
Abstract
Objective:
This case-control study investigated the association between SARS-CoV-2 infection and musculoskeletal health complaints (MHC). The specific aims of the study were (1) to compare the 1-month prevalence of MHC among post-acute COVID-19 patients and participants who never tested positive for COVID-19 matched by the former group’s age and gender; (2) to identify the predictors of MHC among all participants, and (3) define the factors independently associated with MHC in post-acute COVID-19 patients.
Methods and Analysis:
The study was conducted in Bangladesh from February 24 to April 7, 2022. The face-to-face interview was taken using a paper-based semi-structured questionnaire. MHC was measured using the musculoskeletal subscale of subjective health complaints produced by Eriksen et al. Descriptive analysis was conducted to compute MHC prevalence and compare them across groups. Multiple logistic analyses were employed to identify MHC predictors for the participants.
Results:
The prevalence of MHC was 38.7%. Adjusted analysis suggested that the SARS-CoV-2 infection was independently associated with MHC (AOR = 3.248,95% CI = 2.307-4.571). Furthermore, unemployment (AOR = 4.156, 95% CI = 1.308-13.208), moderate illness (AOR = 2.947,95% CI = 1.216-7.144), treatment in hospitals’ general word (AOR = 4.388,95% CI = 1.878-10.254) and health complaints after COVID-19 (AOR = 4.796,95% CI = 2.196-10.472) were found to be the predictors of MHC among post-acute COVID-19 patients.
Conclusion:
Our study found a robust association between SARS-CoV-2 infection and MHC and recommends that healthcare authorities be prepared to deal with the high burden of MHC among post-acute COVID-19 patients.
Introduction
Coronavirus disease 2019, reportedly known as COVID-19, is caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) and tremendously affects human health. The widespread and heterogeneous manifestation of COVID-19 undermines the respiratory, gastrointestinal, cardiovascular, or musculoskeletal systems. 1 Myalgia and arthralgia are one of the most prevalent symptoms of the COVID-19 acute phase. 2 One out of 4 COVID-19 patients complained of generalized diffuse muscle pain during the acute phase of the illness 3 ; however, there is little known about the musculoskeletal health complaints (MHC) among post-acute COVID-19 survivors.
The Global Burden of Disease Study 2019 found MHC the leading cause of disability that affected 1.7 billion people worldwide.4,5 Subsequently, since the pandemic started in 2019, more than 0.56 billion of the world population have been infected by SARS-CoV-2, and the number is increasing every day. 6 To make the situation worse, scientists predicted the incidence of MHC would be raised in the post-pandemic era in 3 specific ways.7,8 First, the illness might add new post-acute COVID-19 musculoskeletal pain patients. Second, the pain would be exacerbated in infected individuals with preexisting conditions. Finally, COVID-19 surrounding factors,9 -11 that is, economic constraints, depression, anxiety, and stress, might increase pain symptoms in noninfected people.
In many cases, such as long-COVID, COVID-19 can cause symptoms that last weeks or months after the active infection subsides. The prevalence of long-COVID can be reached up to 75% based on the severity of the acute disease and preexisting health conditions or morbidity of the patients. 12 Nonetheless, pain is one of the most powerful and persistent features of the long-COVID syndrome. 13 Evidence suggested that the overall incidence of pain (of any kind) recorded after COVID-19 was 34.2%.14,15 Similarly, a case-control study found that 38% of post-acute hospitalized COVID-19 patients suffered musculoskeletal pain. 16 Another study found the prevalence of musculoskeletal pain was 45% among the COVID-19 patients discharged from the hospitals 8 months back. 3 Though the current evidence indicated a high prevalence of musculoskeletal pain, these studies have been mainly conducted among post-acute patients previously hospitalized for COVID-19. However, a significant portion of the COVID-19 patients experienced mild to moderate symptoms and did not require hospital admission. The data regarding the association between SARS-CoV-2 infection and MHC among general community dwellers are scarce. Furthermore, to the best of our knowledge, no study compares the prevalence of MHC in post-acute COVID-19 patients with their matched counterparts at the same point in time.
