
Abstract
Introduction/Objectives:
Patient activation describes the knowledge, skills, and confidence that allow patients to actively engage in managing their health. Prior studies have found a strong relationship between patient activation and clinical outcomes, costs of care, and patient experience. Patients who are obese or overweight may be less engaged than normal weight patients due to lower confidence or stigma associated with their weight. The objective of this study is to examine whether weight status is associated with patient activation and its sub-domains (confidence, communication, information-seeking behavior).
Methods:
This repeated cross-sectional study of the 2011 to 2013 Medicare Current Beneficiary Survey (MCBS) included a nationally representative sample of 13,721 Medicare beneficiaries. Weight categories (normal, overweight, obese) were based on body mass index. Patient activation (high, medium, low) was based on responses to the MCBS Patient Activation Supplement.
Results:
We found no differences in overall patient activation by weight categories. However, compared to those with normal weight, people with obesity had a higher relative risk (RRR 1.24; CI 1.09-1.42) of “low” rather than “high” confidence. Respondents with obesity had a lower relative risk (RRR 0.82; CI 0.73-0.92) of “low” rather than “high” ratings of communication with their doctor.
Discussion and Conclusions:
Though patients with obesity may be less confident in their ability to manage their health, they are more likely to view their communication with physicians as conducive to self-care management. Given the high receptivity among patients with obesity toward physician communication, physicians may be uniquely situated to guide and support patients in gaining the confidence they need to reach weight loss goals.
Introduction
Patient activation is a broad concept that describes the knowledge, skills, and confidence a person has in managing their own health. 1 Prior studies have found a strong relationship between patient activation and clinical outcomes, costs of care, and the patient experience of care.2-7 For example, increased patient activation has been associated with lower total costs of care, 8 greater health-related quality of life, 5 and improved self-management, 6 and low levels of patient-activation have been significantly associated with increased anxiety and higher information needs. 9 These relationships have been demonstrated across a range of different populations and health conditions.5,9,10
Patient activation may be especially salient for patients with obesity. Activated patients are more likely to engage in health behaviors that support successful weight management such as consuming healthy foods, partaking in regular activity, and following a doctor’s advice.4,11 By definition, activated patients understand their role in the care process and feel capable of fulfilling that role. Hence, patients who are activated may be better equipped to manage their weight more effectively.
Yet sustaining patient engagement in weight loss efforts has remained difficult for both patients and providers. 12 Such low engagement may be partly due to the widespread stigma associated with obesity, which is pervasive even within healthcare settings.13-16 Numerous studies have found that doctors, nurses, and other healthcare providers hold negative opinions about persons with obesity. 17 For example, physicians have been found to have less respect for patients with obesity18,19 to be more likely to perceive patients with obesity as non-adherent to medications, 20 and to spend less time building rapport with patients with obesity. 21 Patients with obesity meanwhile report feeling disrespected by providers and perceive that they will not be taken seriously because of their weight.18,22
These perceptions and experiences may work in interconnected ways to reduce patient activation among patients with obesity. First, individuals with obesity who internalize weight-biased attitudes may not feel confident in their ability to manage their health. Second, patients who feel judged may avoid clinical care and not seek out necessary information from their providers. Finally, perceptions of stigma may impair communication during patient-provider interactions.
In this paper, we explore the relationship between a patient’s weight status and patient activation. Specifically, we examine the associations between obesity and the sub-domains of patient activation including confidence, communication, and information seeking behavior. We hypothesize that patients with obesity are less activated than patients with normal weight.
Methods
Data and Study Population
This study uses data from the 2011 to 2013 Medicare Current Beneficiary Survey (MCBS), an in-person, nationally-representative survey of Medicare beneficiaries administered by the Centers for Medicare and Medicaid Services (CMS). 23 The MCBS has a rotating panel sample design where patients are sampled for up to 4 years. We included only the first year’s response for beneficiaries who responded over multiple years. 24 We constructed 2 analytic samples for the study: all respondents, and utilizers only (described below).
For both samples, we excluded institutionalized respondents and those responding via proxies because they were not asked to respond to the Patient Activation Supplement (see measures below). Because the data are primarily around Medicare beneficiaries, we also excluded those who were under 65. Finally, we excluded those who did not respond to the patient activation survey or responded to fewer than half of the survey items, did not have BMI information, or were underweight. This process resulted in the first sample (all respondents), which had 13,721 unique patients.
