
Abstract
Introduction/Objectives:
Despite the introduction of lung cancer screening using low dose computed tomography (LDCT), overall screening rates in the U.S. remain low, with certain populations including Black and rural communities experiencing additional disparities. The primary objective of this study was to understand the facilitators of lung cancer screening initiation and retention in Alabama reported by people at risk from mostly rural, mostly Black populations in Jefferson County—including the urban center of Birmingham—and 6 rural counties: Choctaw, Dallas, Greene, Hale, Marengo, and Sumter.
Methods:
We conducted semi-structured telephone interviews with 58 people who underwent lung cancer screening between December 2019 and January 2022. Participant responses were recorded by the interviewer for analysis. Open-ended responses were coded to identify emergent themes.
Results:
The most reported influences to initiate screening were information or suggestion from a Community Health Advisor (CHAs) or the supervising county coordinator, suggestion from a friend, or consideration of a personal history of smoking. Most participants reported multiple influences. Physicians were not very influential in decisions to initiate screening, but they were extremely influential in participants’ intent to continue screening, both positively and negatively. Knowing the recommended timeline for their annual scans was also a predictor of intention to continue screening. Participants screened during the COVID-19 state of emergency expressed less certainty about dates of next scans and more ambivalence about intention to continue screening.
Conclusions:
This study shows the benefit of using multiple methods to support increased awareness of and interest in lung cancer screening, particularly when educational messaging through CHAs is used. Clear guideline-based messages from healthcare providers about recommended screening is important for increasing retention. COVID-19 related implementation challenges impacted screening recruitment and retention. Future research is warranted to further explore use of CHAs in lung cancer screening.
Keywords
Introduction/Objectives
Approximately 236 740 people in the U.S. will be diagnosed, and 130 180 will die from lung cancer in 2022. 1 Lung cancer screening using low dose computed tomography (LDCT) provides an opportunity to increase survival, but uptake of the intervention has been slow. Between 1.0% and 16% of the eligible population in the U.S. has been screened, with rates varying based on state and geographic region.2-5 Additional disparities impact certain populations: Black individuals have been less likely to be screened compared to White patients and experience lower adherence to screening, increased delays in follow up, and more loss to follow up. 6 Tobacco marketing has targeted Black communities for decades, with product advertising more concentrated in these communities compared to White communities. 7 Rural populations also have more limited access to primary care providers and to lung cancer screening programs. 8 Lung cancer incidence, advanced disease, and mortality rates are higher in rural areas. 9
In Alabama, the need to address these disparities is high: Alabama has twice the Black population as the national average (26.8% vs 13.4%). 10 Black Alabamans between the ages of 19 and 64 are more likely to be uninsured than the White population (12% vs 8.8%). They are also more likely to be covered by Medicaid compared to the White population (31.5% vs 15%), and Alabama is 1 of 6 states to not cover lung cancer screening for Medicaid recipients, which impacts access.11,12 According to the American Lung Association (ALA), 20% of lung cancer cases were diagnosed early in the Black population in Alabama compared to 25% in the non-Hispanic White population, indicating the need for improved early detection. 13
To address these challenges, GO2 for Lung Cancer (GO2; formerly Lung Cancer Alliance) partnered with The Office of Community Outreach and Engagement at the O’Neal Comprehensive Cancer Center at the University of Alabama’s (UAB) on the Alabama Lung Cancer Awareness, Screening and Education (ALCASE) project. ALCASE paired the lung cancer screening expertise of GO2 with UAB’s Community Health Advisor (CHA) Model to decrease lung cancer disparities in several counties with medically underserved, primarily rural, and significant Black populations through education and awareness, while increasing capacity for and access to responsible screening. CHAs are trained leaders in their communities who provide cancer awareness and early detection messages and resources. UAB CHAs provided navigation and education to move participants to lung cancer screening, with referral to smoking cessation services as needed. The CHAs in this project—volunteers who received a small stipend—were supervised by paid UAB staff called County Coordinators. ALCASE focused on Jefferson County—including the urban center of Birmingham—and 6 rural counties: Choctaw, Dallas, Greene, Hale, Marengo, and Sumter. These counties are part of the “Black Belt” of the southern US, a region known for its history of cotton farming, plantations, and large enslaved populations. 14 Black individuals account for 43% to 80% of the target county populations. 10
The primary objective of this analysis was to understand the facilitators of lung cancer screening initiation and retention reported by patients from mostly rural, mostly Black communities in Alabama.
