
Abstract
This qualitative study evaluates physician training and experience with treatment and prevention services for people who inject drugs (PWID) including medications for opioid use disorder (MOUD) and HIV pre-exposure prophylaxis (PrEP). The Behavioral Model of Healthcare Utilization for Vulnerable Populations was applied as a framework for data analysis and interpretation. Two focus groups were conducted, one with early career physicians (n = 6) and one with mid- to late career physicians (n = 3). Focus group transcripts were coded and analyzed using thematic analysis to identify factors affecting implementation of treatment and prevention services for PWID. Respondents identified that increasing the availability of providers prescribing MOUD was a critical enabling factor for PWID seeking and receiving care. Integrated, interdisciplinary services were identified as an additional resource although these remain fragmented in the current healthcare system. Barriers to care included provider awareness, stigma associated with substance use, and access limitations. Providers identified the interwoven risk factors associated with injection drug use that must be addressed, including the risk of HIV acquisition, notably more at the forefront in the minds of early career physicians. Additional research is needed addressing the medical education curriculum, health system, and healthcare policy to address the addiction and HIV crises in the U.S. South.
Keywords
Introduction
The opioid crisis has devastated the U.S. with opioid overdose deaths climbing above 93 000 amidst the COVID-19 pandemic in 2020—a 29% increase from 2019. 1 Among persons who inject drugs (PWID), over 80% inject primarily opioids, 2 placing them at risk for opioid overdose. However, this is not the only health threat facing PWID. Infectious complications of injection drug use (IDU) further contribute to the morbidity and mortality of the opioid epidemic, compounded by the recent surge in methamphetamine use. 3 PWID are at risk of acquiring both bacterial and viral infections—representing a growing share of infective endocarditis hospitalizations, new human immunodeficiency virus (HIV) diagnoses, and acute hepatitis C (HCV) infections4,5 to name a few.
Following a 60% increase in opioid-related hospitalizations from 2009 to 2014, the U.S. healthcare system is gradually adapting its response to injection-related infections. 6 While the previous norm was reactively treating these infectious complications, the system is shifting into a norm of preventing them by addressing the underlying opioid use disorder (OUD) when present. 6 Medications for opioid use disorder (MOUD) (ie, methadone, buprenorphine, and naltrexone) lower illicit opioid use and reduce all-cause mortality. 7 Further, MOUD serve as HIV prevention by decreasing injection and sexual behaviors that increase the risk of HIV transmission, 8 while agonist therapies (ie, buprenorphine, methadone) have been associated with a lower risk of HCV infection. 9 HIV pre-exposure prophylaxis (PrEP) also expands providers’ ability to combat the infectious complications of IDU. Though sexual contact remains most prevalent method of transmission, sharing syringes is second riskiest behavior for HIV acquisition, and PWID account for 1 in 10 new HIV diagnoses in the U.S. 10 While tenofovir disoproxil fumarate-emtricitabine (TDF/FTC) was initially approved by FDA only for HIV PrEP in adults at risk for sexually acquired HIV, 11 the 2021 Clinical Practice Update from the U.S. Public Health Service 12 specifically includes recommendations for its use for PWID that either have HIV-positive injecting partner or more generally share injection equipment. However, despite a U.S. Preventive Services Task Force (USPSTF) Grade A recommendation to offer HIV PrEP to PWID, the adoption of this preventive tool remains fragmented. 13
The uptake of MOUD and HIV PrEP for PWID is lagging across the U.S. In the U.S. South, decreased accessibility is both a part of, and a result from, the unique convergence of vulnerabilities affecting PWID including rurality, restrictive policies (eg, lack of Medicaid expansion, illegality of syringe service programs), and stigma. 14 Because of these barriers, PWID often delay medical care until they are severely ill and require acute medical services in the hospital or urgent care facility. Hence, the hospital setting may be the only touch point for addiction treatment and prevention services. Previous research has revealed barriers to addiction treatment in rural America and PrEP opportunities in more urban areas,14,15 but the intersection of addiction care and HIV prevention remains understudied. In order to implement evidence-based, integrated care for PWID, we must explore provider-level barriers and opportunities for integrated addiction and HIV prevention services in the U.S. South, where robust harm reduction services are lacking.