This case-control study aimed to (1) compares the 1-month prevalence of MHC among post-acute COVID-19 patients and participants who never tested positive for COVID-19 matched by the former group’s age and gender; (2) identify the predictors of MHC among all participants, and (3) define the factors independently associated with MHC in post-acute COVID-19 patients.
Methods
Participants
This case-control study included participants who live at the community level in different locations in Bangladesh. Individuals who had recovered from acute SARS-CoV-2 infection were considered “case,” and those who never tested positive for COVID-19 were considered “control.” Data were collected from apparently healthy ambulatory Bangladeshi individuals aged 18 years and above for both case and control. Subjects suffering from severe chronic health conditions such as rheumatoid arthritis, stroke, cancer, and other severe systematic diseases have been excluded from this study. Bangladesh is one of the most COVID-19-affected countries in the world. To determine the sample size to target 1.9 million laboratory-tested COVID-19 positive individuals in Bangladesh, 6 a confidence level of 95%, a response distribution of 50%, and a margin of 5% error were used. Employed formula calculated a minimum sample size of 385 participants for the case data. 17 The current study procedure was prospectively approved by the Ethical Review Committee of Uttara Adhunik Medical College and Hospital. Furthermore, prospective registration for the case-control study was obtained from the WHO-endorsed Clinical Trial Registry- India: CTRI/2022/02/040449 [Registered on 21/02/2022]. The STROBE guideline for the case-control study was strictly followed entire the study. All the invited participants had provided formal informed consent for participation, collection, and analysis of their data.
Data was collected using a paper-based questionnaire comprised of 4 parts. The first part of the questionnaire asked a wide range of sociodemographic questions, including gender, age, marital status, education, employment status, monthly household income in Bangladeshi taka (৳), and present address. In the second part, participants were asked whether they had a chronic disease diagnosis (eg, hypertension, diabetes, kidney disease, and asthma), whether they were present tobacco users, and regularly performed physical exercise. These questions were answered using dichotomous options (yes/no). In the third part (only for case data), participants were asked to provide information about their COVID-19 illness. Information about the severity of the COVID-19 symptoms (mild, moderate, severe, and very severe), treatment facility they took (home, hospital’s general word, or hospital’s intensive care unit), and COVID-19 vaccine dose they received (no vaccine, one dose, 2 doses or 3 doses) were recorded. Duration of recovery from acute COVID-19 was also recorded for post-acute COVID-19 subjects. Finally, the participants were asked whether they were experiencing subjective health issues, including musculoskeletal pain, after recovering from acute COVID-19.
The last part of the questionnaire measured musculoskeletal health complaints: migraine, leg pain, headache, arm pain, upper back pain, neck pain, shoulder pain, and low back pain. The questions on MHC were based on the musculoskeletal subscale of subjective health complaints produced by Eriksen et al that estimated MHC experienced in the last 30 days.18 -20 Participants were asked to rate the occurrence of migraine, leg pain, headache, arm pain, upper back pain, neck pain, shoulder pain, and low back pain in 4 categories. The severity of each complaint is rated on a 4-point scale (0 = none, 1 = some, 2 = much, 3 = severe). Each complaint is also scored for the duration (number of days) during the last 30 days. Severity × duration has often been used to obtain a total score (0-90), indicating the degree of the complaint. 18 In this study, participants who complained of at least some pain for 3 days (1 × 3 = 3) in the last month and scored ≥3 were considered as having MHC. 19
Procedure
Data were collected from February 24 to April 7, 2022. Six trained expert researchers collected the data in 3 steps. First, 10 government-approved COVID-19 testing centers were conveniently selected in 10 different locations. Second, the data collector gathered particulars of randomly selected 600 (60 from each center) subjects who tested positive for COVID-19. After considering inclusion and exclusion criteria, 450 subjects were eligible for this study. Finally, participants who consented to collect data underwent individual face-to-face interviews at their homes or workplaces; therefore, 439 case data was collected.