Methods
ALCASE ran from June 2018 through November 2021. The study was open to residents of any race or gender living in the target counties who met the eligibility criteria for lung cancer screening based on the U.S. Preventive Service Task Force (USPSTF) recommendation at the time of project initiation: 55 to 80 years of age, a 30 pack-year smoking history, and smoked at the time of their participation or had quit within the past 15 years. The USPSTF updated these guidelines in March 2021, broadening the recommendation to include younger individuals with a lower pack year smoking history, but for consistency, eligibility criteria were not changed. Potential screening patients interacted with CHAs and local county coordinators who provided information about screening and navigation to encourage uptake. Study participants provided county of residence, demographics, insurance information, and screening location preference using an intake form.
During the study, 65 people were screened for lung cancer and 58 (89%) completed semi-structured telephone interviews after screening between December 2019 and January 2022. The interview script was based on a previously used script that explored why eligible individuals opted out of lung cancer screening. 15 There are no known examples of Likert scale measures validated in a population with low literacy rates, so program staff developed response options in consultation with an experienced local community health advisor who understood the needs of the target population. The script was approved by the Institutional Review Board at UAB and can be found in Supplemental Materials. The program manager contacted participants to conduct the interview of up to 28 questions with a mix of open and closed-ended questions, entering responses into a database in real time. Participants were asked questions about the decision to be screened, screening experiences, feelings at various timepoints in the process, and intent to continue the screening process.
Results
There were 243 people determined eligible and who consented to be evaluated for study participation. They were engaged by county coordinators and CHAs at community events, in small groups, and individually to educate on lung cancer risk and screening eligibility, and 65 (27%) were subsequently screened for lung cancer. Of the participants who received lung cancer screening through the project, 58 of 65 (89%) participants participated in the interview, with 40% of respondents interviewed within 2 weeks of their scan. Participants were 58% male and 42% female. Individuals who identified as Black accounted for 95% of respondents. Medicare beneficiaries accounted for 53% of respondents. Other respondents received health coverage through Medicaid, VA, private insurance, or a combination of plans. Three respondents reported being uninsured. Full demographic information is listed in Table 1.
Baseline Characteristics.

Respondents were asked, “What made you think about being screened?” Multiple reasons were allowed (Table 2). Most respondents (69%) decided to get screened because a CHA or county coordinator suggested it. Overall, 65% of respondents cited at least 2 reasons for being screened. For those who only cited one influence, 53% indicated that the CHA or county coordinator was the sole influence, and 25% indicated that seeing an advertisement for screening was the sole influence. This refers to a general awareness mailer produced by UAB and sent to a large population in the target counties during October and November 2021. Of the 9 respondents who reported “seeing an advertisement” as a reason for being screened, only one indicated that the suggestion of a CHA or county coordinator was also an influence. This may indicate that educational mailers are an effective tool to reach those missed by CHA outreach. Notably, only 3% of respondents indicated that a doctor’s suggestion was a reason they got screened.
Reasons for Being Screened (Select All That Apply) (n = 58).

When asked if they intend to get screened every year, 51% said “Yes” (Table 3). Most were motivated by their doctor’s recommendation. Six respondents were motivated by concerns about their health or to make sure there are no changes over time. Three indicated that they would get a lung scan again if they can afford it or it is covered by their health plan. Two indicated that they are already scheduled for another scan because of significant findings during screening. Of the 25 respondents who said “Maybe” or “I don’t know,” 20 indicated that this decision was or will be influenced by their doctor or nurse.
Intention to Screen Annually (n = 57).

For respondents who intended to continue, most received clear guidance from their healthcare provider about the importance of continuing screening. They shared that, “My doctor said I need to follow up yearly, just in case something shows up” and “The NP at the hospital said she wants to keep a check on it to see if anything changes.” This is consistent with the current clinical guidelines for screening, which recommend annual screening while a person meets criteria for age and smoking history. 16
Ambivalent respondents (“Maybe” and “I don’t know”) also illustrated the influence of provider messaging, however not always in a positive way. Reasons for ambivalence included, “My doctor said my scan didn’t show anything,” “My doctor said I didn’t need any follow up,” and “It will be every 2 years per my primary care doctor.” The interval suggestion of “every 2 years” came up several times for respondents who were unsure or not planning to continue screening. All 4 respondents who said “No” when asked if they will get a scan every year said they would consider screening if their doctor recommended it or that they were told that they do not need to be screened again or only every other year.