The objective of this study is to evaluate healthcare provider experience and training around addiction care and HIV prevention services, understand their willingness and capacity to provide integrated services, and elucidate barriers and opportunities in caring for PWID. We applied a behavioral model for at-risk populations to conceptualize focus group data. 16 Because of well-described and aforementioned barriers to outpatient care in PWID, we focused our study on providers who serve PWID in inpatient and outpatient hospital-based settings. We recruited physicians who had no formal addiction medicine training (ie, they were not board-certified in Addiction Medicine and did not have previous formal training to treat opioid use disorder, such as an X-waiver) to understand how providers may support integrated addiction and HIV prevention services, expanding capacity within the existing workforce.
Materials and Methods
Study Design
The present study used qualitative focus group data from a study investigating implementation strategies for integrated MOUD and HIV prevention care for PWID. A phenomenological approach was used to describe healthcare providers’ experiences with, and perspectives on PWID who are hospitalized for complications of IDU including viral and bacterial infections. Because the vast majority of PWID in this population inject opioids, attitudes toward MOUD were also queried. 17 Two focus groups were conducted, one with early career physicians and one for mid-late career physicians.
Study Sampling and Recruitment
Healthcare providers were recruited via word-of-mouth and email to Infectious Disease and Internal Medicine clinical teams that provide hospital-based medicine service. Provider inclusion criteria were current employment at an academic medical center located in Alabama as a physician on a clinical service providing care for PWID in inpatient or outpatient settings. Providers were purposely sampled at the trainee to early career stage for the first focus group and at the mid- to late career stage for the second focus group to account for changes in contemporary medical training, which increasingly emphasizes stigma reduction and the evidence-based care of addiction (eg, MOUD). 18
Trained research staff informed participants of the focus group opportunity and scheduled them for one of the 2 groups. Focus groups were conducted via the videoconferencing platform, Zoom. The study recruitment and consent processes described the objective as an effort to understand healthcare providers’ perceptions of care for PWID, with the overall goal to inform future development of integrated services. This information was provided via an information sheet, participants were given the opportunity to ask any questions prior to enrolling in the study and then provided their consent to participate verbally. Participants were enrolled between January 2021 and February 2021. Participants were given a $10 gift card reimbursement for their time to participate. All study procedures were approved by the authors’ Institutional Review Board (IRB).
Data Collection
Both focus groups were conducted by a female facilitator trained in qualitative research methods. The groups lasted approximately 60 min each and were conducted in English. Participant demographic information was collected at the time of the group via REDCap, a secure, web-based software platform for research data collection.19,20 Focus groups were recorded, de-identified, and transcribed verbatim prior to analysis.
Data Analysis
Interview transcripts were coded by 2 members of the study team using thematic analysis. 21 Researchers (KC, WT) developed a codebook using an inductive and deductive process. A preliminary coding framework was developed according to the Behavioral Model of Healthcare Utilization for Vulnerable Populations 16 that emphasizes key areas directly impacting utilization of prevention and treatment among PWID including access, initiation, and adherence. According to the model, predisposing factors refer to social, systemic, and structural sources of vulnerability. Enabling factors refer to resources individuals, health systems, and communities possess that may facilitate uptake of PrEP and addiction services, specifically MOUD. Need-related factors refer to health status and health risks impacting health service utilization. Additional codes were added as they emerged from data analysis. Coders met bi-weekly to review coding agreement, discuss and resolve any discrepancies in coding, and assess whether additional codes were needed based on emergent themes from the data. A final codebook and qualitative matrix were created and shared with the study team to refine codes and interpret findings.
Results
Descriptive information of the 9 focus group participants is shown in Table 1. The mean age was 38 years (SD: 9, Range: 28-58), providers were mostly White (7/9), and female (5/9). Two thirds of focus group participants were trainee to early career physicians and one-third were mid- to late career physicians. Most had expertise in general internal medicine (6/9), and the group had varying years of experience working with PWID from 1 to 2 years to over 10 years of experience. Table 2 organizes each framework domain, illustrative quotes, and emergent themes that will be described in the following sections.
Descriptive Information of Focus Group Participants (N = 9).

Qualitative Matrix of Health Care Provider Perspectives of Factors Impacting Utilization of Integrated MOUD and PrEP Services Among PWID.
