
Abstract
Background:
Ending the HIV Epidemic is a campaign dedicated to reducing new HIV infections in the United States by 90% by 2030. Preexposure prophylaxis (PrEP) holds significant promise as a prevention tool. However, uptake has not improved much since then. As a result, this research looked at how PrEP literacy relates to sexual communication self-efficacy
Methods:
Between August 4 and 21, 2020, we performed a community-informed cross-sectional study of Black and Latino residents in Indiana. We collected demographic information as well as PrEP literacy, sexual communication self-efficacy, and awareness of HIV status.
Results:
Being unaware of one’s own HIV status and being unsure of one’s sexual identity were both linked to reduced self-efficacy in the domain of sex communication. Those who had a greater level of PrEP literacy felt more confident in their ability to communicate with others about sexually related topics. People living in rural areas showed a significantly lower degree of sexual communication self-efficacy than participants in urban settings.
Conclusion:
Providing information about PrEP to those at risk of acquiring the virus may help them connect with treatment or prevention services. Healthcare professionals should take the time to understand their patients’ levels of PrEP literacy and communication self-efficacy regarding sexual health.
Introduction
Entering the fifth decade of the epidemic, HIV continues to be a significant global health concern. During 2019 in the United States, approximately 36 398 individuals received an HIV-positive diagnosis. 1 People of color continue to be disproportionately impacted by HIV. Among new HIV diagnoses in 2019, 42.1% occurred among Black individuals, and 28% were attributed to Latinx, compared to 2% who were white and 2.5% who identified as Asian.1,2 Black Americans also represent the largest HIV incidence rate which was 45.4 per 100 000 compared with their white counterparts who report an HIV incidence rate of 5.2 per 100 000. 2
Latinx individuals account for approximately 18.5% of the U.S. population, yet they represent the second-highest HIV incidence rate (23.4%) and 21.6% of those living with undiagnosed HIV.2-4 Despite a decline in new HIV diagnoses, the number of Latinx diagnoses has increased. Recent research by Arya et al 5 found that being unaware of HIV testing guidelines or disagreeing with the CDC’s guidelines was a significant barrier to testing among Latinx individuals.
Diagnosing HIV as early in the infection process as possible is essential to linking individuals into the HIV care continuum and achieving viral suppression. However, the number of Americans who are unaware of their HIV-positive status continues to be an issue. Many populations have noted a general decrease in HIV incidence between 2015 and 2019 including white, Asian, and Black individuals. 1 However, HIV incidence continues to be highest among Black Americans and has increased by 30% among Black men who have sex with other men (MSM).6,7 An estimated 22.2% of Black Americans and 21.6% of Latinx Americans are living with HIV/AIDS undiagnosed. 4
Having no knowledge of one’s HIV status is a major barrier to ending the HIV epidemic. As a result of being unaware of their HIV status, people are omitted from treatment and risk inadvertently transmitting HIV to their sexual partners. All races and ethnicities considered MSM are disproportionately affected by HIV. However, heterosexual men represent the highest percentage of people living with undiagnosed HIV, at 16.6%, compared to 15.2% of people who identify as MSM. 8 The increased percentage of those who identify as heterosexual living with undiagnosed HIV infection highlights the importance of addressing HIV outside of the sexual identification lens and focusing on sexual, behavioral, and structural risk factors placing individuals at increased risk. Applying universal screening policies is 1 way to identify those who are HIV positive, connect them with appropriate treatment plans, and help maintain viral suppression.
A significant advancement in HIV prevention occurred in 2012 with the Food and Drug Administration’s approval of preexposure prophylaxis (PrEP), the first medication used to prevent the acquisition of HIV. According to research, PrEP can reduce the transmission of HIV by more than 90% when used according to instructions. 9 However, PrEP uptake remains low. The number of Americans identified as appropriate candidates for PrEP in 2015 to 2016 exceeded 1 million, but only 8% were prescribed the medication, and only 1% of Black Americans identified as suitable candidates were prescribed PrEP. 10
How people talk about sex and sexual health has been shown to influence sexual behavior factors such as HIV and condom use.11,12 Additionally, feeling more confident discussing sexual health has been associated with improved sexual communication skills, positive attitudes toward condoms, and more frequent condom use.13,14 While the findings regarding sexual health communication are encouraging, the majority of the literature focuses on patient and provider or parent-child communication self-efficacy, largely omitting the experiences of sexual partner communication self-efficacy.15,16 Therefore the current study was developed to address the gap in the literature and better understand the intersectionality of sexual health self-efficacy and HIV prevention among people of color.
