
Abstract
Objectives:
This study examines the implementation and short-term effects of a Learning Partner Model (LPM)-based educational program on cancer prevention and control information for community health volunteers in Japan.
Methods:
The program was undertaken by 3 local governments in collaboration with a government initiative and offered a 90-min group workshop to community health volunteers. Community health volunteers (primary participants) recruited in turn friend or family members (secondary participants) with whom they were prepared to share the content of the workshop with the help of printed materials received in the workshop. We conducted self-administered paper and pencil questionnaire surveys before, immediately after, and 3 months after the workshop. The t-test, Fisher’s exact test, paired t-test, and McNemar test were used to compare the 2 groups’ demographic characteristics and healthy habits at pretest. Repeated measures ANOVA was used to compare cancer prevention knowledge between groups and over time.
Results:
Of 142 participants, 107 pairs of learning partners (primary and corresponding secondary participant) completed all questionnaires. All primary participants and 37.4% of the secondary participants were women, and 57.9% of the learning partners were spouses. The results showed significantly higher correct answers on the cancer-prevention knowledge questions in the post-workshop and follow-up surveys compared to the pre-workshop survey (P < .001). The increase in knowledge was observed in all learning-partner groups in all 3 sites.
Conclusion:
The study demonstrates a promising strategy that can be adapted to the health needs of the community beyond cancer prevention and control, building on the efforts of local governments and government health initiatives.
Keywords
Introduction
Cancer occupies a large share of the world’s disease burden, and in Japan, 1 in 2 citizens will be diagnosed with cancer at some point in their life (Ferlay et al). 1 After the 2006 Cancer Control Act, the Japanese government formulated 5-year Basic Plans to promote cancer control in 2007, 2012, and 2017. These Basic Plans intended to have local governments determine prefectural plans, establish Cancer Control Promotion Councils, and devise policies to promote comprehensive cancer control in municipalities and companies. In the second and third Phases, the Basic Plans’ central items were cancer control, education, and public awareness that explicitly noted that the general public, and not just cancer patients and their families, should also be educated about cancer control.
International organizations have documented areas of improvement in the general public’s health knowledge such as primary prevention.2,3 Specifically, the National Cancer Center identified gaps in knowledge about cancer risk factors and prevention methods in Japan. 4 The 2017 to 2018 revision of the Curriculum Guidelines by the Ministry of Education, Culture, Sports, Science and Technology (MEXT) specified that students should be taught this preventive knowledge in health and physical education classes. Thus, the groundwork is being laid in grade-school education to increase cancer prevention knowledge in Japan. Meanwhile, Japanese adults have also been reported to have a low level of familiarity with cancer prevention information. 5
In Japan, government institutions have long engaged in public awareness activities on cancer prevention by training community health volunteers, known as Health Cooperators and Cancer Control Promoters. 6 What these health volunteers have in common is that most of them are adults, often retired women in their 60s and 70s, and that they have adopted a leadership role in solving a variety of problems in their communities. 7 Engaged in activities rooted in their communities, these volunteers are effective communicators, and local governments rely on them to use their talents in health promotion activities, which is highlighted in the Ottawa Charter for Health Promotion. 8
There have been some examples of community health volunteers holding the primary responsibility for spreading cancer prevention knowledge in their communities.6,9,10 The current study focuses on the implementation of the Learning Partner Model (LPM) in which knowledge based on scientific foundations is transferred from person to person in an everyday environment.11,12 In the context of cancer prevention, community health volunteers first acquire science-based knowledge on cancer prevention in a particular course. As participants in the course (primary participants), they also prepare for the diffusion of knowledge and designate someone in their social network as their learning partner (secondary participant). The LPM relies on an active learning method through which the primary participants transfer their newly acquired knowledge to the secondary participants. As a result, the secondary participants have also been reported to acquire cancer prevention knowledge, even though they do not directly participate in the course.