Contrarily, control subjects were chosen from the case’s eligible family members, neighborhoods, or office colleagues. As a result, 439 matched individuals who provided informed consent were interviewed face to face.
Data Analysis
We dichotomized the 4 responses to the MHC question as either having the problem (yes) or does not have the problem (no). Chi-squared tests were used to compare categorical variables with and without MHC. To compute adjusted odds ratios (AORs) with a 95% confidence interval (CI), multiple logistic regression analyses were performed with MHC as a dependent variable and sociodemographic characteristics, clinical and COVID-19 illness-related factors as predictor variables for MHC. Variables were statistically significant in the 2 descriptive analyses included in the appropriate regression models. The Hosmer-Lemeshow goodness-of-fit test ensured that the models adequately fit the data. P-values < .05 were considered statistically significant. SPSS (version 22.0; IBM Corp; USA) was used to perform all data analyses.
Results
Participants’ General Characteristics
This study analyzed the data of 878 individuals (50.5% women, mean ±SD age 38.30 ± 12.77 years). Post-acute COVID-19 cohort (cases) consisted of 439 individuals (49.2% women) aged 38.33 ± 12.53 years. Contrarily, the control group had 51.7% of women with a mean age of 38.28 ± 13.01 years.
Table 1 shows that the majority of the participants were married (83.6%), with a bachelor’s degree (34.1%), service holder (33.7%), had a monthly household income ৳>45 000 (42.5%), from a nuclear family (66.6%), lived in the city (61.5%). However, only 24.0% had hypertension, 23.5% had diabetes, 10.3% had kidney disease, and 16.4% had asthma. Furthermore, only 19.8% and 38.8% of participants reported that they perform regular physical exercise and current tobacco users, respectively.
Descriptive Analysis: Sociodemographic and Clinical Factors and Musculoskeletal Health Complaints (for All Participants).
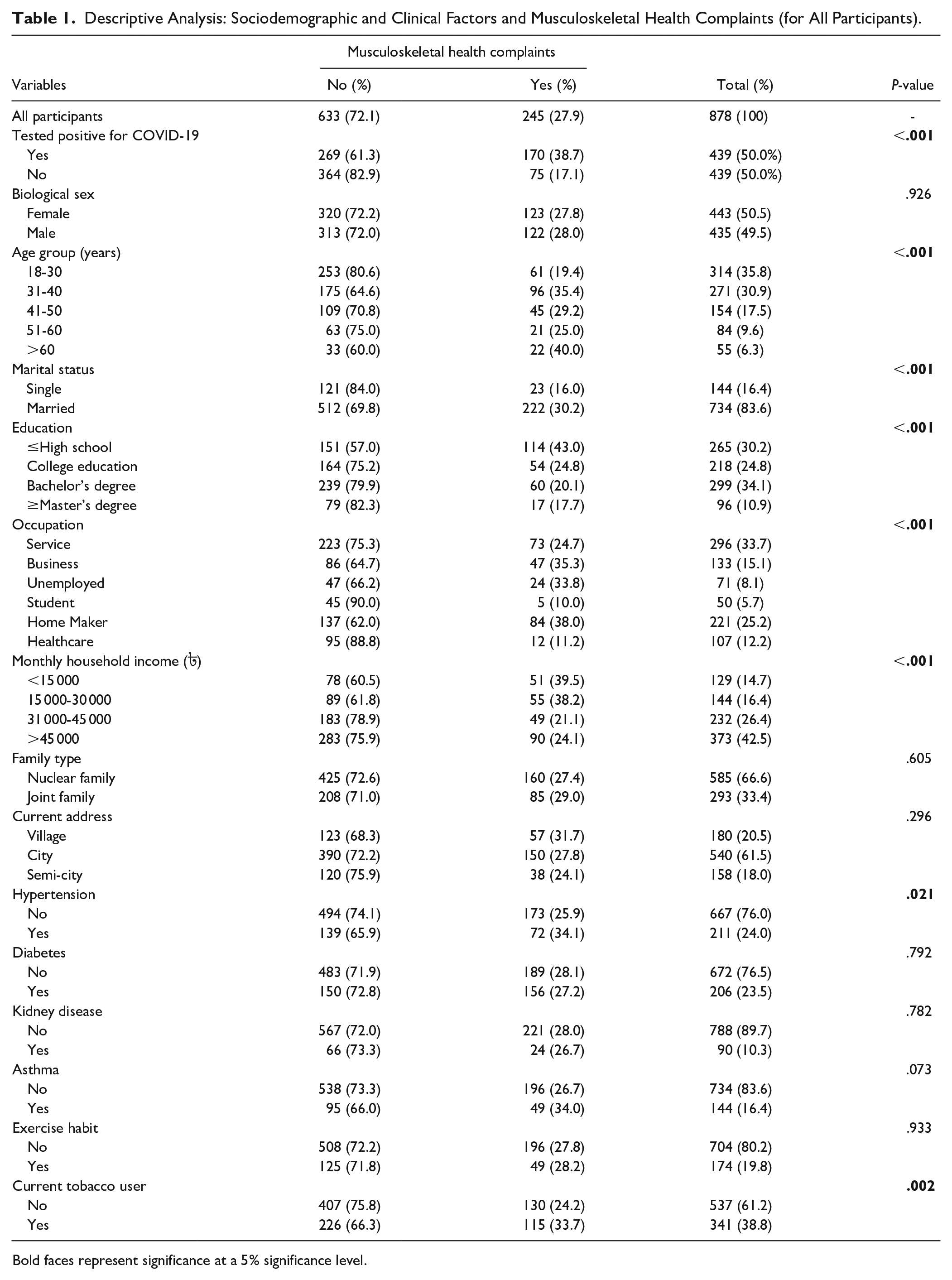
Bold faces represent significance at a 5% significance level.
