
Abstract
Introduction:
Cardiovascular disease (CVD) is the leading cause of death for males, females, and people of most racial and ethnic groups in the United States. In addition to known epidemiological and behavioral risk factors, recent evidence suggests that circumstantial or behavioral factors may also be associated with CVD. This study evaluates the contribution of cardiovascular disease (CVD) risk factors, community vulnerabilities, and individual health behaviors to individual physical and mental wellness among Black and White, male, and female Medicare beneficiaries.
Methods:
This study utilized data from the Behavioral Risk Factor Surveillance System, county-level CVD risk factor prevalence, and selected items from the Social Vulnerability Index.
Results:
Correlations were found between unhealthy days reported by males and area social vulnerabilities and health behaviors. Prevalence of disease was correlated with mentally unhealthy days for White males. Among White females, health behaviors, disease prevalence, and social vulnerability measures were associated with unhealthy days. Among Black females, disease prevalence was highly correlated with mentally unhealthy days.
Discussion:
While individual-level health behaviors are highly associated with perceived physical and mental health, the self-reported health of Black respondents is also heavily correlated with local area vulnerabilities, including community poverty, group housing, and crowding.
Keywords
Introduction
Self-rated health has received growing attention as a measure of population health, since it centers on the assessment of health status and relates to the population’s well-being and life satisfaction.1,2 While factors influencing self-rated health have been extensively studied,3-5 evidence suggests that self-rated health is a multidimensional construct with various domains, including demographics, lifestyle, and psychological and physical health6,7 which can differ according to age and gender.8,9 In most population studies, physical health tends to be the principal determinant of self-rated health while the influence of mental health on the assessment of overall health remains less clear.10,11 In addition, few studies have focused on the difference between factors associated with self-rated physical and mental health in the presence or absence of cardiovascular disease (CVD) risk factors and compared these associations across sex groups and racial population cohorts.12-14 Furthermore, relative differences in the contribution of behavioral, environmental, and epidemiological risk factors to self-reported health among racial, ethnic, and sex cohorts has not been studied. We hypothesize that this gap in the current literature has lead researchers and clinicians to undervalue the role of social circumstances in reported physical and mental health—particularly among females and minoritized groups.
The investigation of sex differences in self-reported health has amassed a large body of evidence with females reporting low levels of general health compared to men.15-18 Sex differences in the epidemiology, symptomology, treatment, and outcomes of CVD have been attributed to biological pathways19,20 as well as social constructs. 21 Among patients with CVD, females consistently report worse health-related quality of life and greater disability related to their disease. An investigation using 10-years of data from the Medical Expenditure Panel Survey found that compared to males, females with atherosclerotic cardiovascular disease were more likely to perceive their health status as poor and report lower quality of life scores. 22 A growing body of evidence suggests clinically relevant differences between males and females such as hormone production, response to treatment, and the prevalence, presentation, management, and outcomes of the disease, but little is known about why CVD affects males and females differently. 23 Similarly, in a prospective study of patients with peripheral artery disease, Dreyer et al found that females reported worse physical and mental health compared to men despite similar clinical characteristics. At 12-months, there were no differences in mortality or serious adverse events between the groups yet, female patients continued to report worse physical and mental health scores suggesting systematic differences in reporting between males and females. 24 In additional to distinct sex-differences in self-reported health, race-associated disparities in self-reports have been identified in the self-rated physical and mental health of individuals living with CVD.25-28
Black individuals consistently report poorer health, even when age, chronic health conditions, and a host of additional individual-level covariates are considered.29,30 While some studies suggest that Blacks and Whites may evaluate their health differently,31,32 an abundance of psychometric investigations that attest to the validity of self-reports of health have led researchers to believe that, in general, differences detected between racial groups are real rather than an artifact of the measurement method.33,34 In short, extant research offers strong evidence of a substantive race differential in self-reports of health but, as yet, has not yielded a convincing explanation for this discrepancy. Conversely, there are well-established Black–White disparities in the prevalence of CVD risk factors with the Black population experiencing higher rates of diabetes, hypertension, and heart disease than other racial groups, leading to disproportionate cardiovascular morbidity, mortality, and poor quality of life.35-37 In fact, CVD mortality occurs at a younger age and overall mortality rates are higher at most ages for Blacks compared to Whites.38-40