Diffusion of knowledge from primary to secondary participants occurs through one-on-one conversations and with the support of educational materials that are used during the course and shared amongst the learning partners. Japanese reports on the effect of using printouts to spread knowledge on cancer prevention have mostly focused on the context of school education. 12 In a study focusing on hypertension, health-related printouts distributed to company employees impacted the management of one’s hypertension. 13 It also found that women are more likely to read health-related printouts than men. 14 The effectiveness of printouts in spreading knowledge on health has also been reported in a case where residents in a Japanese rural community were given self-checkup sheets to develop their oral health. 15 An interventional study on Japanese female university students also found a higher educational effect of handing out printouts on pregnancy and drinking alcohol in conjunction with individual lectures than that of simply distributing the printouts within the general population. 16 Similarly, our study includes an educational program that includes a lecture and the distribution of educational materials among community health volunteers.
The goal of this study was to implement and examine the effectiveness of an LPM-based educational program for spreading cancer prevention knowledge in Japan. The program was part of a health education project for community health volunteers that was undertaken by 3 local governments in collaboration with a government initiative organized by our research team.
Methods
Cancer-Prevention Course and Diffusion of Cancer-Prevention Knowledge
With the aim of enabling the team to conduct action research, we established collaborations with 3 different local governments that were about to embark on a cancer prevention information dissemination program by community health volunteers within the neighboring Kanto region area during the 2016 fiscal year. Each of the local governments collaborating in the study offered the same cancer prevention course to community health volunteers in a group setting, 1 group in each of the 3 locations. A doctor specializing in medical oncology gave 1.5-h lectures using the same material at all 3 locations in designated lecture rooms. The course topics included primary cancer prevention (not smoking, improving one’s diet, physical activity, and other everyday healthy habits), encouraging undergoing early detection cancer screenings, and understanding cancer patients’ and their families’ feelings. After each lecture, the public health nurse from the corresponding local government verbally encouraged the primary participants to identify a friend or family member with whom they could share their new knowledge (ie, “secondary” participants) so that they would become learning partners. Participants also received handouts with information to share with their learning partners. Please see Supplemental Appendix A for an overview of the health education program.
Project Participants and Data Collection
The 3 local governments collaborating in the study had a community health volunteer certificate program and conducted regular monthly meetings with the volunteers. During the monthly meeting in April 2016, at the beginning of the fiscal year, each of the sites invited all their certified community health volunteers to participate in the project. Besides the information discussed during the meeting, a written description was provided. Site coordinators also reached out to certified community health volunteers who had not attended the meeting in April. A total of 142 community health volunteers agreed to participate and attended one of the cancer-prevention lectures that were conducted between May 2016 and February 2017 at the 3 sites. To accommodate logistic and administrative constraints of the existing community health volunteer programs in all 3 sites, a quasi-experimental design method was agreed upon. Participants were asked to complete a self-administered questionnaire before the course (pretest), immediately upon completion of the course (posttest), and 3 months after the course (follow-up). We distributed and collected the questionnaires in our meetings with the primary participants. The questionnaires were distributed also to secondary participants and completed questionnaires were collected at a location designated by each local government. The survey was administered without fixed dates or times, as long as it took place within the corresponding pretest, posttest, or follow-up survey period. We asked each local government’s designated public health nurse to secure 10 min for each survey, in accordance with the implementation manual.
Upon completion of the study, 107 pairs of learning partners had completed all 3 sequential measurements.
The questionnaires included items about demographic characteristics (sex, age, and occupation), whether the participants follow any of 7 healthy habits, 17 and cancer prevention knowledge. To assess respondents’ cancer prevention knowledge, we used a 14-item scale in which participants selected risk factors they perceived to be associated with cancer. Eight of the 14 items represent evidence-based cancer risk factors in Japan 5 so that the maximum score was 8 if all 8 risk factors were identified correctly. The risk factors include tobacco smoking, alcohol drinking, poor vegetable and fruit intake, excessive salt intake, unbalanced diet, physical inactivity, obesity, and cancer-causing viral and bacterial infections. In addition, secondary participants also revealed their relationship with the primary participants and city where they lived. Please see Supplemental Appendix B for an English translation of the questionnaire.