Similarly, Table 2 presents the results of the case data analysis. It was observed that the majority of the participants were married (85.6%), with a bachelor’s degree (33.9%), service holder (34.4%), from a family who had a monthly household income ৳>45 000 (45.1%), from the nuclear family (67.9%), from the city (54.4%). However, only 27.3% had hypertension, 26.7% had diabetes, 14.4% had kidney disease, and 23.9% had asthma. Furthermore, only 24.4% and 44.9% of participants reported that they perform regular physical exercise and current tobacco users, respectively. In addition, the majority of the post-acute COVID-19 patients recovered from the acute illness more than 180 days ago (36.7%), had suffered from mild COVID-19 (49.9%), taken treatment at home (65.1%), were fully vaccinated before caught the disease (53.0%) and were witnessing subjective health issues after COVID-19 (82.2%).
Descriptive Analysis: Sociodemographic, Clinical, and COVID-19-Related Factors and Musculoskeletal Health Complaints (for Post-Acute COVID-19 Patients).

Bold faces represent significance at a 5% significance level.
Descriptive Analysis of All Data
Descriptive analysis of all data suggests the prevalence of MHC is 27.9%. However, the prevalence of MHC was significantly higher among the cases than in the controls (38.7% vs 17.1%; P ≤ .001). Closer analysis suggested that the prevalence of individual MHC that is migraine (10.5% vs 2.1%, P ≤ .001), leg pain (19.6% vs 7.7%, P ≤ .001), headache (26.2% vs 10.7%, P ≤ .001), arm pain (10.3% vs 4.3%, P = .001), upper back pain (16.6% vs 7.5%, P ≤ .001), neck pain (21.4% vs 8.9%, P ≤ .001), shoulder pain (17.1% vs 3.2%, P ≤ .001) and low back pain (24.4% vs 15.7%, P ≤ .001) was significantly higher among cases than in their counterparts (Figure 1). In addition, aged (40%, P ≤ .001), married (30.2%, P ≤ .001), participants with lower education (43%, P ≤ .001), homemaker (38%, P = .001), participants with lower household income (39.5%, P ≤ .001), participants who diagnosed with hypertension (34.1%, P = .021) and current tobacco user (33.7%, P = .001) reported MHC in significantly higher rate (Table 1).

