
Abstract
Objectives:
To examine Influenza and COVID-19 vaccine concerns and uptake among adult patients in a Southern safety-net health system.
Methods:
Trained research assistants conducted a structured telephone interview from April to October 2021. Of 118 participants, mean age was 57.7 years, 63.6% were female, 55.1% were Black, 42.4% white, and 54.2% reported rural residence.
Results:
Among participants, 44.9% had received the influenza vaccine during the 2020 to 2021 season, and 66.1% had received the COVID-19 vaccine. Participants who received the influenza vaccine were more likely to report getting a COVID-19 vaccine compared to those who reported not getting a flu vaccine (81.1% vs 53.8%, P = .002). Black adults were significantly less likely than white adults (29.2% vs 46.0%, P = .048) and bordering on significance, males less likely than females (27.9% vs 41.3%, P = .054) to have reported receiving both vaccines. Of note, 25.4% of participants did not get either vaccine. The most common reasons for not getting the influenza vaccine were not being concerned about getting the flu (13.8%) and belief the vaccine gave them the flu (12.3%). The primary reasons for not getting a COVID-19 vaccine were concern about vaccine safety (22.5%), concern about side effects (20.0%), and belief they were not going to get sick (20.0%).
Conclusions:
These findings could help direct regional vaccine messaging and clinical communication to improve vaccine uptake among underserved populations.
Introduction
Experts warned the convergence of coronavirus-19 and seasonal influenza would result in considerable morbidity and mortality. 1 As of September 2, 2022, over 1.05 million people have died of COVID-19 in the U.S and in the previous influenza season, over 22,000 died of influenza between 2019 and 2020.2,3 Vaccines are our most powerful tool in reducing the risk of serious illness, hospitalization, and death from both of these viruses.4-6 As the world embraces the high likelihood that SARS-CoV-2 will become a second seasonal respiratory pathogen with epidemic potential, effective communication about influenza and COVID-19 vaccines will become increasingly important concerns. 7 While the scientific details of viral evolution (eg, antigenic shift and drift, emergence of variants, and natural selection) may not be germane for all patients, the development of trust built on long-term relationships with health care providers is critical to overcoming patient concerns about vaccination that lead to disparate health outcomes. Trust and acceptance of COVID-19 and influenza vaccines are critical for mitigating health disparities and improving population health.7-9
The Centers for Disease Control and Prevention (CDC) recommends adults stay up to date with both COVID-19 and influenza vaccines. However, unvaccinated people, especially those over 65 years of age or with significant comorbidities (eg, immune compromise, chronic kidney, heart or liver disease, obesity, diabetes or severe asthma, etc.), remain at high risk of serious infection, and/or death due to SARS-CoV-2 and influenza.8,9
The World Health Organization (WHO) considers vaccine hesitancy to be a global health threat. 10 The WHO has defined vaccine hesitancy as behavior influenced by a number of factors including lack of trust in the vaccine or the provider, complacency (not perceiving a need for the vaccine or not valuing the vaccine) or lack convenient access. 10 Major factors associated with vaccine hesitancy include perceptions of risk, safety, efficacy, and trust, as well as social demographic characteristics11-13 Recent U.S. studies identified a wide variation in vaccination uptake by region and race and found vaccine-hesitant individuals are a heterogeneous group who have varying degrees of indecision about specific vaccines or vaccination in general.6,12,14,15
As of September 2, 2022, the CDC 2 reported 77.3% of US adults (≥18 years of age) were fully vaccinated with the primary series and 45.4% received a flu vaccination in the 2020 to 2021 season. 2 However, racial and rural disparities persist. Vaccine hesitancy for all routinely recommended vaccines has been historically higher in rural than urban areas where residents tend to be older, uninsured, have limited access to healthcare, and are more likely to face transportation barriers than urban counterparts.16-20 Currently, rural residents are less likely than urban residents to receive the both vaccines and COVID-19 vaccine disparities have increased twofold in the last year.15,17 Black adults are also less likely to be up to date with influenza vaccination compared to whites (40.4% vs 55.5%) 21 however racial disparities for COVID-19 vaccination has narrowed and the CDC recently reported Blacks and whites have similar rates. 22
Immunization for both COVID-19 and influenza also remains uneven across the country. Rhode Island ranks first among states, with 85% fully vaccinated for COVID and 60.9% for influenza. Louisiana (LA) persists in ranking among the bottom 5 states with 63.0% fully vaccinated for COVID-19 23 and 42.0% for influenza. Disparities within the state also exist, with vaccine rates for both virus lower in rural areas. COVID-19 vaccination rates in Louisiana are now higher among Black adults than White adults, but influenza vaccination remains lower for Black adults. The purpose of this study was to determine racial, sex, and rural differences in influenza and COVID-19 vaccination and to identify concerns and socio-demographic factors associated with vaccine acceptance among a wide age range of adults in Northern Louisiana especially those experiencing high rates of health disparities. The goal was to aid in the development of effective strategies to enhance public health and clinical communication about vaccines in populations subject to significant health disparities.