The second sample (utilizers only) added an additional restriction to exclude those who did not have any inpatient or outpatient claims during the survey year. We applied this restriction because the patient activation supplement asks patients questions about interactions with providers (Supplemental Table 1). We believe these questions would be best addressed by those with at least 1 recent medical encounter. This restriction also allowed us to control for claims-based comorbidities and account for potentially higher clinical complexity among patients with obesity, as captured by medical claims. 29 This process resulted in 6996 unique patients. Supplemental Figure 1 depicts the inclusion criteria and for both analytic samples.
Measures
Patient Activation: Patient Activation was derived from responses to the 2011 to 2013 Patient Activation Supplement, the most recent and up-to-date version available. 25 The 16 items in the Patient Activation Supplement are designed to capture 3 domains of patient activation: confidence, communication, and information seeking. The questions within each domain are listed in Supplemental Table 1.
We used a validated approach to assigning levels for overall patient activation and the 3 domains.26,27 Weighted composite scores were constructed by dividing the sum of scores for the relevant questions and dividing that sum by the number of non-missing items. Composite scores below the mean minus one-half of the standard deviation were designated “low,” those above the mean plus one-half of the standard deviation were assigned “high,” while the rest were designated “medium.”
Weight categories: Weight categories were based on self-reported body mass index (BMI) derived from height and weight and defined according to standard guidelines: normal weight (BMI 18.5-24.9), overweight (BMI 25.0-29.9), and obese (BMI ≥ 30).
Other health and socio-demographic factors: Sicker patients may feel less capable of managing their health. Therefore, we included measures of self-rated health (compared to others of the same age, excellent/very good/fair/poor), utilization (number of outpatient visits), and comorbidities. For the first sample (all respondents), comorbidities were measured using the self-reported number of physician-diagnosed comorbid conditions. 28 For the second sample (utilizers only), we calculated Elixhauser comorbidity scores based on all outpatient and inpatient claims for the year. We also controlled for 6 self-reported socio-demographic factors: age (65-74/75-84/≥85); gender; race (white/African-American/other); marital status (not married/currently married); household income (under $25 000/$25 000 or more); and education level (less than high school/high school/some college/bachelor’s or higher).
Analysis
We used multinomial logistic regression models to evaluate the relationship between weight status and patient activation for each sample. We selected “high activation” as the base category and report the relative risk ratio (RRR), the exponentiated regression coefficient. Analyses were conducted for overall activation, and activation in the 3 domains. All models controlled for health and socio-demographic factors. We also conducted ordered logistic regression models to check the robustness of our findings to alternative specifications. 29
We used cross-sectional survey weights and the balanced repeated replication (BRR) method for variance estimation to account for the stratified sampling design of the survey and adjustments for survey nonresponse. This statistical approach yields an estimate that essentially reflects a moving average of nationally representative, year-specific estimates.30,31 Because covariate non-response was minimal (ranging between 0.0% and 0.6%), we conducted complete case analyses for multivariate results. All analyses were conducted using Stata SE 15.0. This study of de-identified data was exempt from IRB review.