Method of Analysis
Out of the 142 primary participants attending the course, we selected 107 (75.4%) for analysis as these had no missing data, and both primary and secondary participants had responded to all 3 surveys.
To examine potential differences between primary and secondary participants at pretest, we used t-test, Fisher’s exact test, paired t-test, and McNemar test as applicable to the demographic variables and self-reported healthy habits. To assess changes in learning partner groups’ cancer prevention knowledge before and after the intervention, 2-way repeated measure ANOVA was used with primary vs. secondary participation (between-subjects) and pretest, posttest, follow-up (within-subjects) as independent variables.
P < .05 was considered the critical level of statistical significance. All statistical analyses were performed using IBM SPSS Statistics Version 20 (IBM Japan, Ltd.).
Ethical Considerations
We obtained primary participants’ consent in writing for their cooperation in all 3 surveys. The first author wrote an explanatory document and verbally explained the survey’s purpose beforehand. We secured the secondary participants’ participation by having the primary participants present the explanatory document and verbally explain the survey to obtain their consent. This study was approved by the Research Ethics Committee of the first author’s research institution (application no. 2016-3, approved April 28, 2016).
Results
Table 1 displays the participants’ demographic characteristics and self-reported healthy habits. The primary participants’ mean age was 66.5 ± 4.0 years. For the secondary participants, it was 63.0 ± 12.8. Although significantly lower, the secondary participants’ ages had a wider range, with a standard deviation of 12.8 compared to the primary participants’ 4.0 (P = .008). All 107 primary participants were women and most secondary participants (67; 63.6%) were male, which is consistent with the fact that most learning partners were spouses (62; 57.9%). Other than spouses, the relationship between learnings partners was most often described by secondary participants as friends (20; 18.7%), followed by child (10; 9.3%) and parent (9; 8.4%). Most secondary participants (98; 91.6%) lived in the same community as their primary participants.
Demographic Characteristics and Self-Reported Healthy Habits at Pretest Among Primary and Secondary Participants.