Methods
We conducted a telephone survey regarding concerns and uptake of influenza and COVID-19 vaccines among a convenience sample of patients with a recent physician visit in a north Louisiana safety-net health system between April and October 2021. Trained public health students and clinical research assistants called adult patients of Ochsner-LSU Health Shreveport (OLHS) who had a recent provider visit and asked if they would be willing to participate in a brief 10-min structured telephone survey about COVID-19. Participant responses were entered into a Redcap web-based survey database. OLHS serves predominately low-income patients; 75% have Medicaid and or Medicare and 12% have private insurance. This quality improvement project was approved by the LSU Health Shreveport IRB. Participants provided informed consent prior to participation and were not paid for their time.
Participants were ambulatory care patients who had participated in, or their child had at least 1 visit with a provider at a non-urgent care clinic of OLHS during the study period. Inclusion criteria included age 18 or over and English speaking.
The 10-item survey was designed to assess participants’ concerns and uptake regarding influenza and COVID-19 vaccines. The survey was modified from a telephone survey developed by 1 of the authors, The Chicago COVID-19 comorbidities survey.24-26 The current survey added questions related to the influenza vaccine and participants’ intention to have their children vaccinated against COVID-19. Five items assessed participant characteristics including age, race, gender, employment status, and location of residence (urban or rural).
Influenza vaccine uptake was assessed by asking if they had received the influenza vaccine in 2021. If not, participants were asked to choose all options that applied from 13 options to indicate why they chose not to receive the influenza vaccine. Answers included allergic to the vaccine, don’t like needles, not concerned about getting influenza, don’t think the vaccine works, got it before and believed it gave me the flu, concerned about side effects from the vaccine, not trusting the vaccine is safe, not believing the influenza is as bad as some people say it is, not wanting to pay for it, against my faith/religion, and didn’t want to go out because of COVID-19.
COVID-19 vaccine uptake was assessed by asking if participants had received a COVID-19 vaccine. Participants who had not received a COVID-19 vaccine were asked to indicate the reason(s) for not receiving a COVID-19 vaccine from a list of 13 options from which they could select all that applied (allergic to vaccine, concern about getting really sick, concerned about vaccine side effect(s), against my religion, want to wait, etc.) Participants who had children were asked about their willingness to get their children vaccinated as soon as the vaccine became available. Answers were scored on a 10-point Likert scale with one being unwilling to 10 being very willing.
For analysis purposes, demographic characteristics were defined as follows: gender (male and female), race (Black, White), age (18-29, 30-44, 45-64, and 65+), location (urban and rural), and employment status (working for pay, not working for pay). Statistical analysis was based on within-group proportions and Chi-Square tests were used to determine statistically significant differences between groups.