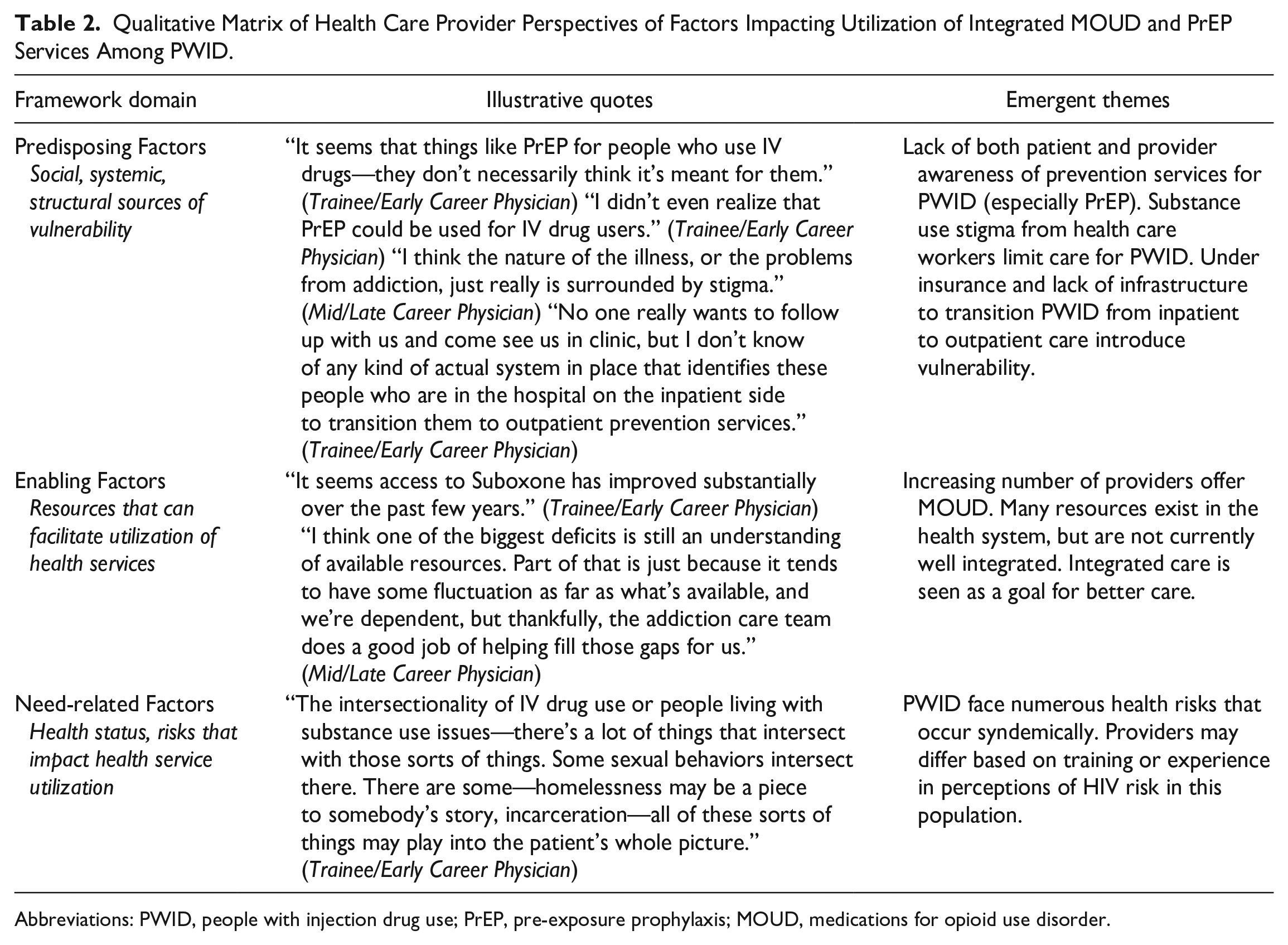
Abbreviations: PWID, people with injection drug use; PrEP, pre-exposure prophylaxis; MOUD, medications for opioid use disorder.
Predisposing Factors
Lack of access and awareness
A significant barrier identified specifically to PrEP utilization for HIV prevention for PWID was a lack of access and awareness. Several providers expressed neither patients nor clinicians view PWID as PrEP candidates: It seems that the marketing is largely PrEP is something to prevent you from getting HIV through a sexual transmission. I don’t know if the people who we’re approaching to possibly provide PrEP for—of course, access is an issue, but the awareness piece may come down to ‘I don’t feel like this is for me.’ (Trainee/Early Career Physician)
The marketing concerns that this provider alludes to have been compounded by an increase of direct-to-consumer advertisement of a different form of PrEP (tenofovir alafenamide-emtricitabine, TAF/FTC) only for sexual risk and excluding people who have receptive vaginal sex and PWID.