When asked “Do you know when your next scan appointment is?” 27 respondents said “Yes” and 30 said “No.” Respondents who knew the date or timeline for their next scan or that their care provider would call them to schedule it were more likely to indicate their intent to continue with screening compared to respondents who did not know when their next scan would be.
Respondents who did not know the timeline for their next scan were not asked follow-up questions, however 2 added that their doctor told them there was no follow up recommended. For those who did not know the timeline for their next scan, only 13% indicated intent to continue screening and 55% said they were not sure (“I don’t know” or “Maybe”). In contrast, for those who knew the timeline for their next scan, 93% said they intended to continue screening and only 7% said they were uncertain (Figure 1).
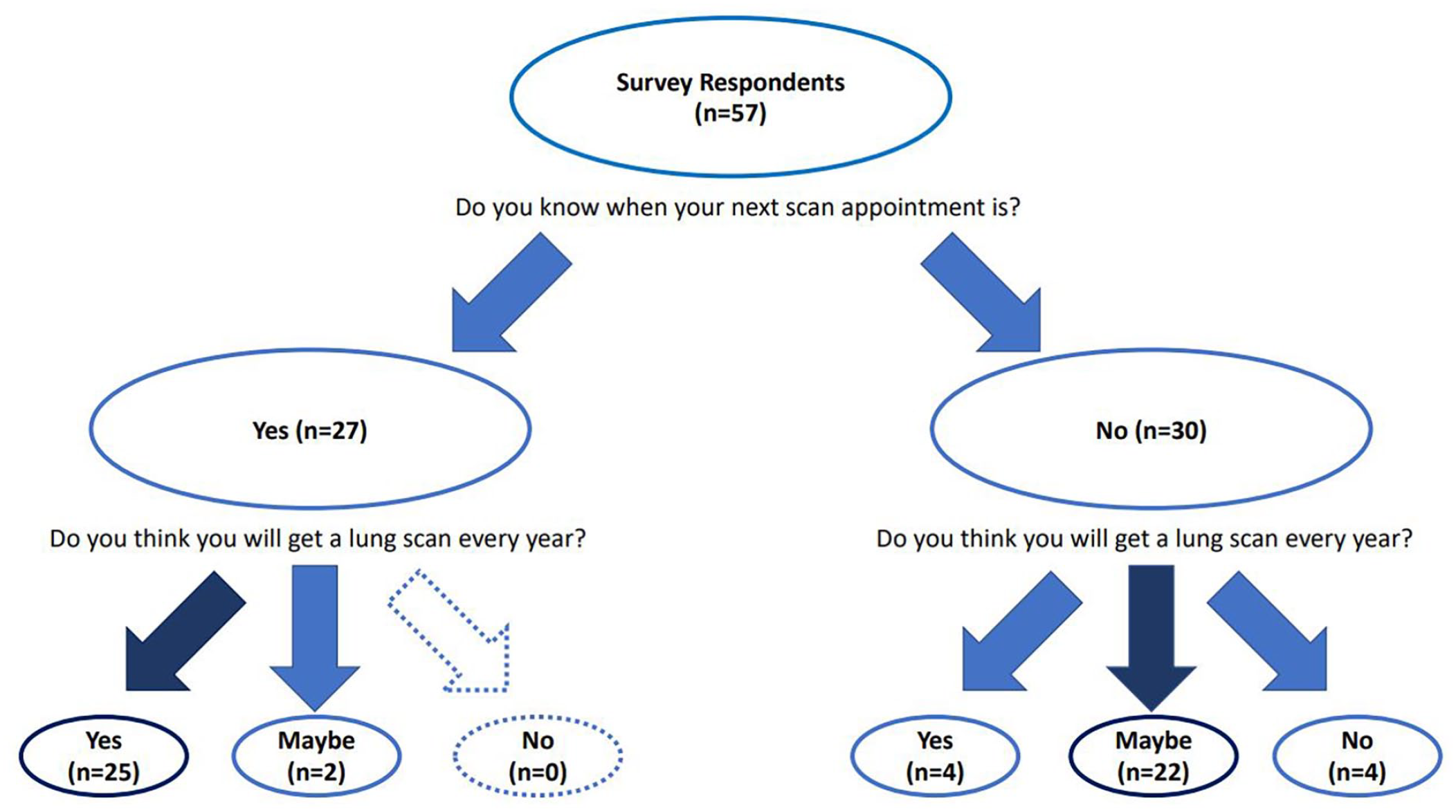
Intent to scan based on knowledge of next scan appointment.