Results
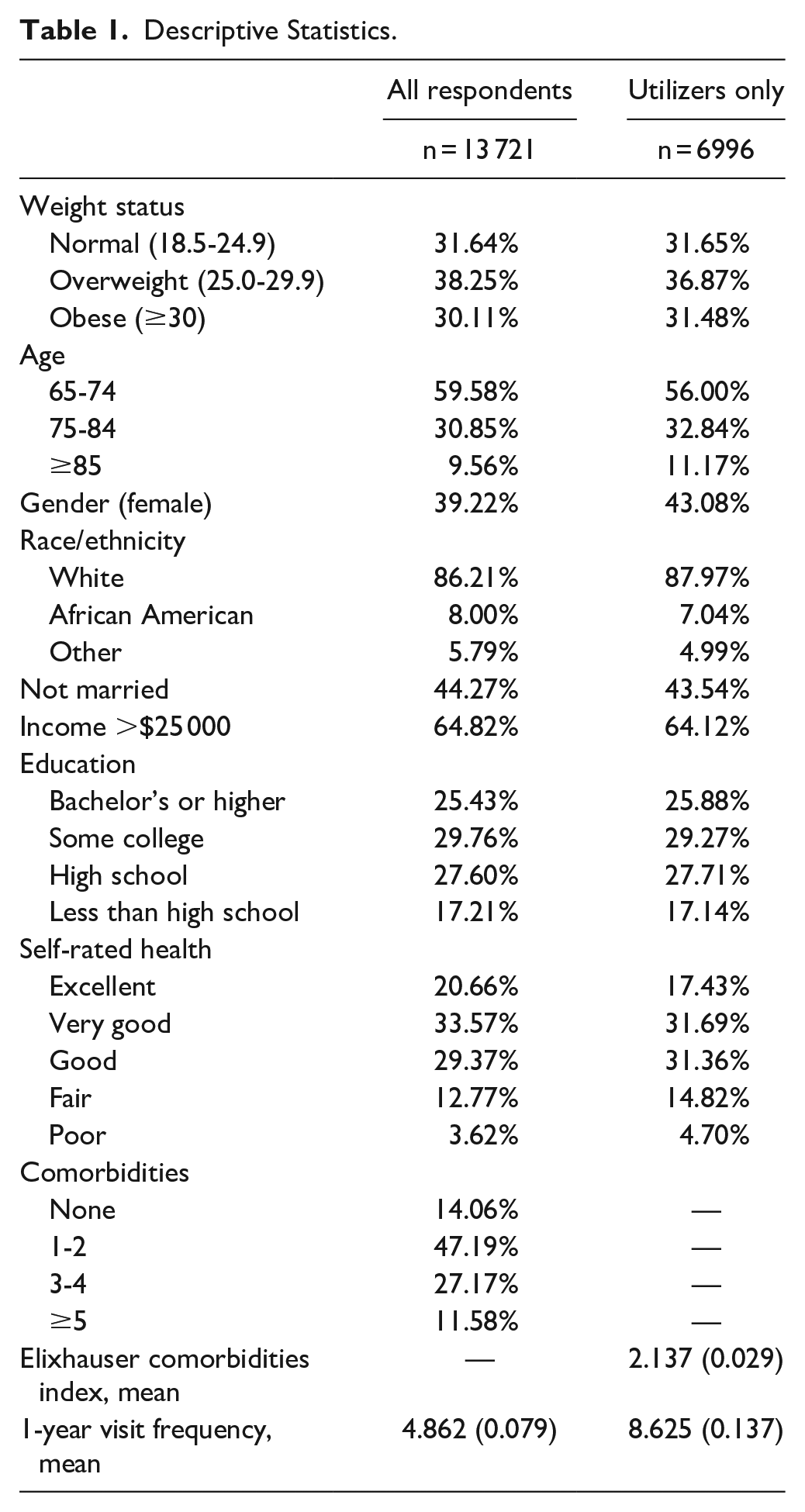
Table 1 provides descriptive statistics for the 2 analytic samples. The prevalence of overweight and obesity was similar across both samples, and the distribution of weight categories was generally consistent with prior estimates of the Medicare population. 29 We found no difference in overall patient activation by weight category in multinomial logit models in both analytic samples (all respondents and utilizers only). Overall patient activation was similar across all weight categories in both analytic samples (Table 2). However, difference emerged by weight status when analyzing the patient activation sub-domains. The biggest difference by weight category was found in the confidence domain. Compared to respondents with normal weight, patients with obesity were significantly more likely to have “low” or “medium” confidence rather than “high” confidence (All respondents: RRR 1.24 low; RRR 1.41 medium; Utilizers: RRR 1.27 low; RRR 1.52 medium). This significant negative association between weight status and confidence was also found in sensitivity analysis using ordered logistic models (available upon request).
Descriptive Statistics.

The referent category in the multinomial dependent variable is high activation.
P < .05.
The referent category for weight is normal (BMI 18.5-25.0).
Models control for age, gender, race, marital status, income, education, self-rated health, and comorbidities.
Analyses of the communication domain found that patients with obesity had a lower risk (All respondents: RRR 0.82; Utilizers: RRR 0.82) of “low” rather than “high” ratings of communication with doctors. Individuals who were overweight were also less likely to rate communication as low (vs high) compared to peers with normal weight (All Respondents: RRR 0.89; Utilizers: RRR 0.87), though the relationship was not significant for the utilizers only sample. Ordered logistic regression models also showed a consistently positive relationship between weight status and communication, suggesting that people with obesity are more likely than people with normal weight to give a high rating for patient-physician communication.