Materials and Methods
Study Design
A cross-sectional study was conducted between August 4, 2020, and August 21, 2020, using the Qualtrics online survey platform. In addition to its online survey platform, Qualtrics offers a variety of research services, including Qualtrics Panels.17,18 Qualtrics Panels is a research panel managed by Qualtrics, in which surveys are distributed to a targeted population of respondents. It has been demonstrated in the literature that the use of survey panels yields high-quality responses from a representative sample.18,19 The inclusion criteria were as follows: (1) being 18 or older, (2) being a current resident of Indiana, and (3) identifying as Black or Latino. The exclusion criteria were as follows: (1) being under the age of 18, (2) not being a current resident of Indiana, and (3) not identifying as Black or Latino. It was estimated that a sample size of 384 would be required to provide results representative of the Indiana Black and Latinx population, with a 5% margin of error and a 95% confidence level. All procedures and materials were approved by the Indiana University Institutional Review Board.
In order to participate in the survey, participants were required to read a study information sheet and provide their electronic consent. To ensure high-quality responses, an instructional verification question was used. 20 Participants were asked to choose a word from 4 options in the verification question. As a result, if a participant failed to select the item as instructed, they were removed from the survey and not included in the final analysis. The survey was accessed by 693 participants prior to the closing date. Among those who accessed the survey, n = 66 failed to progress beyond the demographic section, and n = 22 failed to pass the instructional verification question, leading to a final sample size of n = 605.
Theoretical Framework
The present study was developed using the PRECEDE-PROCEED framework. PRECEDE-PROCEED was selected because it includes a comprehensive framework for assessing community health needs in order to design, implement, and evaluate public health initiatives. 21 Specifically, this study adapted elements of phases 1 to 3 to guide the development of questions.
Prior to the development of the survey, a community advisory board (CAB) was convened. The CAB was composed of Black and Latinx individuals who lived and worked throughout the state of Indiana. Members of the CAB represented diverse backgrounds including a variety of educational experiences, first-generation U.S. residents, retirees, and individuals from the manufacturing and healthcare industries. During the CAB meetings, members discussed their personal experiences and opinions concerning HIV among people of color in Indiana. Using the PRECEDE-PROCEED framework to guide the conversation, the discussion resulted in the identification of key constructs related to the HIV continuum of care.
Following the identification of the salient constructs, the research team developed a preliminary survey instrument. A working draft of the survey was then disseminated to the CAB to solicit feedback and verify their perceptions and experiences were appropriately represented. Finally, the instrument was refined based on feedback, and returned to the CAB for approval, resulting in the final survey instrument.
Measures
Demographics
This survey included demographic questions regarding race/ethnicity, age, gender, sexual orientation, level of education, and relationship status of respondents. Educational attainment was measured using a 7-point scale, with items ranging from 1 = less than high school to 7 = doctoral degree. We evaluated sexual identity using a 5-item scale created for this survey (straight/heterosexual, gay/homosexual, lesbian, unsure/questioning). The gender of the participants was determined by asking a 4-item question (male, female, transgender, non-binary). As part of the study inclusion criteria, participants were asked to identify their race/ethnicity and were given 4 options (Black/African American/African Diaspora; more than 1 race including Black/African American/African Diaspora; Latin/Hispanic/Spanish; more than 1 race including Latin/Hispanic/Spanish).
PrEP literacy
PrEP literacy was assessed using a nine-item scale developed for this study. Seven of the 9 questions discussed common misconceptions about PrEP (eg, individuals who take PrEP are more sexually promiscuous, PrEP is only for men who have sex with other men). One question addressed the efficacy of PrEP by asking participants about the impact of inconsistent PrEP use. A final question explored perceptions of the cost of PrEP. Participants were asked to select 1 of 3 responses to the following question: PrEP is too expensive (true, false, depends on Insurance). PrEP literacy scores range from 9 to 18, with 9 representing the lowest level of PrEP literacy and 18 representing the highest level.
Sexual communication self-efficacy
Sexual health communication was measured using an adapted version of the Sexual Communication Self-Efficacy Scale (SCSES). 22 The SCSES includes 19 questions regarding the degree of difficulty with which participants discuss sexual health issues. Each question was evaluated using a 4-point scale ranging from 1 (very difficult) to 4 (very easy). The final score ranges from 19 to 76, with 19 indicating the lowest level of self-efficacy in sexual communication and 76 indicating the highest level. In the present study, the SCSES exhibited high internal consistency with a Cronbach’s alpha of .94.
Rurality
Rurality was measured using 1 question developed for this survey where participants were asked to enter the zip code of their primary residence. Each zip code was entered into the Am I Rural? tool and subsequently coded as either rural or non-rural. 23
HIV status
HIV status was measured using 1 dichotomous question developed for this study. Participants were asked to identify if they were aware of their HIV status (yes/no).
Analysis
The analysis was conducted in 2 phases. All data were first analyzed descriptively using univariate analysis. Second, a multivariable linear regression model was employed in order to examine the relationship between 5 independent variables and the dependent variable of self-efficacy in sexual health communication. A review of the test assumptions prior to analysis indicated a satisfactory level of normality, linearity, and homoscedasticity. Analyses were performed using Statistical Product and Service Solutions 27.