We retrospectively examined the potential impact of the COVID-19 public health emergency (PHE), which began soon after screening started: The initial PHE began March 13, 2020 and ended July 6, 2021. The second PHE began August 13, 2021 and ended October 8, 2021. 17 Those screened between PHE periods—July 7-August 12, 2021—were included in the category “Pre/Post-COVID-19 State of Emergency.” Two factors connected to screening continuation—knowledge of next scan date and intent to continue—were compared for those screened before or after the state of emergency period with those screened during the state of emergency. Participants screened during the state of emergency expressed less certainty about dates of next scans (41% knowing date vs 53%) and more ambivalence about intention to continue screening (44% intending to screen annually vs 57%; Supplemental Table 1a and 1b).
Discussion
Education by CHAs and county coordinators was a primary influence on screening initiation for 69% of respondents, and 43% of these respondents indicated that this influence was the only reason they were screened. This shows the powerful influence of CHAs as messengers, at least when it comes to initiation of screening. That 65% of respondents reported at least 2 influences also indicates the value of varied influences to move some individuals to screening, as opposed to relying on the influence of PCPs during annual wellness visits. In fact, only 3% of respondents indicated that a doctor’s suggestion influenced them to initiate screening. This result contradicts findings of previous studies showing that perceived physician endorsement is a factor likely to promote screening. 18 However, it could also indicate that this population has less exposure to doctors for initial conversations about lung cancer screening. Data show that rural and Black communities are more likely to experience a shortage of primary care physicians and may not have a regular source of health care. 19
There is evidence to support the role of CHAs or community health workers to increase screening rates in medically underserved populations in a cost-effective way, particularly in breast, cervical, colorectal, and prostate cancer screening.20-22 CHA interventions focused on increasing breast screening among Black women specifically showed promise in moving these women to screening.23,24 Future efforts should focus on showing how CHAs can help increase lung cancer screening, particularly to fill gaps in primary care access in medically underserved communities.
For respondents who did not report the influence of a CHA or county coordinator’s suggestion, 8 out of 18 reported that seeing an advertisement for screening was the only influence. The intention of this mailer was to raise awareness of screening in general, not for the purpose of directing the recipient to a specific program. This style of outreach may be an effective communication strategy for reaching people in the target population not reached by CHAs.
While doctors were not seen as major influences for initiating screening (Table 2), healthcare providers strongly influenced decisions about continuation of screening (Table 3), for better or for worse. Respondents who planned to continue screening were heavily influenced to do so by their doctor’s recommendation. Respondents who did not intend to continue or who were ambivalent also indicated that messaging from their doctor led them to believe that annual screening was not necessary, which contradicts clinical guidelines recommending annual screening for certain populations. It is possible that these respondents were no longer at risk according to screening guidelines, but a clear difference in healthcare provider messaging was seen between those who intended to continue screening and those who did not or were unsure.
Communicating clear and consistent evidence-based guidelines is important for ensuring that patients continue screening at the appropriate intervals. Earlier research showed that primary care provider (PCP) knowledge of lung cancer screening benefits, harms, and recommendations was low and negatively impacted referral rates. 25 However, this lack of widespread awareness may have been exacerbated by the recommendation against lung cancer screening by the American Association of Family Physicians (AAFP) in 2013. 26 In April 2021, the AAFP revised their recommendation in favor of lung cancer screening, aligning with the USPSTF recommendation. 27 It may also be useful to explore in a larger sample whether patients are more likely to continue with screening if they have an appointment date for their next scan rather than being contacted at the appropriate interval. In this study, knowledge of the next appointment date was highly correlated with intention to continue screening.
