
Abstract
Physician burnout has been increasing in the United States, especially in primary care, and the use of Electronic Health Records (EHRs) is a prominent contributor. This review article summarizes findings from a PubMed literature search that shows the significant contributors to EHR-related burnout may be documentation and clerical burdens, complex usability, electronic messaging and inbox, cognitive load, and time demands. Documentation requirements have escalated and have inherently changed from paper-based records. Many clerical tasks have also shifted to become additional physician responsibilities. When considering factors of efficiency, effectiveness, and user satisfaction, EHRs overall have an inferior usability score when compared to other technologies. The volume and organization of data along with alerts and complex interfaces require a substantial cognitive load and result in cognitive fatigue. Patient interactions and work-life balances are negatively affected by the time requirements of EHR tasks during and after clinic hours. Patient portals and EHR messaging have created a separate source of patient care outside of face-to-face visits that is often unaccounted productivity and not reimbursable.
Introduction
Burnout
Physician burnout is prominent and manifests as a chronic stress response with components of depersonalization, emotional exhaustion, or impaired feelings of accomplishment. 1 Figure 1 shows the prevalence of at least one symptom of burnout from a surveys of U.S. physicians in 4 periods from 2011 to 2021. 2 The consequences of this burnout to healthcare may be expressed as major medical errors, poor quality of care, safety incidents, reduced patient satisfaction, and primary-care workforce turnover.3-5 Electronic Health Records (EHRs) are a significant source of burnout along with varying combinations of time pressures, chaotic work environments, low control of pace, family responsibilities, COVID-19 pandemic stressors.1,2

Prevalence of at least one symptom of burnout among U.S. physicians.
EHR and Burnout
Nearly 80% of hospitals 6 and 86% 7 of ambulatory clinics in the United States have implemented an EHR as of 2015 and 2017, respectively, and the adoption rates have likely increased significantly since then. As would be expected, the workflows and dynamics of providing healthcare have changed and will continue to adapt in the transition from paper-based records. A consequence of this evolution has been enhanced stress for providers. In fact, the prevalence of physician burnout has been increasing in all specialties in recent years with the highest levels reaching almost 50% in primary care in the United States. 8 The current state of the EHR is frequently pinpointed by physicians as the single most important stressor in patient care, 9 and nearly 75% with burnout symptoms identify the EHR as a source. 10
Billing and documentation have been the primary drivers of EHR design, not patient needs and health management.11,12 Physicians have acquired more administrative tasks, and, as a result, daily effort, workflow, and patient interactions have fundamentally changed. 12 In a 2018 national survey of 521 primary care providers (PCPs) by The Harris Poll on behalf of Stanford Medicine, half of PCPs believe that EHRs impair clinical effectiveness. 13 Nearly half (44%) also view the principle utility of EHRs as simply data storage, while only 3% see the primary value in disease management and prevention. 13 Ultimately, 59% of PCPs believe EHRs need a complete overhaul. 13 Figure 2 represents the prevalence of several EHR burnout characteristics from surveys. The goal of this literature review is to identify and characterize the specific aspects of EHR workflows that contribute to burnout.
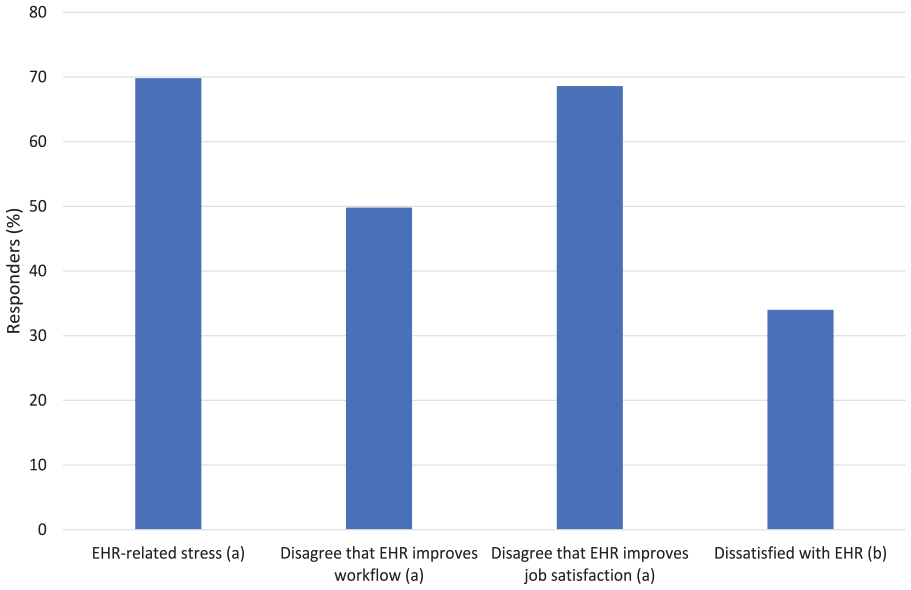
Physician views on EHR use.