Another provider shared their knowledge gap in the indication for PrEP in an outpatient setting: I know we’ve had lectures on who should get PrEP and those sorts of things, and I feel like if we identified someone in clinic in primary care, we’d probably be comfortable doing it maybe—as long as we pulled up what we were supposed to do, but I don’t think we’ve gotten any training that can link that to persons who use IV drugs. (Trainee/Early Career Physician)
Overall, knowledge regarding who is eligible for PrEP is fragmented, subject to broader marketing, and lacking in application of clinic-based skills. A later career physician discussed their perspective on CME-based training that are often brief and lack in follow-up on usable skills, “It’s a lot of information, CME type of things, but not that I have used any of that besides increased awareness.” (Mid/Late Career Physician). Awareness is necessary but insufficient for providing care for PWID at risk for HIV.
Other providers agreed PrEP for PWID might be viewed as off-label use, causing confusion for providers who do not routinely prescribe PrEP. One provider stated, “At the end of the day, it really comes down to just taking the pill once a day, every day, but it’s the access and the awareness issues that I think are concerning.” (Trainee/Early Career Physician). Despite the simplicity and effectiveness of PrEP for PWID, this provider conveys the broader palpable hesitancy around offering PrEP—particularly for hospitalized PWID at discharge due to uncertainty around where these patients will follow-up.
Stigma
IDU-related stigma was discussed as another significant barrier to healthcare delivery among PWID. Participants provided numerous examples of stigma as a barrier to care for PWID and considered substance use stigma to be a de facto experience for PWID: “In my experience, if you’re in the hospital for any significant amount of time, and it’s known that you have addiction issues, there is gonna be stigma associated with that.” (Mid/Late Career Physician). Some providers discussed differing experiences of substance use stigma in inpatient settings compared to outpatient, infectious disease settings: I have anecdote after anecdote after anecdote of having a patient on your—on my medicine service or [Infectious Diseases] service where they inject drugs and nursing staff doesn’t necessarily respond well to their pain. They’re not quite thought of as honest or they can’t be trusted to leave the floor and things like that. There’s sometimes occasional comments that are made—not necessarily derogatory, per se, but clearly underhanded, related to their injection drug use. I think a lot of the training that we do on the outpatient side—for our clinic, at least, and how we recognize trauma or stigma and try to address that—that really is not—I don’t think that’s being done on the inpatient side. If it is, it’s not evident. (Trainee/Early Career Physician)
Substance use stigma is particularly problematic when it interferes with treatment recommendations for PWID as one participant noted: “you kinda do feel that what you’re recommending, which is from an Infectious Diseases perspective, of course—is best for the patient, but other services don’t agree because of their drug use. That’s a little bit tricky.” (Trainee/Early Career Physician).
Infrastructure
Providers agreed insurance barriers limit the potential for integrated HIV prevention and addiction care to reach patients. This is especially challenging for PrEP, which requires frequent laboratory testing for safety and HIV screening: It’s the visits and labs that are more challenging to have covered, and that’s something that we can’t really get around. More affordable options like the health department exists. I know there are certain clinics that are meant for underinsured or uninsured populations, but even still, labs can often be a struggle to get, and things like that. Yeah. We haven’t broken that barrier yet, and that’s just a really hard one to get around because it’s a little bit out of our hands. (Trainee/Early Career Physician)
Finally, the lack of infrastructure to transition PWID from inpatient to outpatient care is also limiting. Providers agreed the healthcare system is not set up to transition PWID to the outpatient treatment and prevention services they need.
Enabling Factors
Participants agreed greater availability of prescribers who can provide MOUD for addiction care in healthcare systems allows for greater access to care. One provider commented on improvements in access to at least one form of MOUD for addiction care, “Tons of people are [Suboxone] waivered, but there’s almost no access to methadone.” (Trainee/Early Career Physician). Providers discussed some patients prefer methadone over other MOUD, both availability of and regulations surrounding opioid treatment programs (ie, methadone clinics) limit its use.
Participants also agreed the health system has numerous resources available, but they are fragmented—difficult to find and access. Providers shared they depend on interprofessional teams including addiction care teams and social workers to advise them on available resources. Providers tended to agree an integrated, interdisciplinary approach is needed.