When asked about intention of continuing screening, 3 respondents mentioned concern about cost and coverage. Two of these respondents were uninsured and one was a Medicare beneficiary. When asked if they planned to continue screening, they responded, “If I can afford it,” “If I can get some assistance to pay for it,” and “If my plan pays.” While the ability to afford screening is connected to insurance benefits, in rural locations, other financial barriers often include transportation and time off work. Helping offset cost through resources like gas cards can help overcome these barriers.
There were some limitations to this study. Screening through ALCASE began in December 2019. With the rollout of COVID-19 restrictions on public gatherings and face-to-face communication starting March 13, 2020, the ability of CHAs to educate about screening in person became limited. In addition, the focus of staff at UAB Comprehensive Cancer Center and the Alabama Department of Public Health shifted to pandemic response. Restrictions in Alabama did not ease enough to overcome months lost before the project ended. Despite these challenges, 23 of the 27 survey respondents screened during the state of emergency period indicated that the CHA or county coordinator influenced their decision to get screened, showing that CHAs were still able to connect with and educate those at high risk for lung cancer.
While the intention was to conduct the follow up interview within a consistent time period after screening, information transfer was sometimes delayed. Participants were not always told that the program manager was going to call them and did not answer calls from unknown numbers, which caused delays: while about 45% of participant surveys were conducted within 2 weeks of the screening scan, the rest were completed between 1 month and 11 months post-scan. Participants reporting their experiences after more time passed might remember it differently compared to how they remember it soon after the scan.
Conclusions
The primary objective of this analysis was to understand the barriers and facilitators to lung cancer screening initiation and retention for patients from mostly rural, predominantly Black communities in Alabama to inform healthcare providers about effective strategies for increasing lung cancer screening rates. ALCASE showed that use of CHAs may be a successful strategy to increase uptake of lung cancer screening in these communities. This study also showed that having multiple messengers and educational advertising can also support increased awareness of and interest in lung cancer screening. Clear guidelines-based messages from healthcare providers about recommended screening is important for increasing retention. COVID-19 related implementation challenges impacted the current study, and future research to further explore use of CHAs in lung cancer screening will add important data in this area. Studies looking at effective messaging from healthcare providers can help identify effective strategies to increase screening initiation and retention. In addition, future research exploring the level of influence of each reason for considering screening individually would help understand how to prioritize approaches to increase participation and retention.
Supplemental Material
sj-docx-1-jpc-10.1177_21501319231168022 – Supplemental material for Influences on Lung Cancer Screening Initiation and Retention in Rural Alabama
Supplemental material, sj-docx-1-jpc-10.1177_21501319231168022 for Influences on Lung Cancer Screening Initiation and Retention in Rural Alabama by Amy Copeland, Kathy Levy, Claudia M. Hardy, Jennifer C. King and Maureen Rigney in Journal of Primary Care & Community Health
Supplemental Material
sj-pdf-2-jpc-10.1177_21501319231168022 – Supplemental material for Influences on Lung Cancer Screening Initiation and Retention in Rural Alabama
Supplemental material, sj-pdf-2-jpc-10.1177_21501319231168022 for Influences on Lung Cancer Screening Initiation and Retention in Rural Alabama by Amy Copeland, Kathy Levy, Claudia M. Hardy, Jennifer C. King and Maureen Rigney in Journal of Primary Care & Community Health
Footnotes
Acknowledgements
The authors would like to acknowledge Shanada Monestime, PharmD, BCOP, Director, Community Engaged Research at GO2 for Lung Cancer for critical review of manuscript and contributing knowledge on health disparities and Tara Bowman, Program Manager at The O’Neal Comprehensive Cancer Center at University of Alabama at Birmingham for contributing additional requested data.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: JCK reports consulting and advisory board participation, all paid to GO2 for Lung Cancer, from Amgen, Boehringer Ingelheim, Bristol Myers Squibb, and EQRX and research funding paid to GO2 for Lung Cancer from Bristol Myers Squibb and Genentech. MR reports consulting and advisory board participation, all paid to GO2 for Lung Cancer, from AstraZeneca, Jazz, Novartis Global, and Gilead.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a grant from the Bristol Myers Squibb Foundation.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.