Studies indicate that racial differences relate in part to socioeconomic factors, process-of-care variables, and patient preferences, whereas sex differences relate in part to physiological factors. In both cases, however, understanding is limited by deficiencies in currently available datasets. Moreover, factors that have been shown to contribute to race and sex disparities in medical care fail to explain them fully. 41 In addition, Blacks experience stressors generated by systemic racism in the form of lower socioeconomic status, higher likelihood of residing in poor neighborhoods, barriers to quality healthcare, and lower health literacy which is often intensified by strained resources.42-45 Closely related to this finding is minority members’ common reluctance to seek care in anticipation of cultural barriers, such as patient-doctor miscommunication, or racial prejudice from the healthcare professional. 46
Geographic residence and neighborhood characteristics have begun to emerge as important determinates of health outcomes. The structural characteristics of a neighborhood determines whether it is feasible to take a walk, shop for groceries, or remain engaged in community-based activities.47,48 Living in an area with a lower median income is associated with increased deprivation of healthy foods, green spaces, community programs, and recreation opportunities that might mitigate poor health behaviors and the accumulation of CVD risk factors. 49 Neighborhoods and communities with a higher prevalence of minority members have been associated with deprivation, characterized as food deserts, with high crime rates, and frequent exposures to air and water pollutants, all factors associated with a higher likelihood of developing CVD.50-52 Despite the association between environmental and community vulnerability and health disparities, community and neighborhood characteristics are often absent from research examining disparities in self-reported health.
As a person ages, systemic racism has a cumulative effect on individual health throughout the lifespan leading to a persistence in health disparities. 53 Advancing age is also associated with inevitable changes in cardiovascular structure and function. Access to and utilization of healthcare among the elderly is important in the detection and management of CVD—the leading cause of mortality among the elderly, (age≥65). 54 CVD risk factors (ie, hypertension, dyslipidemia, and type 2 diabetes) and poor lifestyle behaviors are significant contributors to the occurrence of cardiovascular events, such as heart attack and stroke. Among Black populations, CVD-related events tend to be more severe and as a consequence, result in increased disability and higher mortality rates. 55
Since older adults compose the most rapidly growing subset of the population, this study focuses on individuals aged 65 and over enrolled in fee for service Medicare in 2018. Since self-reported health has been shown to be predictive of morbidity and mortality, even after controlling for baseline health status,56,57 this analysis quantifies health using the number of self-reported physically and mentally unhealthy days per month. Empirical analysis assesses the relationship between these metrics and individual-level preventative health care, community-level vulnerability measures, and county-level prevalence of CVD risk factors. While CVD and CVD risk factors impact both physical and mental health, CVD screening, treatment, and risk management are provided to Medicare beneficiaries. Despite the coverage of these services, many areas still show high rates of hypertension, hyperlipidemia, and diabetes suggesting that these Medicare services are either not available, not effective, or not utilized. Therefore, it is important to evaluate the relative influence of CVD risk factors, community inequities, and health behaviors on self-reported health. The use of multiple levels of data—individual, county, and systems—allows this study to compare the relative influence of multiple, interrelated factors on individual health.
The evaluation of these factors and their contribution to the health of the aged population is becoming increasingly important as the geriatric proportion of the US populations grows. By 2030, 1 in 5 persons in the US will be over age and by the middle of this century, there will be more than 80 million older adults. The population is not only getting older but also becoming more diverse; that is to say, ethnic, and racial minorities represent an increasing proportion of the population. Soon, nearly 1 in 4 older adults will be from a racial minority group. The aggregation of lifelong patterns of disadvantage can manifest later life as poor perceived health and/or chronic disease. Identifying individual, community-level, and CVD risk factor determinates of self-reported health is increasingly important when assessing racial disparities and sex differences in self-reported physical and mental health among elderly Americans.5,58
Methods
This study used data from 3 primary sources: the Behavioral Risk Factor Surveillance System Selected Metropolitan/Micropolitan Area Risk Trends (SMART) (individual level), the Centers for Disease Control and Prevention Social Vulnerability Index (CDC SVI) (community level), and the Centers for Medicare and Medicaid Services (CMS) County Level Chronic Conditions Table: Prevalence, Medicare Utilization and Spending (structural/health systems level). Each of the data source is briefly described below followed by the data integration technique and analysis strategy. Centers for Disease Control and Prevention (CDC) Human Research Protection Program (HRPP) Institutional Review Board (IRB) reviewed and approved the data for this study.