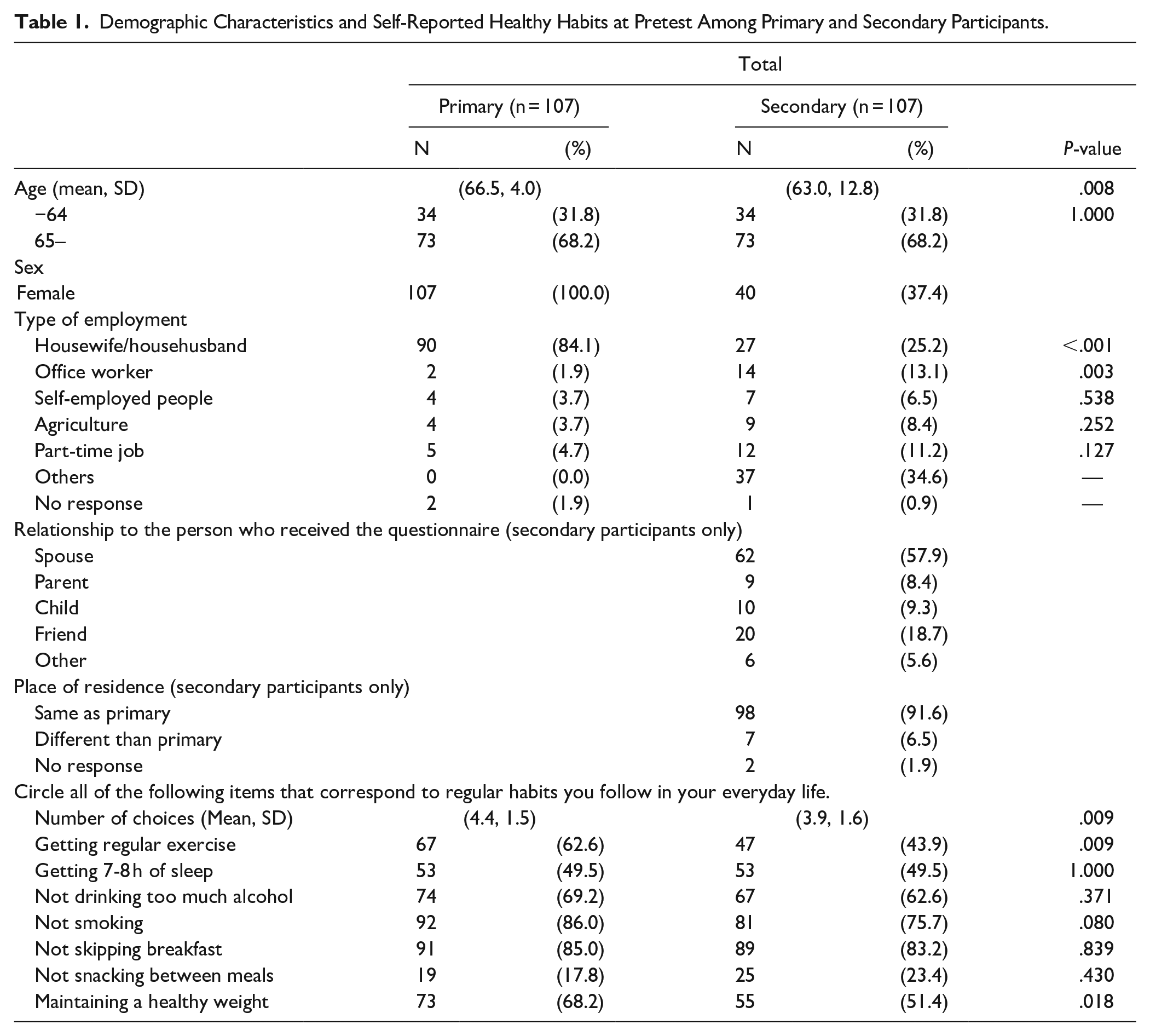
There were statistically significant differences in the proportion of primary and secondary participants who were housewife/househusbands (84.1% vs 25.2%) and employed company office workers (1.9% vs 13.3%). Regarding occupation, approximately a third of secondary participants selected “other,” with 90% of them in this group indicating that they were currently unemployed.
At pretest, the mean number of self-reported healthy habits was 4.4 for the primary participants and 3.9 for the secondary participants, representing a statistically significant difference (P = .009). More specifically, statistically significant differences were found in the proportion of respondents who selected “getting regular exercise” (67 vs 47; 62.6% vs 43.9%; P = .009) and “maintaining a healthy weight” (73 vs 55; 68.2% vs 51.4%; P = .018).
Table 2 presents the cancer knowledge mean scores at pre-test, post-test, and follow-up for primary and secondary participants as well as the results of the 2-way repeated measures ANOVA. The results indicate that both learning-partner groups increased their cancer knowledge upon completion of the course (within effects P < .001). No difference in the pattern of change emerged between the primary and secondary participants (interaction effect P = .478). Total scores of the primary group were statistically significantly higher than the secondary group at all measurements over time (between group effects P < .001).
Cancer knowledge at pretest, post-test and follow-up among primary and secondary participants.

Total score comparison between primary and learning partners. Full scores: 8 points.
P-value: interaction.
P-value: repeated measures 2-way ANOVA (between-subject).
Discussion
This study assessed the implementation and short-term effects of an LPM program in community health volunteers’ (primary participants) transferring of knowledge on cancer prevention directly to their social circle (secondary participants). We observed statistically significant knowledge improvements in both the primary and secondary participants when post-test and follow-up surveys were compared to the pretest surveys. Overall, the follow-up showed a non-statistically significant decline in knowledge compared to the post-test results in all learning partner groups.