Methods
Figure 3 is a summary of the literature search of PubMed completed in June, 2022 and February, 2023 to include articles 2010 to present. The search strategy was for titles having keywords that included the following: ([“EHR” or “EHRs” or “EMR” or “EMRs” or “electronic health record” or “electronic medical record” or “electronic health record” or “electronic health records” or “health information technology”] AND [“stress” or “burnout” or “time” or “clerical” or “frustration” or “fatigue” or “cognitive” or “burden” or “workload”]). Articles were filtered to English language only. Sequential title, abstract, and full text reviews were completed with the following exclusion criteria: (1) not applicable to primary care or general practice of medicine, (2) not involving EHRs in the U.S., (3) not related to physician burnout, and (4) editorials or commentaries. Reference sections from selected articles were also reviewed for additional relevant literature. Table 1 summarizes key findings from the 36 articles that were eligible for inclusion in this review at the end of the search.

Summary of literature search.
Summary of Key Findings From Included Articles.

Results
Contributors to EHR-related burnout may be organized into broad categories of time demands, documentation and clerical burdens, complex usability, cognitive load, and electronic messaging volume.
Documentation and Clerical Burden
The rising load of clerical tasks associated with EHRs and placed on clinicians is one of the more commonly identified reasons for burnout in medicine.39,49 Physicians have become responsible for entering not only diagnoses, orders, and visit notes but also additional administrative data of perceived low clinical value. 32 Nearly 69% of PCPs feel that most EHR clerical tasks completed by them do not require a trained physician. 13 In a survey of 282 clinicians from 3 institutions in California, Colorado, and New Mexico, of which 68% worked in primary care, the most prominent concern (86.9% of responders) about EHR use was the need for excessive data entry. 37 In fact, clinicians may need as much as 2 additional hours in electronic data entry for every hour of direct patient contact. 38 Physicians with insufficient time for documentation are 2.8 times more likely to report symptoms of burnout, 35 and in some cases clinic schedules are deliberately shortened and spots closed to allow sufficient time. 33
From purely clinical care standpoint, the primary reason for notes and documentation has been simply to describe what happened during a visit to provide details needed for the context of the next visit, continue a plan of care, and clarify factors that affect care of a patient. 36 Implementation of EHRs along with the evolving demands of additional stakeholders in the healthcare system have expanded documentation requirements to include billing criteria, quality measures, and compliance matters. 36 These external demands have lead to redundant and cumbersome data capture, 34 and the length of clinical notes alone have doubled since the Health Information Technology for Economic and Clinical Health Act 37 in 2009 provided financial incentives to adopt EHRs but with added needs to demonstrate meaningful use.
Complex Usability
The quality of a user’s experience with a technology in terms of effectiveness, efficiency, and overall satisfaction can be quantified with the System Usability Scale (SUS) to a score of 0 to 100, with the industry average at a 68. 50 For example, the SUS score for Google search of 93, a usability grade of A, is in the top 0.01% of technologies, and the score for Microsoft Excel of 57, a usability grade of F, is in the bottom 22%. 15 Overall EHR usability from a survey of US physicians between 2017 and 2018 has a SUS score of 45.9, which is in the bottom 9%, a usability grade of F, and is categorized as “not acceptable” in comparison to other products. 15
In The Harris Poll, 90% of PCPs felt that EHRs need to be more intuitive and responsive, and 72% believed that enhancing user interfaces would best address EHR challenges in the immediate future. 13 Interfaces can often be complicated by elements that are distracting, duplicated or clinically irrelevant. 16
Navigation seems inefficient in EHRs 35 at least partially as a result of complex webs of windows, icons, menus, and pointers. 19 Workflows can be hindered by long pull-down lists that are unfiltered or unorganized by context and by deeply nested menus. 19 Seemingly straight-forward tasks may also be divided inappropriately into several small steps with multiple scrolls, points, and clicks. 19 Streams of numerous dialog boxes to enter documentation also leads to mouse-click fatigue. 17
Security issues can also contribute to diminished usability by requiring multiple long-ins per patient and by requiring progressively more-complex passwords with also progressively shorter expiration periods. 18 Surprisingly, total clinic time spent on security tasks may equal time spent on reviewing problem lists. 18 When physicians at Yale School of Medicine switched to a badge tap log-in system to eliminate repetitive typing of username and password, up to 140 times per day individually, up to 20 min per day were saved along with removing the annoyance. 14
Cognitive Load
EHR-associated information overload impedes locating and identifying key clinical information and imposes substantial cognitive demands on physicians.11,40 In addition to inefficiency and the contribution to physician burnout, there is a risk to patient care in missing or overlooking critical data. 41 Nearly 70% of physicians in a survey of 2 Midwestern hospitals reported difficulties in finding needed information in the EHR from overload. 42 Data to be reviewed for a single patient encounter are often difficult to separate from clinically unnecessary information in EHR displays 37 and often organized in fragmented data groups in varying locations and formats.41,46 In a cognitive task analysis of experienced clinicians, the EHR was not found to be helpful in maintaining awareness of the big picture in care of a patient. 47