This analysis limited the BRFSS respondents to only those aged 65 and over with an identifiable MMSA code. Respondent demographic characteristics selected for this analysis included age, race, ethnicity, educational attainment, being overweight, marital status, and veteran status. Additionally, binary indicators for having a regular physician, visiting a dentist within the last 2 years, having a mammogram within the last 2 years (females only), receiving the pneumonia vaccine, and always wearing a seatbelt were added to account for use/availability of preventative health services and behavioral heterogeneity. While the BRFSS contained additional indicators for health services and health behaviors, a parsimonious list was used to avoid serial correlation in regression estimates.
SVI: The degree to which a community exhibits certain social conditions describes a community’s social vulnerability. The CDC SVI59,60 evaluates census tracts on 15 social factors, including unemployment, minority status, and disability and groups them into 4 related themes: socioeconomic, household composition and disability, minority status and language, and housing and transportation. The SVI social factors include items related to potentially permeable population subsets, therefore not every indicator is relevant to every member of a community, but the aggregation of these factors quantify the average vulnerability of the entire community. As a result, applications of the SVI increasingly link vulnerability or elements of vulnerability to health behaviors, outcomes, and characteristics such as physical activity, physical fitness, and teen pregnancy.61-63 Since this study focused on Medicare beneficiaries aged 65 and above, only items relevant to the circumstantial or contextual environment of this age cohort were included in the analysis. Five items were selected: the percentage of persons living in group quarters (defined as places where unrelated people live or stay in a group living arrangement, ie, owned or managed by an organization providing housing and/or services for the residents), percentage of persons below poverty, percentage of households with no vehicle available, percentage minority (all persons except white, non-Hispanic), and the percentage of occupied housing units with more people than rooms. SVI items are provided for every county in the US with an available nonzero population estimate from the US Census Bureau or for which sufficient data was available for calculation.
A Medicare beneficiary was considered to have a chronic condition if the CMS administrative data had a claim indicating that the beneficiary received a service or treatment for the specific condition. Beneficiaries may have had more than one of the 21 chronic conditions included in the published data. Prevalence estimates were calculated at the state and county level by taking the beneficiaries with a particular condition divided by the total number of beneficiaries in the fee-for-service population. Since this study chose to focus on CVD risk factors, the county-level prevalence of diabetes, hypertension, and hyperlipidemia was used.