Prevalence of musculoskeletal health complaints among non-COVID and post-acute COVID subjects.
Adjusted Analysis of All Data
Regression model 1 identified 3 variables with higher AOR as the predictors of MHC among all participants. The variables are: post-acute COVID-19 (AOR = 3.248,95% CI = 2.307-4.571), unemployment (OR = 3.297,95% CI = 1.371-7.924), and hypertension (OR = 1.544,95% CI = 1.001-2.380) (Table 3).
Multiple Logistic Regression Analysis of All Data.
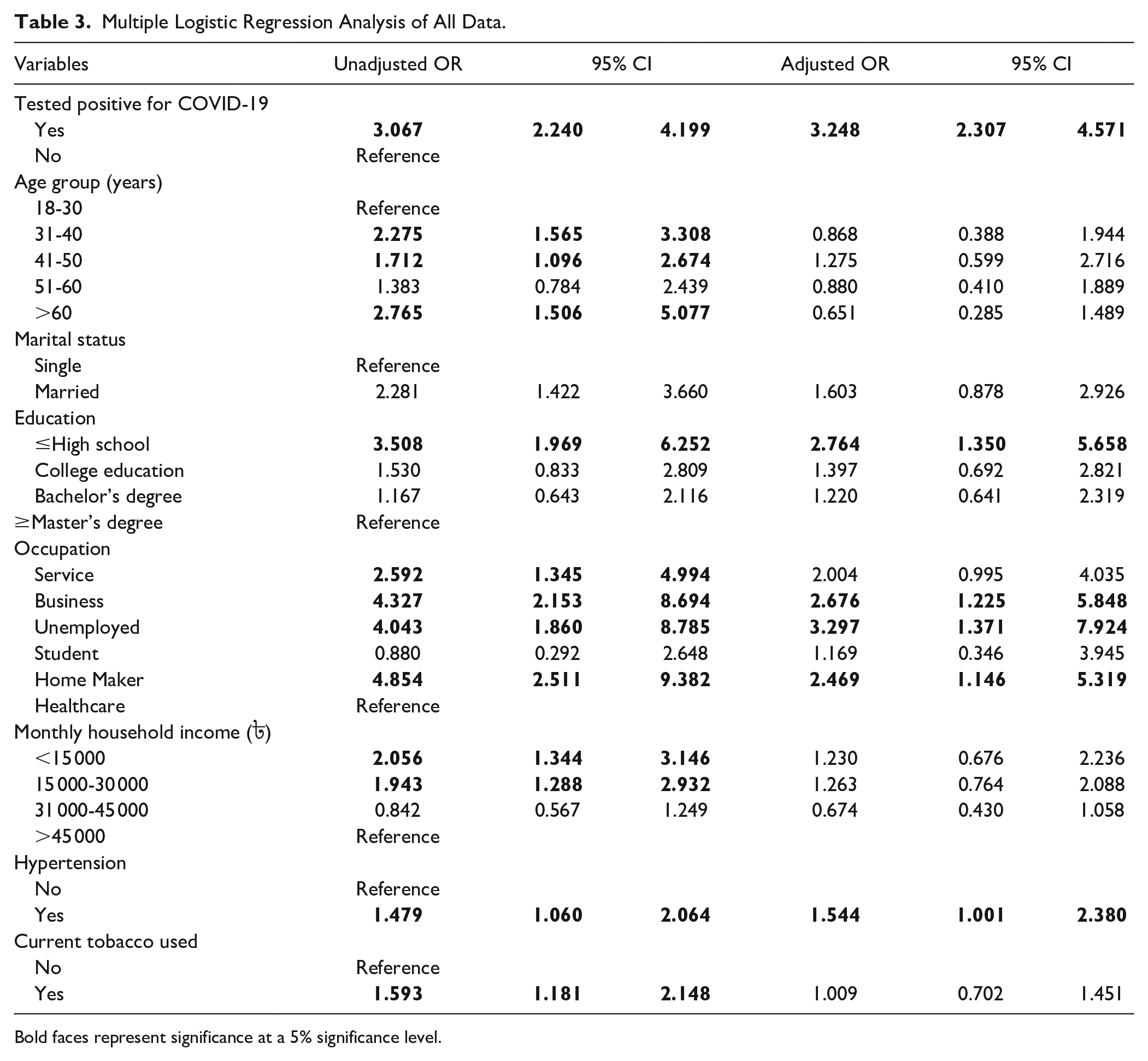
Bold faces represent significance at a 5% significance level.