The program was successfully implemented in 3 distinct municipalities in Japan following the same protocol. In addition to the 90-min lecture that was central to the program, all primary participants were community health volunteers and printed materials were used to support the transmission of knowledge from primary to secondary participants.
Japan’s community health volunteers have been found to exert a positive influence on their families and community residents, because they have always traditionally had a role of maintaining and fostering the social capital that is rooted in the community, such as trust and networks. 18 The sociodemographic characteristics of community health volunteers in our study are similar to the national average reported by Taguchi et al, 7 who conducted a survey on the living conditions of health volunteers in Japan. In our sample, all primary participants were women and 84.1% were housewives which reflects the time and social flexibility that is necessary to serve as community health volunteers. Housewives have been reported to not only improve their own quality of life, but have also a positive effect on others, mostly their family.19,20
The primary participants in this study chose an average of 4.4 healthy habits in their responses, which was statistically significantly higher than the 3.9 average of the secondary participants (P = .009). In particular, the proportion of respondents who chose “getting regular exercise” and “maintaining a healthy weight” was significantly higher among primary compared to secondary participants. While the results have limitations because they are based exclusively on self-report, they are consistent with previous studies indicating that community health volunteers, the primary participants in this study, are a more health-aware group than the general public. 21 To spread this knowledge in Japanese communities, it is important for community health volunteers to first acquire that knowledge and then pass it on to those close to them.
In this study, in addition to the 90-min lecture attended by primary participants, the use of printouts reinforced the primary participants’ knowledge on cancer prevention and represented an appropriate tool for transferring that knowledge to the secondary participants. However, based on the Learning Pyramid model, which claims that the greatest effect of active learning is in communicating the newly learned knowledge to others, 22 understanding the exact effect of these printouts is limited and is a task for future research.
Programs to spread knowledge among Japanese adults have either way predominantly involved passing out or publicly posting printouts. Thus, this study is novel for examining the effect of an LPM program to spread knowledge through community health education. Based on this study, health education programs should be reexamined as parts of a strategy to spread health knowledge in communities. The components of the program in our study could be easily applied to other health areas. For example, the results of this research can be applied to disseminate an understanding of contemporary issues facing local communities, such as disaster preparedness, COVID-related issues, and so on.
Previous studies have reported that community health volunteers’ involvement in actual volunteering activities are related to the training’s particularly marked impact on their sense of satisfaction in their future activities and that satisfaction also correlates with the length of time they continue these activities. 23
The primary participants in this study may occasionally need to personally cover costs becoming a health volunteer. 24 In addition, reducing the associated psychological burden is also a pressing research task. 25 Ultimately, reducing these burdens will lead to the sustainability of transferring and spreading knowledge on cancer prevention through community health volunteer programs.
On the other hand, a few points should be noted with regard to spreading knowledge on cancer prevention. In the context of educating children about cancer in school, a significantly high proportion of children chose “someone who smokes and drinks too much” as their representative cancer patient after their cancer-prevention class. 26 While smoking and drinking alcohol are controllable risk factors for cancer, 2 it does not mean that all cancer patients were smokers. That is to say, improving knowledge on cancer prevention may also encourage prejudice against cancer patients. Previous studies have found that it is easy for people to be prejudiced against, for example, lung cancer patients by equating them with smokers, which raises the issue of cancer stigma.27,28 From this, since the primary participants in this study were health volunteers, who maintained positive healthy habits and were responsible for increasing others’ awareness of these habits, it is necessary to hear the opinions of cancer patients and survivors to devise appropriate methods of spreading knowledge about cancer prevention. In other words, when conducting disease prevention education, it is necessary to provide well-balanced learning content with a view to coexistence with patients.