Results
Table 1 provides descriptive statistics. Individuals are on average between 72 and 73 years of age (SE = 0.07). One-third of Whites had a college diploma compared to 15% and 18% of Black males and females. Between 26% and 36% of Whites males and females were overweight compared to 22% and 23% of Black males and females. Nearly 70% of White males were married (45% White females) compared to only 49% of Black males (27% Black females). Roughly 40% of males were veterans (2% of females). Receipt of health services differed greatly between Blacks and Whites. Over two-thirds of Whites received the pneumonia vaccine compared to only about half of Blacks. Similarly, 80% of Whites visited the dentist within the last 2 years, compared to only 68% of Black males and 71% of Black females. Most White (males 93%, females 95%) and Black (89% males, 93% females) Medicare beneficiaries had a regular doctor.
Descriptive Statistics by Race and Sex.
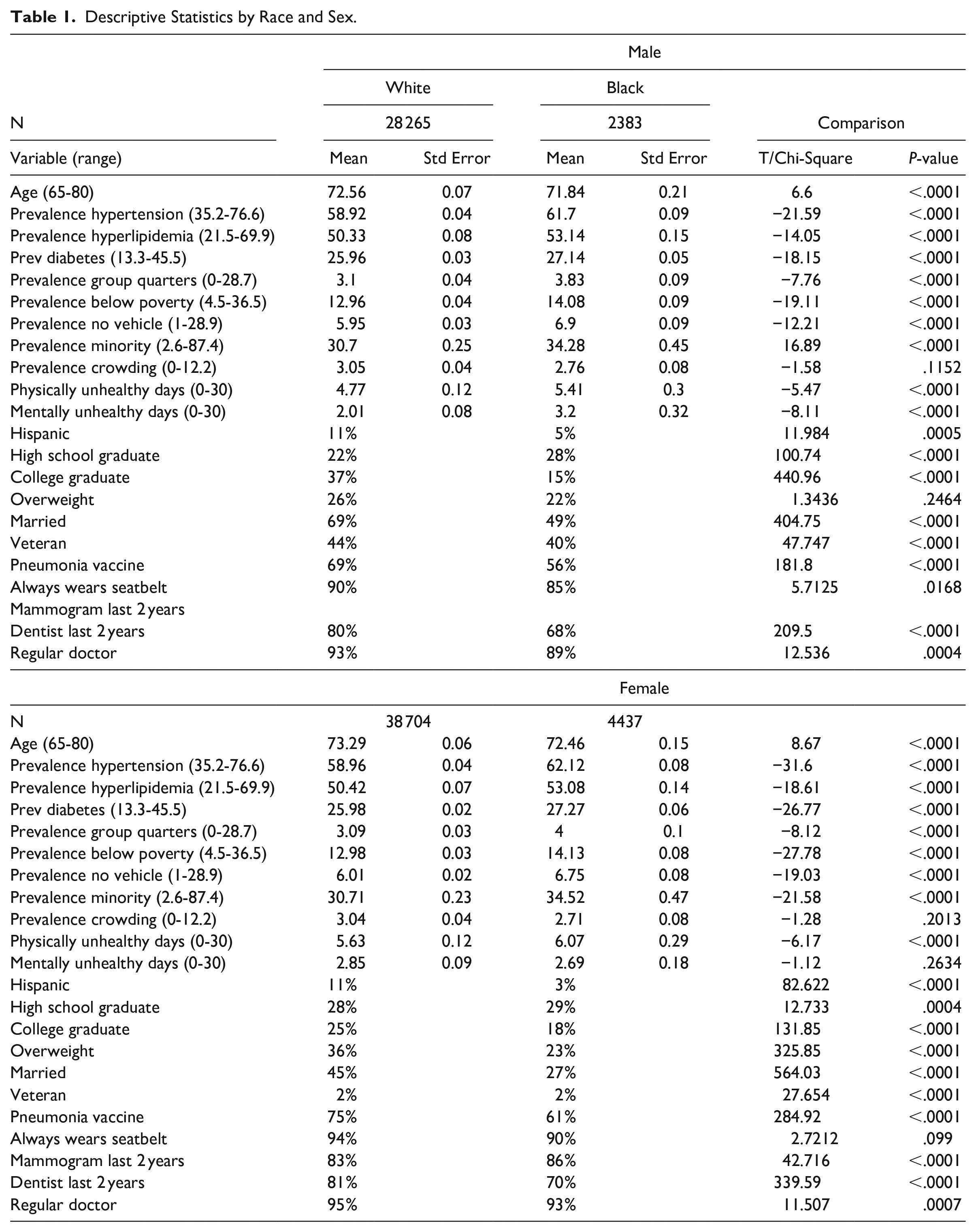
The prevalence of hypertension, hyperlipidemia, and diabetes was higher for Black males than White males and Black females than White females in their counties of residence and differences were statistically significant. Additionally, Blacks lived in areas with a significantly higher prevalence of group quarters, households with no vehicle, poverty, and minority residents than Whites. However, White males and females resided in counties with more crowding (males 3.05%, female 3.04%) than Black males (2.76%) and females (2.71%), but differences were not statistically significant (males t = 1.58, P = .1152, females t = 1.28, P = .2013). White males (4.77, SE = 0.12) and females (5.63, SE = 0.12) reported fewer physically unhealthy days than Black males (5.41, SE = 0.30) and female (6.07, SE = 0.29) (males t = 5.47, P < .0001; females t = 6.17, P < .0001). Additionally, White males (2.01, SE = 0.08) had fewer mentally unhealthy days than Black males (3.20, SE = 0.32) (t = 8.11, P < .0001). However, White females (2.85, SE = 0.09) had slightly more mentally unhealthy days than Black females (2.69, SE = 0.18), but the difference was not statistically significant (t = 1.12, P = .2634).
Physically Unhealthy Days: Poisson model results of physically unhealthy days for Black and White respondents by sex are listed in Table 2. After controlling for demographic factors, CVD risk factors, were significant only among females. White females living in an area with a greater prevalence of hyperlipidemia (11.62, SE = 2.81) and diabetes (9.60, SE = 3.37) reported more physically unhealthy days. Of the CVD risk factors evaluated, only prevalence of hyperlipidemia was significantly associated with the number of physically unhealthy days for Black females (13.54, SE = 6.84).
Relationship between CVD Risk Factors, Area Vulnerabilities, and Receipt of Health Services and Reported Physically Unhealthy Days.

Bold denotes significance and the 95% confidence level.
Estimates are weighted to reflect the population distribution.