Results
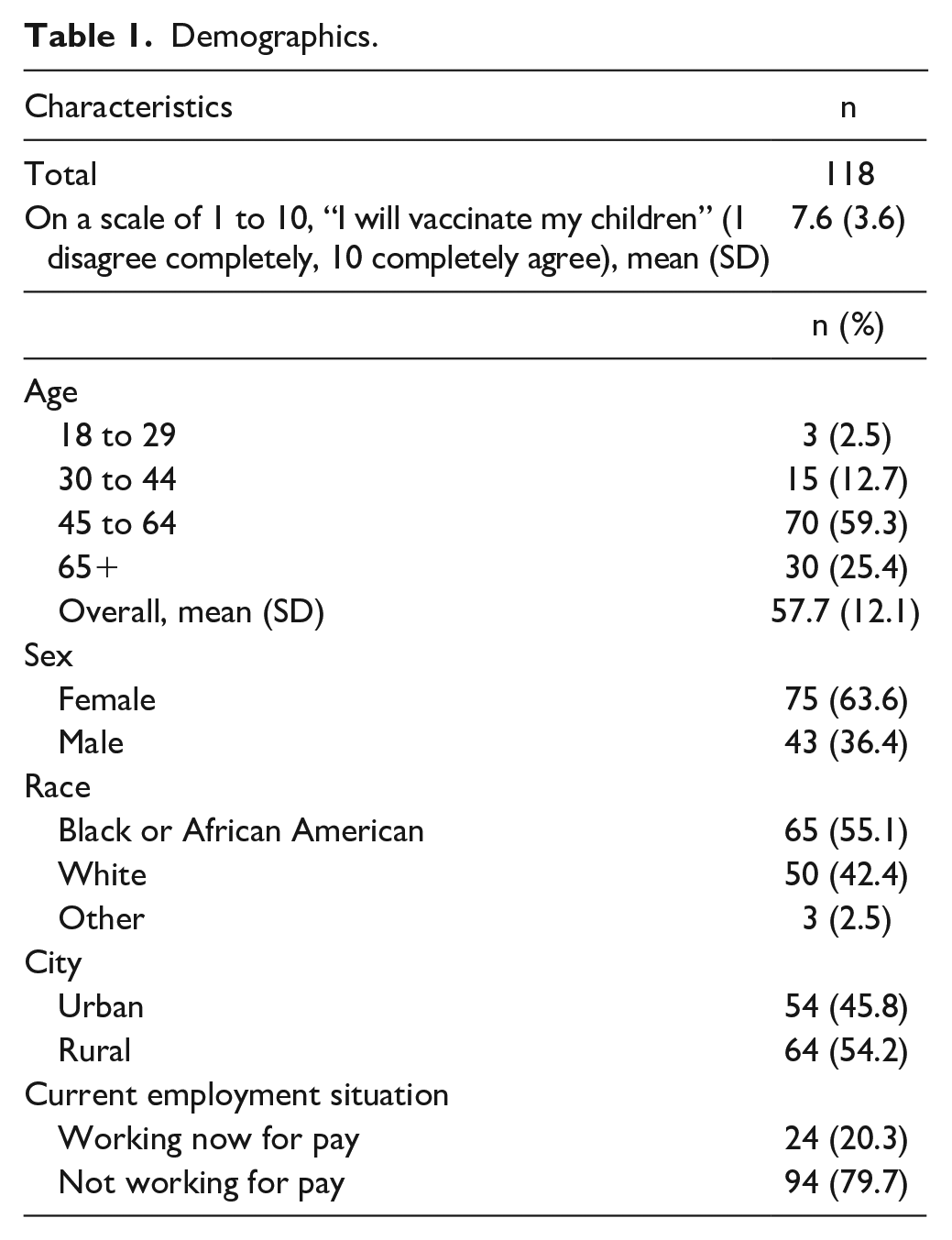
Of the 210 participants receiving care in a specialty or primary care clinic at OLHS, 118 (56.2%) completed the survey. Table 1 summarizes the characteristics of participants; the mean age was 57.7 years, the majority were female (63.6%), 55.1% were Black adults, 42.4% were white, and 54.2% reported living in rural areas. Of the participants who completed the survey, 79.7% were not working for pay.