I think it depends on where you’re practicing. If you’re in a place that has really robust social work and an infrastructure that supports multi-modal care, then it’s probably easier. The places where I work—most of them are interdisciplinary and provide things like—you go to one visit, and you—at the gender clinic, we will do surgical care, hormones, and PrEP in one visit, but the patient has a team. If you’re in that kind of space, I think it’s easier. (Trainee/Early Career Physician)
Several mid-later career providers also highlighted the importance of addiction medicine-focused teams they use for consultation in hospital settings including social workers and nurses who have up-to-date resources and training to address the complex needs of PWID. Providers expressed they rely on support from other subspecialties, including addiction medicine, infectious diseases, nursing, and social work when connecting PWID to relevant services.
Need-Related Factors
Participants perceived many health risks for PWID including overdose, mental health comorbidities, and infections. Importantly, addiction, medical, and social complications occur together as one participant noted: “If you look at it almost like an ecological level of where they are—there’s the person who injects drugs themselves, and then the context of—well, their addiction problems or their infection problems or whatever you wanna think about it. They all coexist.” (Trainee/Early Career Physician). Patients need whole-person approaches to their care to address treatment and prevention needs.
Providers expressed concern PWID are at heightened risk for incomplete care: “persons who inject drugs are at higher risk of leaving AMA [against medical advice] and not getting their endocarditis fixed or maybe it was a small infection and they left and it gets more complicated.” (Trainee/Early Career Physician). Participants viewed these experiences as relevant in shaping provider attitudes about care to PWID, and can also inform decisions about how PWID will access services.
Early career providers agreed HIV was a significant risk for PWID: “Tremendous risk. Yeah, tremendous risk. If we actually think about how effectively HIV is spread, injection drug use is a higher risk than sexual transmission. It is a very high-risk factor.” (Trainee/Early Career Physician). Meanwhile, providers in the second focus group of later career physicians focused less on HIV as a risk, and more on HCV: The main virus that we see is hepatitis C, way more than HIV or any other. I don’t really personally think about seeing a lot of HIV contracted from injection drug use in the hospital. It’s not something I’ve experienced. Whenever we screen these people for hep C, it’s a high number for hep C, definitely. (Mid/Late Career Physician)
This dichotomy between the early career and mid to later career groups may indicate providers with more contemporary medical training are more likely to perceive HIV risk among PWID and prescribe PrEP for HIV prevention.
Discussion
As overdose and infectious diseases risks intensify with the Opioid Epidemic, evidence-based interventions—specifically, MOUD and PrEP—are greatly needed to mitigate these risks. Through a framework adapted from the Behavioral Model of Healthcare Utilization for Vulnerable Populations, 16 this qualitative study captures the challenges and opportunities, as experienced by frontline providers, around incorporating these interventions into an academic medical setting in the U.S. South. Clinicians with varying experience revealed their own hesitancies and knowledge gaps around HIV risk and treatment and prevention options, and also reflected on their patients’ obstacles to these services, including awareness, stigma, and access (eg, insurance). Based on our findings, we identified a need to address 3 key areas including education, clinical infrastructure, and policy for further research and program development around an integrated addiction and HIV prevention strategy for PWID.
Results of this study emphasize the persisting educational barriers slowing implementation of treatment and prevention services for PWID. Unique knowledge gaps influencing PrEP uptake for PWID were emphasized. Compounding their own inexperience in prescribing PrEP for PWID, providers raised concern their patients injecting drugs “don’t feel like this [ie, PrEP] is for me” and PrEP marketing implicitly reinforces this notion. These missed opportunities in patient education and engagement widen an already unacceptable gap to PrEP in the South where its uptake falls far short of the scope of the regional HIV epidemic—with the South accounting for only 30% of the U.S.’s PrEP use despite bearing over half of new HIV diagnoses. 22 Few PrEP education tools or public health campaigns exist targeting PWID, related to opioid use, HIV prevention, or both. Provider perspectives revealed additional educational gaps in MOUD training and mentoring.
Stigma is a persistent and insidious barrier to care for PWID observed by healthcare providers in inpatient and outpatient settings. Increasing provider education about stigma and bias as well as integrating providers as drivers of stigma reduction efforts and community engagement are needed to address intersecting substance use, HIV, and other stigmas occurring in the healthcare setting. 23 Healthcare stigma interventions must be designed for all levels of healthcare staff to reduce the perpetuation of stigma and improve quality of care and retention in treatment and prevention services.