Dependent Variable: Number of Physically Unhealthy Days in the Last 30.
Social vulnerabilities factors related to more physically unhealthy days for White males included prevalence of groups quarters (0.85, SE = 0.33), minorities (2.20, SE = 0.47), and crowding (2.62, SE = 0.54). Among Black males, prevalence of groups quarters (3.33, SE = 1.36) and poverty (9.61, SE = 4.09) were significantly correlated with the number of physically unhealthy days. White (0.58, SE = 0.33) and Black (1.80, SE = 0.86) females reported more physically unhealthy days related to the prevalence of group quarters. Minority prevalence was associated with physically unhealthy days for White females (0.96, SE = 0.47).
Individual health behaviors significantly associated with fewer physically unhealthy days among White males included receiving the pneumonia vaccine (−4.57, SE = 0.56), wearing a seatbelt (−2.21, SE = 0.78), visiting the dentist (−5.31, SE = 0.60), and having a regular doctor (−3.43, SE = 0.96). Only receipt of the pneumonia vaccine (-12.97, SE = 1.97) was associated with fewer physically unhealthy days for Black males. Among White females, all evaluated health behaviors had a significant influence on reporting fewer physically unhealthy days: receiving the pneumonia vaccine (−3.84, SE = 0.58), wearing a seatbelt (−3.60, SE = 1.05), mammogram in the last 2 years (−3.67, SE = 0.65), visiting the dentist (−7.14, SE = 0.64), and having a regular doctor (−2.33, SE = 1.13). For Black females, wearing a seatbelt (−7.06, SE = 2.14), having a mammogram (−3.78, SE = 1.79), and having a regular doctor (−5.92, SE = 2.89) were associated with better physical health.
Mentally Unhealthy Days: Poisson model results of mentally unhealthy days are listed in Table 3. A higher county-level prevalence of hypertension (26.16, SE = 7.44), hyperlipidemia (9.30, SE = 3.29), and diabetes (15.36, SE = 3.91) was associated with more mentally unhealthy days for White but not Black males. Among females, the prevalence of hypertension was significantly associated with more mentally unhealthy days for both White (16.60, SE = 6.03) and Black (40.14, SE = 20.40) females. Hyperlipidemia was associated with more mentally unhealth days only for White females (8.46, SE = 2.66), while diabetes was associated with more mentally unhealthy days only for Black females (24.76, SE = 11.89).
Relationship Between CVD Risk Factors, Area Vulnerabilities, and Receipt of Health Services and Reported Mentally Unhealthy Days.

Bold denotes significance and the 95% confidence level.
Estimates are weighted to reflect the population distribution.
Dependent Variable: Number of Mentally Unhealthy Days in the Last 30.
The only significant neighborhood vulnerability related to mental unhealthy days for White males was the prevalence of group quarters (1.50, SE = 0.38). Among Black males mentally unhealthy days were associated with group quarters (3.94, SE = 1.82) and crowding (9.02, SE = 3.13). Among White females, mentally unhealthy days were related to poverty (3.55, SE = 0.91), no vehicle access (3.08, SE = 0.66), and crowding (2.42, SE = 0.52), while only poverty was related to mentally unhealthy days for Black females (9.42, SE = 3.12).
Among White males, receiving the pneumonia vaccine (−2.01, SE = 0.63) and wearing a seatbelt (−6.31, SE = 0.86) were associated with a lower number of mentally unhealthy days; however, visiting the dentist (3.67, SE = 0.68) was related to more mentally unhealthy days. Among Black males, receipt of the pneumonia vaccine was related to fewer mentally unhealthy days (−7.85, 2.57). Among White females, fewer mentally unhealthy days was significantly related to receiving the pneumonia vaccine (−1.80, SE = 0.55), wearing a seatbelt (−4.55, SE = 0.97), mammogram in the last 2 years (−2.75, SE = 0.61), visiting the dentist (−5.19, SE = 0.60), and having a regular doctor (−2.49, SE = 1.14). For Black females, having a regular doctor (−7.45, SE = 3.18) was significantly associated with fewer mentally unhealthy days.