Unadjusted Analysis of Case Data
Unadjusted analysis suggested that the higher odds of MHC was found in participants aged 31 to 40 years (OR = 1.928,95% CI = 1.201-3.097), married individuals (OR = 3.080,95% CI = 1.590-5.968), participants with lower education (OR = 3.021,95% CI = 1.509-6.047), homemaker (OR = 4.632,95% CI = 2.131-10.068), participants with lower household income (OR = 2.206, 95% CI = 1.209-4.026), participants diagnosed with kidney disease (OR = 1.857,95% CI = 1.026-3.360), participants who recovered from acute COVID-19 in less than 3 months (OR = 1.933,95% CI = 21.231-3.033), participants who were suffering from moderate COVID-19 (OR = 3.714,95% CI = 1.912-7.212), participants who had taken treatment at hospital’s general word (OR = 2.676,95% CI = 1.912-7.212), participants who were fully vaccinated before caught COVID-19 (OR = 1.717,95% CI = 1.102-2.676). Furthermore, participants who reported experiencing subjective health complaints, including MHC as a post-COVID sequela, had higher odds of MHC (OR = 4.794,95% CI = 2.452-9.375) (Table 4).
Multiple Logistic Regression Analysis of Post-Acute COVID-19 (Cases) Data.

Bold faces represent significance at a 5% significance level.
Adjusted Analysis of Case Data
Regression model 2 suggested that being married (AOR = 2.862,95% CI = 1.195-6.854), unemployment (AOR = 4.156,95% CI = 1.308-13.208), moderate COVID-19 symptom (AOR = 2.947,95% CI = 1.216-7.144), treatment in hospitals’ general word (AOR = 4.388,95% CI = 1.878-10.254) and subjective health complaints as post-COVID-19 sequelae (AOR = 4.796,95% CI = 2.196-10.472) were independently associated with MHC among the case cohort (Table 4).
Discussion
This case-control study revealed that the prevalence of MHC was significantly higher among the individuals who had recovered from acute SARS-CoV-2 infection than the non-COVID subjects. Furthermore, SARS-CoV-2 infection was a robust predictor of MHC. Analysis of case data suggested that the marital status, occupation, severity of COVID-19, treatment facility received by the patient during illness, and status of post-COVID subjective health complaints were independently associated with MHC.
Prevalence of MHC
A systematic review and meta-analysis of post-acute COVID-19 pain studies concluded that almost 10% of post-acute COVID-19 individuals would be suffering from musculoskeletal post-COVID pain syndrome. 21 However, a survey conducted among hospitalized post-acute COVID-19 patients found that 45.1% of participants reported musculoskeletal pain after 8 months of discharge from the hospital. 3 Another case-control study found that the prevalence rate of musculoskeletal pain was 38% among post-acute COVID-19 patients. 16 Similar to these prevalence rates, our study estimated the prevalence of MHC at 38.7% among the community-level post-acute COVID-19 population. Additionally, our study explored the prevalence rate of MHC among the individuals who have taken treatment for COVID-19 at home, in the hospitals’ general world or ICU; therefore, it provided more plausible public health evidence regarding the association between SARS-CoV-2 infection and MHC. Interestingly, we found higher MHC odds among those who took treatment at the hospital’s general word.