Other socio-demographic health variables including age, income, education, and self-rated health were found to be highly significant, such that older, 32 poorer, 33 less educated, 34 and those reporting poorer health compared to their peers were less likely to be activated overall (Table 3). 35 Sensitivity analyses pooling all responses, that is, including multiple responses for beneficiaries included in multiple years of the survey, did not meaningfully change this pattern.
Multinomial Logistic Regression of Overall Patient Activation on Patient Weight Status.*

The base category in the multinomial dependent variable is high activation.
P > .05.
Discussion
There are several limitations to our study. Cross-sectional analysis establishes association without temporal ordering. Furthermore, unmeasured confounders could explain the associations between weight status and domains of patient activation. For example, while we controlled for some socio-demographic and health factors in multivariable analyses, residual confounding from unmeasured variables may result in biased estimates. There are also limitations in our measure of patient activation. Though the MCBS Patient Activation supplement has been validated elsewhere, it varies from those in the more widely used Patient Activation Measure (PAM), a proprietary measure set that is cost-prohibitive to use in a government survey. While the MCBS questions are different, the items are conceptually similar, focusing on knowledge and skills related to health conditions, self-management, treatments, and interacting with health providers. 31
Despite these limitations, our paper provides new insights regarding the relationship between a patient’s weight status and patient activation. We found no difference in overall patient activation by patient weight status. This non-significant finding was surprising given prior studies that suggest a negative relationship between BMI and patient activation.36,37 However, a more granular look within the domains of patient activation revealed significant differences based on weight status. Specifically, we found that patients with obesity are less confident about their ability to care for their own health, even after controlling for a broad range of socio-demographic and health factors. The confidence domain within patient activation includes questions around the ability to follow instructions about medical care as well as the ability to change habits or lifestyle. This finding aligns with other research that shows an association between obesity and low self-confidence more generally. 38
At the same time, we found that compared to respondents with normal weight, patients with obesity rated communication with providers more highly. This finding runs counter to other empirical studies that found negative 19 or no association 39 between physician-patient communication and patients’ weight status. These inconsistencies may be due to differences in questionnaire wording and emphasis. The MCBS Patient Activation supplement focuses on the aspects of provider communication that enables patient to manage their own health. For example, the survey asks patients whether they can “call my doctor’s office to get medical advice when I need it.” In contrast, surveys used in prior studies include other aspects of communication not captured in the MCBS such as perceptions around respect, fostering healing relationships, and responding to emotions.19,39 Given the widespread stigmatization of weight in medical settings, it is likely that people with obesity perceive certain aspects of provider communication more positively than others.
Conclusion
Taken together, our findings suggest that that negative perceptions about one’s own ability to manage their care co-exist with positive perceptions about patient-provider communication among older patients with obesity. These contrasting results imply that patients with obesity may benefit from receiving support from their primary care physician to develop the skills and confidence they need to successfully manage their weight. Such clinician-led efforts may include integrating Shared Decision Making (SDM) and self-management tools to help activate patients with weight problems. At a minimum, clinicians can hold discussions soliciting information and addressing questions patients may have about their weight. Barriers to patient-provider weight discussions include time constraints, sensitivity concerns, lack of training, pessimism regarding success, and negative stereotypes toward patients with obesity.18,40,41 System-wide efforts to overcome these barriers may be a challenging but worthwhile pursuit.
Supplemental Material
sj-docx-1-jpc-10.1177_21501319221129731 – Supplemental material for Obesity and Patient Activation: Confidence, Communication, and Information Seeking Behavior
Supplemental material, sj-docx-1-jpc-10.1177_21501319221129731 for Obesity and Patient Activation: Confidence, Communication, and Information Seeking Behavior by Ji Eun Chang, Zoe Lindenfeld and Virginia W. Chang in Journal of Primary Care & Community Health
Supplemental Material
sj-docx-2-jpc-10.1177_21501319221129731 – Supplemental material for Obesity and Patient Activation: Confidence, Communication, and Information Seeking Behavior
Supplemental material, sj-docx-2-jpc-10.1177_21501319221129731 for Obesity and Patient Activation: Confidence, Communication, and Information Seeking Behavior by Ji Eun Chang, Zoe Lindenfeld and Virginia W. Chang in Journal of Primary Care & Community Health
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.