Discussion
The purpose of this study was to investigate the effects of disadvantage, at the individual and community-levels, and CVD prevalence on self-reported physical and mental health among elderly Medicare beneficiaries. Our findings of worse self-reported health in females, relative to males are consistent with other studies.15-18 Similar patterns of poor mental and physical health among the sex and racial groups suggest some overlap in the experience of these self-reported health outcomes. These results suggest that although the community-level prevalence of CVD risk factors was higher among Black respondents compared to White respondents, the influence of disease prevalence on self-reported health differed by the type of health outcome assessed. For White males, disease prevalence was related to worse mental but not physical health. For Black males neither physical nor mental health were associated with disease prevalence. These findings among males could reflect support the Black-White health paradox –the tendency for Blacks to report better mental health compared Whites despite a higher prevalence of chronic disease.64,65 This theory was supported by a 25-year investigation of the relationship between multimorbidity and mental health among 1034 Black and White respondents. Findings indicated that White respondents with multimorbidity at baseline reported a greater increase in depressive symptoms over the 25-year study period, but no increase was found among Black participants. 64 However, in our study the Black-White health paradox was not found among females given that Black females exhibited a greater increase in the number of poor mental health days as the prevalence of CVD risk factors increased.
Evaluating the effect of neighborhood characteristics on self-reported health, we found that more physically and mentally unhealthy days were reported among males and females of both races with higher levels of crowding, group quarters, minority residents, and no vehicle (often referred to as high neighborhood vulnerability). The prevalence of group quarters was positively related to more physically unhealthy days for all groups, as well as more mentally unhealthy days for both White and Black males. Limited research has been conducted on the relationship between group quarters (ie, places where unrelated people live or stay in a group living arrangement) and self-reported health. In the SVI, group quarters can include a variety of residential typologies including prisons, residential treatment centers, and college dorms which confounds comparability with results from other investigations of specific group housing configurations. However, prior studies using American Community Survey (ACS) data, which provided estimates for the SVI group quarters, has found that group quarter residency rates are higher among older individuals with disabilities, young males with disabilities, and individuals who are Black.66,67 The higher rates of disability among those living in group quarter housing may have contributed to the correlation between physically and mentally unhealthy days, particularly for males who are more likely to reside in these establishments.
A second measure of housing—the prevalence of crowding, was related to more physically unhealthy days for White males and more mentally unhealthy days for Black males and White females. The prevalence of crowding was similar between racial groups and males and females. Unlike group quarters, several investigators have studied the effects of household crowding and found it to be associated with infectious disease and poor mental health.68-71 In addition, the association between household crowding and health likely begins in childhood. Evidence suggests that children who grow-up in crowded households are more likely to exhibit behavioral problems which can lead to poor mental and physical outcomes in adulthood.72,73 As adults, personal characteristics including individual’s past experience, personal preference, and ability to cope can alter their perception of crowding. 74 The various measurements used to define crowding—proportion of people to rooms, perception that there are too many people in the available space, or community-density further complicate comparisons.
Numerous studies have linked neighborhood economic status to self-reported health.75-77 In our study, the percentage of individuals living below poverty was related to more physically unhealthy days only for Black males and more mentally unhealthy days for White and Black females. Investigators have found that extended exposure to neighborhood poverty is related to worse health outcomes 77 and Black individuals are less likely to experience neighborhood mobility, that is, minority children who are born in poor neighborhood are more likely to experience prolonged exposure to neighborhood poverty compared to Whites. 78
In our study, the racial composition of an individual’s neighborhood was also associated with more physically unhealthy days but only for White males and female. Robert and Ruel found similar results using national survey data. In their model, older White residents living in counties with a high prevalence of minority residents relative to the county-level percentage has worse self-reported health, which persisted after adjustments were made for overall percent of minority residents at the county-level, percent poverty, and individual age and gender. 79 This relationship between minority prevalence and poor self-reported health was not found among Black respondents. Rather, older Black adults living in counties with a higher percentage of minority residents reported better health compared to those living in counties with fewer Black residents. 79 Our results, and the findings of others, suggest that living in a neighborhood with a high density of minority residents may be associated with worse self-reported health among White and Borrell adults, but better health for Black adults.27,79,80 The elevated prevalence of poor self-reported health by White residents living in neighborhood with a high concentration of minority residents could be a consequence of concentrated disadvantage resulting in neighborhood deprivation. It is plausible that Black residents are somewhat protected from the effects of residential segregation through strong family and social networks which may mitigate the effects of neighborhood deprivation and result in a lower likelihood of poor health.81,82
Individual-level health behaviors were related to better self-reported physically and mentally unhealthy days among all groups. White males and females who engaged in all examined health behaviors perceived fewer physically unhealthy days. White females engaging in health behaviors reported fewer mentally unhealthy days, while for White males, fewer mentally unhealthy days was only associated with receipt of a pneumonia vaccine and wearing a seatbelt. Among Black males, the only health behavior related to fewer physically or mentally unhealthy days was receipt of the pneumonia vaccine. Black females had fewer physically unhealthy days when they reported wearing a seatbelt and having a recent mammogram; and had fewer physically and mentally unhealthy days when they reported having a regular doctor. In our sample, overall engagement in health behaviors was high across all sex and racial groups. Black respondents were less likely to report engaging in health behaviors compared to White respondents, with one exception—there was a greater prevalence of having a mammogram in the previous 2 years among Black females relative to White females. A higher prevalence of breast cancer screening among Black females is consistent with previous studies using the BRFSS and National Health Interview Survey data.83,84 Although historically mammography rates were lower among Black females, more recent public health campaigns have publicized findings that Black females are more likely to be diagnosed with breast cancer at a younger age and have a higher incidence of breast cancer subtypes associated with worse outcomes. Plausibly, these campaigns coupled with provider education has been effective in increasing breast cancer screening among Black females. Among Black respondents, particularly Black males, engaging in health behaviors did not have the same level of association with self-reported health.