Limitations and Strengths
This study has several limitations. First, because we used a self-administered questionnaire to collect data, the results were based exclusively on self-report. Thus, there is a possibility that respondents gave socially desirable responses when reporting health habits. Second, selection bias may also influence the results, as 75.4% completed all questionnaires and were eligible for analysis. Correspondingly, selective retention can result in overestimating the program’s effect if participants getting the most out the program were more likely to complete all questionnaires. In addition, the quasi-experimental design limits the extent to which the increase in cancer-risk knowledge can be attributed to our program and not to other initiatives, or to the Hawthorne effect, whereby becoming a research subject may make participants feel like something is expected of them and cause them to change their behavior, ultimately leading to a desirable outcome. 29
Further, the decrease in knowledge on cancer prevention seen in the follow-up survey suggests that future research should evaluate how people can retain the knowledge acquired in the course and develop strategies to support gains in health literacy that may have been facilitated by the program.
Nonetheless, this study also has some important strengths. Previous researchers have emphasized the value of community-based participatory research where academic and community partners learn from each other during the implementation of the study. 30 Our project was conducted as a partnership of 3 different sites in collaboration with government initiatives and was implemented successfully. Further, increases in knowledge in secondary participants were consistent with changes observed in community health volunteers and this was observed in all 3 sites. This strengthen the possibility that an increase in knowledge can be attributed to participation in the program.
A previous study conducting a similar cancer prevention group session to members of the general public showed that knowledge among participants attending the lecture was statistically significant higher at posttest compared to pretest. 12 The results of this study suggest that providing the lecture and pertinent printed materials to community health volunteers can be a complementary and useful strategy to increase cancer health literacy in the adult population in Japan.
Conclusions
We implemented an LPM-based educational program for cancer prevention in Japan, as part of a health education program for health volunteers, undertaken by 3 local governments in collaboration with a government initiative. The results revealed improvements in both primary and secondary participants’ cancer prevention knowledge. As such, we conclude that the activities of the community health volunteers attending the course and using printed materials were critical factors contributing to the LPM-based program’s effectiveness in spreading knowledge. We recommend future studies test more health promotion programs using LPM and further explain the mechanisms of raising awareness. The strategy may represent a particularly useful and efficient tool to reach out to the general population and apply to timely health topics beyond cancer.
Supplemental Material
sj-docx-1-jpc-10.1177_21501319221110682 – Supplemental material for The Effect of a Learning Partner Model-Based Program on Spreading Cancer Prevention Knowledge Using Community Health Volunteers in Japan
Supplemental material, sj-docx-1-jpc-10.1177_21501319221110682 for The Effect of a Learning Partner Model-Based Program on Spreading Cancer Prevention Knowledge Using Community Health Volunteers in Japan by Hiroko Yako-Suketomo, Asae Oura, Kayoko Katayama, Kyohei Saito, Ken Ohashi and Ana M. Navarro in Journal of Primary Care & Community Health
Supplemental Material
sj-docx-2-jpc-10.1177_21501319221110682 – Supplemental material for The Effect of a Learning Partner Model-Based Program on Spreading Cancer Prevention Knowledge Using Community Health Volunteers in Japan
Supplemental material, sj-docx-2-jpc-10.1177_21501319221110682 for The Effect of a Learning Partner Model-Based Program on Spreading Cancer Prevention Knowledge Using Community Health Volunteers in Japan by Hiroko Yako-Suketomo, Asae Oura, Kayoko Katayama, Kyohei Saito, Ken Ohashi and Ana M. Navarro in Journal of Primary Care & Community Health
Footnotes
Acknowledgements
This study was presented in part at the 76th Annual Meeting of the Japanese Society of Public Health (JSPH). We would like to express our thanks to all those whose help we received.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Japanese Society for the Promotion of Science (JSPS) Grant-in-Aid for Scientific Research [Fundamental Research C, grant no. JP15K01665]; and conducted as part of the Comprehensive Research Project to Promote Cancer Control, supported by a grant from the Ministry of Health, Labor, and Welfare [project no. H29–Cancer Control–General–020].
Ethics Information
This study was conducted with the approval of the Research Ethics Committee of the Japan Women’s College of Physical Education (application no. 2016-3, approved April 28, 2016).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.