EHR notes can be challenging to cognitively process from bulky structures and cluttering with nonessential or repetitive details. 36 The use of templates and structured data entries can contribute by creating poor syntax and narrative flow of text. 36 Copying and pasting parts of previous notes is common with EHRs and can also generate lengthy, bloated notes with redundant information and errors. 33 More than half the content of 100 randomly selected resident progress notes at an urban academic medical center in New York was duplicated from previous notes. 51
Alerts and reminders also bring about information overload and cognitive fatigue.33,48 In a study of primary care clinics at a large, tertiary care Veterans Affairs (VA) facility, physicians received an average of 56.4 alerts daily and spent 49 min daily to process these. 45 In a separate study of focus groups from 2 large VA centers, the 3 most cited barriers from alerts were the high volume, workload, and perception that some alerts were unnecessary. 44 Making clinical decisions based on these alerts can be a considerable cognitive demand because many factors must be processed at the same time, such as degree of urgency, critical status, chart review, and determination whether the alert is simply informational or requires action. 43
Time Demands
Physicians may be spending 49.2% of total time in an average clinic day on EHR and desk work and only 27% in direct face time with patients. 38 In the exam room alone, EHR activity may represent up to 37% of visit time. 38 More than half of physicians in a 2014 survey by the Wisconsin Medical Society reported that the EHR has worsened patient interactions. 20 Nearly 62% of PCPs in the 2018 Harris Poll felt they had insufficient time to adequately address patient questions or concerns as a result of EHR time demands, and 69% felt that EHRs take valuable time away from patients. 13
A prevalent concern of nearly two thirds (63%) of physicians about EHR use is the interference with work-life balance. 37 Half of physicians feel too much time is spent on EHR use at home,22,23 and the odds of burnout for those physicians expressing moderately high to excessive home EHR time are nearly twice that for those reporting minimal home EHR time. 35 In nationwide data from the Arch Collaborative of more than 200 separate health organizations, physicians with home EHR charting of 5 h or less weekly were 2.43 times more likely to have lower burnout scores than those charting 6 h or more. 21
Electronic Messaging and Inbox
With the adoption of EHRs, patients have an alternate form of access to providers through patient portals and secure messaging, and the volumes of these messages are steadily rising. 27 Patient portal messages alone in primary care at the University of Wisconsin increased 62% from 2013 to 2016. 25 Additional EHR inbox messages that also encompass patient care tasks outside of a traditional face-to-face visit include patient call notes, form requests, refill requests, and referral responses.26,29 In a study of PCPs from 5 medical facilities within Kaiser Permanente, most EHR inbox effort was spent on patient messages, and stress duration measured by physiological sensors was longest for those who completed inbox tasks mostly outside of clinic hours. 31
The number of inbox messages addressed is a significant predictor of burnout. 26 In a study of primary care practices in a large academic health system in San Francisco, providers with more than 307 messages per clinical FTE per week (the highest quartile in the study) were 6 times more likely to have exhaustion compared to those with less than 147 messages (the lowest quartile). 24 In another retrospective cohort study in the ambulatory clinics of the 2 largest healthcare systems in Rhode Island, clinicians with high message volumes were 4 times more likely to report symptoms of burnout than those with fewer volumes, and inbox volume was the most significant predictor of burnout over other workload measures including number of daily appointments, time spend reviewing charts, number of orders placed, note length, and number of result messages. 26 In that study, PCPs received 4 times more messages than specialists. 26
The EHR inbox competes with other activities of a clinical workday and may have become nearly the equivalent of a second set of patients to be treated beyond scheduled patients. 28 In a qualitative study from interviews with PCPs across facilities of Kaiser Permanente Northern California, commonly voiced stressors from inbox management beyond workload alone were patient expectations for rapid replies, unlimited nature of the inbox, and a sense of urgency from a full inbox. 28 Unlike effort spent in care of scheduled patients, the added burden of care given through electronic messaging is also typically unmeasured productivity and not reimbursable. 30
Conclusion
EHRs may offer several advantages over paper-based records such as coordinating care between several health care providers and clinics, providing a mechanism for safer and reliable prescribing, having legible documentation, improving communication with patients, and enhancing the security of patient data. 52 However, EHRs have also created new or exacerbated traditional stressors for physicians and have become a pronounced contributor to burnout. Substantial clerical and data-entry burdens are newer, additional responsibilities for healthcare providers and frequently seem redundant and cumbersome. Portions of these documentation requirements involve issues such as billing, quality metrics, and compliance that may appear beyond fundamental patient care.
Compared to other forms of technology, EHRs also tend have a relatively poor overall usability score. This may be a at least partially a result of overly complex interfaces and inefficient, nonintuitive workflows. Information overload, bulky notes, alerts, and reminders further add the cognitive burdens in patient care. EHR activities may also take valuable clinic time away from direct patient interactions and take time after clinic hours that interferes with a healthy work-life balance. EHR inboxes are an added source of patient care tasks beyond traditional face-to-face visits. The number of inbox messages to be addressed has been increasing in the past several years, correlates with burnout, and often represents unmeasured productivity.
Footnotes
Author Contribution
JB is sole author and editor of the manuscript.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.