Demographics.
Among participants, 44.9% reported receiving the influenza vaccine in the most recent influenza season (2020-2021) and 66.1% reported receiving a COVID-19 vaccine. There was no difference in influenza or COVID-19 vaccination uptake by race, sex, or place of residence (Table 2). Participants who reported receiving the influenza vaccine were more likely to report getting a COVID-19 vaccine compared to those reporting not getting a flu vaccine (81.1% vs 53.8%, P = .002). Approximately one-third (36.4%) reported receiving both the COVID-19 and Influenza vaccines. No differences were found by location, but Black adults were significantly less likely than white adults (29.2% vs 46.0%, P = .048) and bordering on significance, males less likely than females (27.9% vs 41.3%, P = .054) to have reported receiving both vaccines (Table 2). Of note, 25.4% of participants did not get either vaccine.
Experiences by Race, Gender, and Place of Residence.

p < .05.
Participants with children reported a strong willingness to have their children vaccinated against COVID-19, when the vaccine became available to them, with a mean score of 7.6 on a 10-point scale. Participants who reported not receiving the COVID-19 vaccine were significantly less likely to indicate a willingness to vaccinate their children for COVID-19 than those who got the vaccine (means respectively (4.0 vs 9.2, P < .001). Those who reported not getting the influenza vaccination were also significantly less likely to indicate a willingness to vaccinate their children for COVID-19 than those who reported receiving the influenza vaccine (7.0 vs 8.3, P < .001).
The most common concerns about the influenza vaccine were not being concerned about getting the flu (13.8%) and believing the vaccine gave them the flu (12.3%). The most common reasons for not receiving a COVID-19 vaccine were concern about vaccine safety (22.5%), side effects (20.0%), and the participant did not believe they were going to get sick from COVID-19 (20.0%).
Discussion
Regional vaccine concerns and uptake must continue to be assessed as health systems and wider society prepare for the likelihood of annual co-epidemics of COVID-19 and influenza. In our survey with predominantly low-income participants in a Southern safety-net health system, 1 in 4 had received neither vaccine. Over half had not received the influenza vaccine this season and approximately 1 in 3 had not received a COVID-19 vaccine. This level of immunization falls short of Healthy People 2030 vaccination goals and may threaten over-burdened regional health care systems. 27 Addressing barriers to vaccination is critical to achieving vaccine equity, reducing disparities, and decreasing COVID and flu related illness and death in the US. 28
Despite widespread public health campaigns, disparities in COVID-19 and influenza vaccination uptake continue to exist. 6 The National Health Interview Survey found influenza vaccine uptake was lower among males, Black adults, and rural residents. 29 A large online survey of the COVID-19 vaccine found COVID-19 vaccine hesitancy was higher among Black adults, rural residents, females, and those having children at home. 12 Vaccine resistance and hesitancy are complex and driven by multiple factors. In a national county-level study comparing COVID-19 vaccination, Tolbert et al. 30 found counties with larger shares of racial/ethnic minorities and higher rates of poverty and uninsured populations have lower vaccination rates. In another county-level study, Sun and Monnat 31 found lower levels of educational attainment and more conservative political ideologies in rural areas may play important roles. 32 Rural residents are on average poorer, have lower rates of insurance coverage, have less robust health care infrastructure, and must travel further distances to venues where vaccines are administered. 33 Availability is unlikely to be the main explanation for differences in vaccination rates, but access factors may play some role. 31
In our small regional study that included both COVID-19 and influenza vaccination, we found no difference in influenza or COVID-19 vaccine uptake by sex, race, or rural residence. Black adults were less likely than white adults, and men were less likely than women to have received both vaccines.
