barriers to telehealth also encompass challenges to being of low-income status such as affordability costs, insurance, and availability of technological services.
Ownership of technological devices such as a mobile phone or computer was required,16,17,19 and this was a significant barrier to internet access and, thus, effective therapy for depression and anxiety. Besides therapy, SMS text messaging brought concerns about the limited viability of utilizing a shorter PHQ-8 scale. 27 Furthermore, a study showed that mental health interventions using text messaging were only limited to patients who were already attending CBT sessions, but did not include patients who were not scheduled and were not attending sessions. 25 Individuals were living in an area with limited privacy and did not own necessary equipment for connectivity barriers.
When coordinating mental health care for patients and providers, patient outreach differed in the context of non-English speaking populations. Low English literacy impacted communication between the provider and patient, warranting attention to interpreter services. 26 Incorporating interpreter services that include providers who are Spanish-speaking, for instance, enhanced the telehealth experience by accommodating patients with language barriers. In addition, patients, at times, required a referral to the hospital outpatient psychiatric clinic, which invoked a sense of financial anxiety and potential negative stigma against antidepressants 20 —this ultimately lowered medication and treatment adherence in those cases.
Discussion
This review synthesized current literature on telehealth interventions to address mental health care barriers due to socioeconomic hardship. Findings from this review revealed commonalities in telehealth goals and differences in the types of interventions specific to various telehealth strategies. There were consistent positive findings across studies supporting the use of telehealth to provide mental health services, specifically for anxiety and depression. Studies reviewed showed minimal differences in the quality of care between virtual therapy and traditional in-person sessions. For low-income individuals, the availability of telephone usage with audio or video access compensates for technological challenges such as accessing the internet and limited bandwidth.
Although telehealth allows virtual access to a mental health provider, the findings from this review do not provide sufficient support to the idea of entirely replacing in-person mental health care with telehealth. Telehealth is limited in addressing persistent barriers to accessing care that continue to affect low-income populations such as affordability and stigma. However, telehealth can improve access to mental health care in low-income populations that are underserved due to limited resources. Telehealth interventions can assist in mitigating social determinants of health such as transportation challenges, and factors such as access to technology and other socioeconomic disadvantages. While this review did not specifically focus on the role of geographic region, more research is needed to assess the types of providers and clinics compatible for telehealth interventions in both rural and urban areas. Different low-income populations (eg, rural vs urban areas) may benefit more than others from telehealth interventions.
There are some limitations to this narrative review that should be noted. Although the Centers for Medicare & Medicaid Services (CMS) have expanded access to telehealth services due to the COVID-19 pandemic, issues with provider reimbursement persist in the mental health care system in the US. Reimbursement for telehealth use through Medicaid, specifically, could be considered for both video and audio mental health services. Telephone usage for telehealth interventions should be considered in policy changes to CMS and health insurance plans to increase participation in telehealth services. The studies included did not discuss the cost-effectiveness of implementing telehealth service services. Current data on the total cost of providing telehealth services is limited to fully understanding cost outcomes. Efforts to implement telehealth interventions could consider the availability of technological resources, the effectiveness of telephone versus video therapy to treat depression and anxiety, and the use of mental health screenings for low-income groups. Despite these limitations, this narrative review provides key insights into future research on telehealth for underserved communities.
In conclusion, telehealth has great potential to improve access to mental health services comparable to in-person care for underserved, low-income populations. Further research could focus on gaining clarity of differences in the quality of mental health care between video versus telephone. In addition, the level of financial resources needed for potential users of telehealth services should be considered when using this technology-based approach to provide mental health care services. Lastly, given the burden of unmet need among racially marginalized populations, incorporating culturally tailored services that include but are not limited to access to bilingual mental health providers should also be an important consideration for future telehealth implementation strategies.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: We thank the Program to Accelerate Training in Health Equity (PATHE) initiative at the School of Global Public Health, New York University, for its financial support.