Lack of awareness in both the public and medical community, as well as existing knowledge gaps regarding sex-specific differences in presentation, risk factors, pathophysiology, and response to CVD treatment, further contribute to outcome disparities. There is a critical need for implementation of sex- and gender-specific strategies to mitigate disparities in CVD outcomes. 85 However, the context in which these outcomes occur and the associations with demographic, social, and structural determinants must first be understood. While this study was not intended to provide a comprehensive review of the factors associated with sex and race outcome disparities, it characterizes the influence of various individual, structural, and environmental vulnerabilities on Black and White male and female Medicare beneficiaries. Additional research is needed to evaluate the full spectrum of associations and inform innovative solutions to improve outcomes for all patients with CVD.
Our results should be considered within the context in which they were contrived. First, this study integrated data from CMS, BRFSS, and CDC SVI based on MMSA codes. Therefore, the analysis sample represents residents of micropolitan and metropolitan areas, rather than the full national level population. Our sample originated with individual responses to the SMART BRFSS. Like all self-report data, the SMART BRFSS is subject to recall bias and participants may overreport health behaviors to respond to questions in a socially desirable manner. An overestimation of self-reported mammography screening has been found in comparisons of self-report to medical record data 86 in addition, the degree of overestimation can vary based on demographic characteristics with younger and Black females being more likely to overestimate their participation in breast cancer screening. 87 However, this bias may not exist for all health behaviors. Investigators using 2016 BRFSS data found a strong positive correlation between self-reported and observed seatbelt use at the state-level. 88 Second, while we did identify important racial differences in perceived health related to community deprivation, CVD risk factor prevalence, and health behaviors, the cross-sectional design of the current study precluded our ability to determine the direction of these associations. For example, whether participation in health behaviors contributed to better self-report health or whether an individual’s health perception influenced their likelihood of engaging in health behaviors cannot be determined, future prospective studies are needed to investigate the causal relationships between self-reported health and health behaviors. Additionally, due to sample size limitations, this study only included Blacks and Whites, but future studies should strive to incorporate a more diverse population. Lastly, there were additional social vulnerabilities and health behaviors, both observed and unobserved, that could influence self-reported health yet were not included in our analysis.
Conclusion
Our findings revealed the importance of social vulnerability, CVD risk factor prevalence, and individual health behaviors on self-reported physical and mental health. Although Black females reported the highest number of unhealthy days, followed by White females, Black males, and White males, the factors associated with the perceived health of each sex and race cohort varied significantly. As we originally hypothesized, social and community-level factors were more likely to be associated with poor self-reported mental and physical health among Blacks than Whites. However, individual-level health behaviors were significantly correlated with physical and mental health among Whites, but Blacks’ perceived health was also related to community-level social vulnerabilities including community poverty, group housing, and crowding. However, these estimates only reflect the relative correlation between self-reported health and these factors. Unmeasured or unobserved factors could undoubtedly also play a role as well as the co-occurrence of multiple area vulnerabilities. A variety of personal, epidemiological, and contextual interact to mutually determine an individual’s health and their self-reported health outcomes. However, disparities in community-level social determinates of health must be addressed to improve the self-reported physical and mental health of elderly minority residents.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.