Vaccine hesitancy is also related to public perception of the risks, effectiveness, and safety of the vaccines. 34 Nationally, as in our study, uptake of the annual influenza immunization is low compared to COVID-19.2,35,36 In our study, more than 1 in 10 were not concerned about the risk of getting the flu and had the misconception that a previous flu shot had given them the flu. More than 1 in 5 had COVID-19 vaccine concerns related to safety, side effects, and the belief they would not get sick from the virus. This indicates public health messaging and provider communication promoting both vaccines need to include the risks of getting the virus and the safety and benefits of the vaccines. Messages may need to be specifically tailored to address the vaccine hesitancy of Black adults and males.
Pediatric vaccination is an important component of mitigating a dual epidemic of influenza and COVID-19. 1 Vaccinating children is necessary, not only to prevent this illness in children epidemic, but also to establish herd immunity within the general population. 37 In the United States, only approximately 60% of children receive a seasonal influenza vaccination annually. 35 The COVID-19 pandemic may encourage parents to be more likely to have their children receive the influenza vaccine.38,39 However, a national online survey of parents found the COVID-19 pandemic alone did not encourage the uptake of pediatric seasonal influenza vaccination; rather it may have exacerbated polarity in vaccination uptake. 38 In our study, participants with children reported they would likely get their children vaccinated when COVID-19 vaccines became available for them. Yet, unsurprisingly, parents who did not get the influenza or COVID-19 vaccine reported being less willing to have their children vaccinated than those who had received either of the vaccines.
Given the unpredictable future of COVID-19, the emergence of new variants, the potentially waning population immunity, and the threat of a twin epidemic there is a continuing need for clear, trustworthy public health messaging and clinical communication about the health risks posed by both viruses, the safety of the vaccines and the benefits of vaccination. Additionally, our findings confirm the need for periodic regional studies to help inform the targeting of public health messages as well as the importance of providers in our region providing accurate up-to-date, trustworthy information about the viruses and educating patients about the benefits of both vaccines for themselves and their families.
Limitations
Limitations of this study: (1) It was a small convenience sample with predominantly low-income patients at 1 health system; (2) We did not assess income or education; (3) the small sample did not allow determination of specific concerns by participant characteristics; (4) the survey was conducted in English only; and (5) vaccination information was not verified for each participant.
Conclusions
This study provides a snapshot of low-income Louisiana patients’ influenza and COVID-19 vaccine uptake and concerns. The findings are important in helping inform ongoing efforts to increase effective clinical and public health communication about vaccines. Disparities in public perceptions and uptake of both viruses and vaccines continue to evolve, and regional research over time is needed on vaccine acceptance among a wide range of adults to understand the complex factors that promote and mitigate vaccine hesitancy.
Footnotes
Author Contributions
Drs. Arnold, Davis, and Wolf contributed to conceptualization; Methodology, Drs. Arnold and Davis; Validation/Formal Analysis, Dr. Arnold; Investigation, Drs. Arnold and Davis.; Resources, Drs. Arnold and Davis; Data Curation, Drs. Arnold, Davis; Writing—Original Draft Preparation, Drs. Arnold and Davis; Writing—Review & Editing, all authors; Visualization, Drs. Arnold and Davis; Supervision, Drs. Arnold and Davis; Project Administration, Drs. Arnold and Davis; Funding Acquisition, Drs. Arnold and Davis.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Drs. Davis and Arnold are supported by 2 U54 GM10490, The National Institute of General Medical Sciences of the National Institutes of Health, which funds the Louisiana Clinical and Translational Sciences Center. The content is solely the responsibility of the authors and does not necessarily represent the office views of the NIH. This research was funded by the Department of Medicine, LSU Health Shreveport.
Institutional Review Board Statement
The study was approved by the Institutional Review Board of LSU Health Shreveport (STUDY00001447 on 4/14/2020).