Integration of addiction and HIV preventive care will require a corresponding increase in clinical infrastructure. In this study, providers identified multidisciplinary care teams and inpatient-to-outpatient transitions as essential features for building this infrastructure. Multidisciplinary teams including case management and mental health services enhance access to, and retention in, HIV primary care. 24 Similar teams targeting hospitalized patients and their transition to outpatient HIV care have also accelerated patient outcomes along the HIV care cascade. 25 Lessons from HIV treatment models and transition teams are applicable to HIV prevention too. Just as hospitalization has served as a “reachable moment” to identify at-risk patients with OUD and link them to community care, 26 the inpatient-to-outpatient transition for PWID is naturally positioned to incorporate addiction care and HIV prevention initiation and connection to follow-up integrated care. These changes will require a robust inpatient team and close collaboration with community partners who are able to provide integrated addiction care and HIV prevention.17,27
No matter how well designed the clinical infrastructure, PWID and their providers face unique challenges requiring policy changes. In this study, providers articulated the lack of insurance coverage looms as a threat to integrated addiction care and HIV prevention—not only jeopardizing MOUD and PrEP initiation but also interfering with standard-of-care monitoring once started (eg, checking renal function and performing routine STI testing for patients on PrEP). Medicaid expansion could most swiftly address this insurance disparity, and with it, states could benefit from the increased PrEP utilization 28 and decreased opioid overdose deaths expansion states have already experienced. 29 Despite a saturation of counties with a high need for addiction treatment services, these same counties often have little to no capacity to provide treatment with buprenorphine. 30 The aspirational policy would be legalization of harm reduction services, specifically syringe service programs, wherein HIV prevention and treatment, HCV treatment, and addiction treatment is provided together. However, syringe service programs remain illegal in much of the U.S. South leaving a missed opportunity and touch point for PWID.
The results of this study should be interpreted in light of some limitations. Healthcare providers were recruited for this study at a peak in the ongoing COVID-19 pandemic and were completed via synchronous focus groups online using secure video conferencing software. This approach to qualitative data collection was used well before the COVID pandemic and evidenced data quality comparable to in-person focus groups, 31 and have gained additional evidence for their feasibility and acceptability through the pandemic as social distancing measures necessitated online data collection.32,33 The second focus group of mid- and later career physicians was small, potentially limiting discovery of new themes from this group. Data saturation was not necessarily the goal of this research as our team engages in a process of constructing knowledge around a specific and complex problem of delivering integrated treatment and prevention services in healthcare settings. 34 Few new themes emerged in the second group and the research team agreed data were adequate for describing the specific issue at hand. Consistent with the goal of qualitative research, we aimed to describe in-depth the barriers and facilitators to evidence-based treatment and prevention services for PWID perceived by healthcare providers. This study does not report on the direct experience of patients. This study focuses on OUD and does not account for PWID with other non-medical use such as methamphetamines, for which there is no effective pharmacotherapy. Additional research is needed to understand linkage to care issues from the perspectives of PWID and other stakeholders (eg, community workers, advocates, policy makers).
In conclusion, this study examined provider perspectives on the challenges and opportunities for providing integrated addiction and HIV prevention for PWID. Healthcare providers included in this study were employed in an academic medical center in the U.S. South with experience serving PWID in inpatient or outpatient settings. While the issues outlined through this qualitative analysis are complex, they provide concrete examples of barriers experienced by providers when deciding on treatment plans for PWID. Providers identified action items to enable integrated, stigma-free, evidence-based care from education to multidisciplinary staffing to health insurance access and harm reduction policy. The needs are great and may be overwhelming for healthcare systems treating PWID. A first step may include taking stock of existing educational and staffing resources around addiction care and HIV prevention to create an interdisciplinary team of champions willing to work toward change for this vulnerable group. Future implementation science work may address the unique contextual factors affecting PWID and those who care for them to enact change at multiple levels.
Footnotes
Acknowledgements
We thank Yogeinis Maldonado for assistance with manuscript preparation. We also thank the participants for their time and engagement.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the UAB Center for AIDS Research Administrative Supplement Award (P30 AI027767 Supplement). KBC receives funding from the National Heart, Lung, and Blood Institute (NHLBI) under award number K23 HL156758-01A1. EE receives funding from the National Institute of Mental Health (R01 MH124633-01) and Substance Abuse and Mental Health Services Administration (1H79SP082270-01). The content is solely the responsibility of the authors and does not necessarily represent the views of the National Institutes of Health.