Contrarily, about 50% of the participants reported MHC those recovered from the acute illness in 90 days or less. The rate reduced to 31% as the recovery duration surpassed 3 months, increasing slightly after 6 months. However, the prevalence rate of MHC was significantly higher if we compare the rates with that of the controls (17%). Thus, our study indicated that the SARS-CoV-2 infection was potently related to MHC regardless of the recovery time from the acute illness. Previous studies reported similar fluctuation of MHC prevalence during the time course of recovery from acute illness.3,16,21 Nonetheless, additional longitudinal studies are warranted to understand the long-term impact of SARS-CoV-2 infection in MHC.
Predictors of MHC
There is a clinical implication of the identification of risk factors for MHC. Our study found SARS-CoV-2 infection a robust independent associated factor of MHC. In general, lower educational qualifications and unemployment were also independently associated with MHC. Evidence suggestes that the MHC is becoming a growing concern in low-income and low-resource settings. 22 Furthermore, COVID-19-induced mental health and economic stressor among these cohorts may further explain the higher prevalence of MHC.9,11 Limited access to health facilities among unemployed and individuals with lower education may explain the higher prevalence of MHC, and highlight significant public health concerns.
In addition, we found moderate illness, treatment in hospitals’ general word and subjective health complaints after acute COVID-19 as the significant predictors of MHC among post-acute COVID-19 patients. Previous studies revealed that a reasonable prognosis of COVID-19 was related to preexisting or post-acute MHC.3,23 Though further study is warranted to explain the possible complicated inter-relationship of the COVID-19 severity or prognosis and MHC, our study provided substantial evidence that those who suffered from mild to moderate illness might suffer from MHC at any point in the post-acute recovery stage. As a high number of COVID-19 patients were suffering from mild to moderate illness, our study would stress preparing the health sector to tackle upcoming waves of MHC in the post-COVID era.
Limitation of the Study
First, we did not take data regarding ergonomic factors and the participants’ working nature, such as sedentary or heavy weight lifting. Second, participants’ BMI was not measured, which might confound the study findings. Finally, as we have taken information on MHC occurrence in the past month, the chronicity of MHC that is acute, sub-acute, or chronic cannot be measured from this data. Despite these limitations, this study added valuable information supporting the potential for an increase in chronic pain after the COVID-19 pandemic.
Conclusion
The forecast suggests an unprecedented prolonged pandemic. The health impact will likely manifest in both infected individuals and people spared infection but are nevertheless adversely affected by disruptions in everyday life and experience a wide array of physical, psychological, and social stressors. Based on the shreds of evidence, it is postulated that the cumulative impact of the pandemic will lead to an increase in MHC in the immediate and possibly long-term future. Amidst many uncertainties, the findings of our study would further encourage the research community to study, devise, and implement strategies to mitigate the pain-related health consequences of this pandemic. The timely recognition of new MHC or exacerbations of preexisting MHC, prompt and targeted management, and strategies to mitigate the potential impact on health are strongly encouraged.
Footnotes
Acknowledgements
The authors are thankful to the participants for providing the information used to conduct the study. The authors are also grateful to Dr. Nirupam Das of the Bangladesh Doctor’s Foundation and Nur-A-Safrina Rahman for helping with data collection.
Author Contributions
Mohammad Ali: conceived and designed the experiments; performed the experiments; analyzed and interpreted the data; contributed reagents, materials, analysis tools, or data; wrote the paper. Atia Sharmin Bonna, Abu-sufian Sarkar, Md. Ariful Islam: performed the experiments; contributed reagents, materials, analysis tools, or data; reviewed the paper.
Data Access,Responsibility,and Analysis
Dr. Mohammad Ali had full access to all the data in the study and took responsibility for the data’s integrity and the data analysis’s accuracy.
Data Sharing Statement
Data will be made available on request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.