Results
Descriptive Analysis
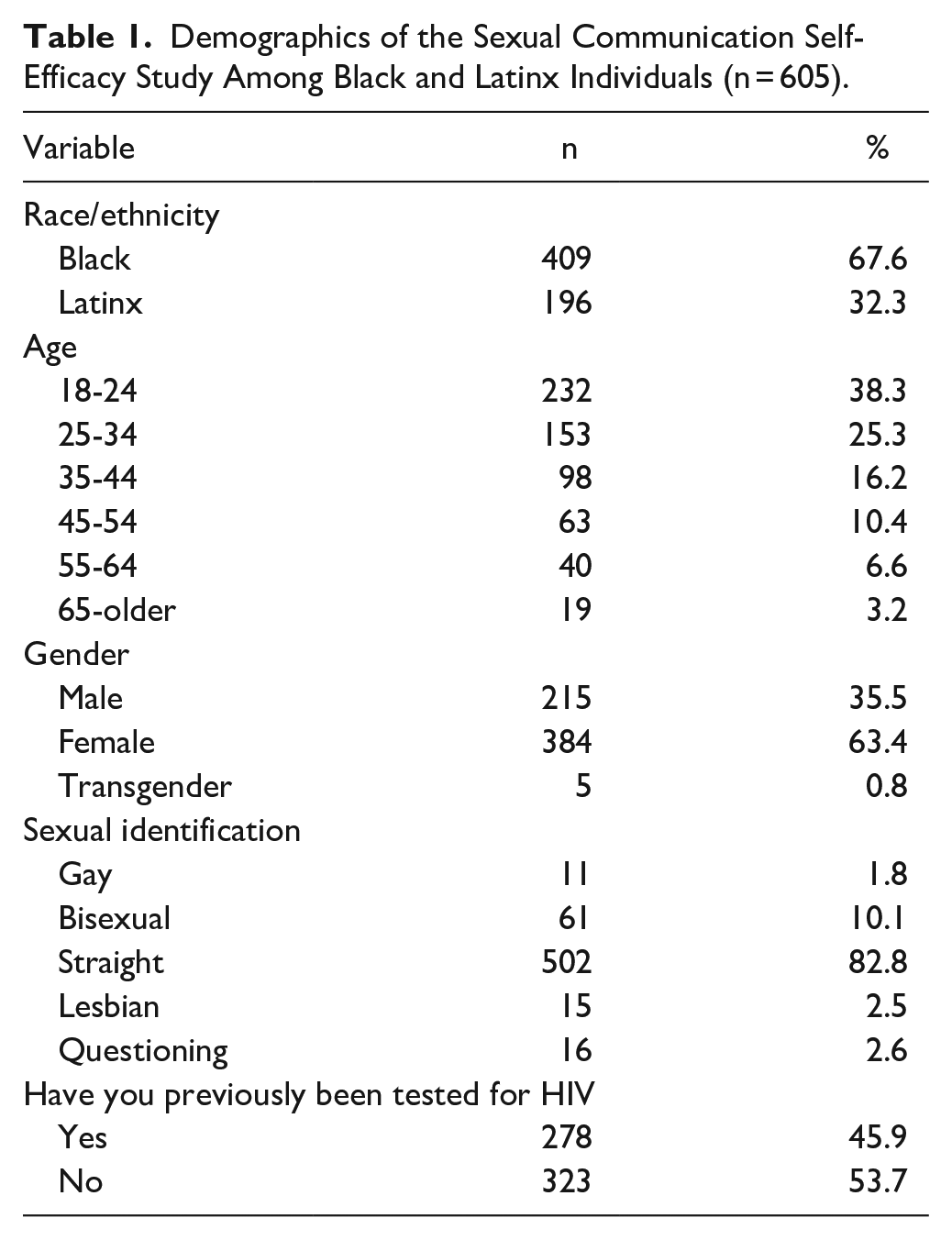
A majority of participants (n = 384, 63.4%) identified themselves as females, followed by 215 (35.5%) who identified as males. Five participants (0.8%) identified as transgender or gender non-binary. In total, 409 participants (67.5%) identified themselves as black, while 196 (32.3%) identified as Latinx. In terms of age, most were aged between 18 and 24 (n = 232, 38.3%) and 25 and 34 (n = 153, 25.2%). Regarding sexual identification, the majority identified as straight (n = 502, 82.8%) and 103 (17%) as LGBTQ. Among the respondents, the majority reported completing some college but no degree (n = 185, 30.5%), followed by a high school diploma (n = 171, 28.2%).
A majority of the participants exhibited a medium level of PrEP literacy (n = 374, 61.7%), followed by n = 65 (10.7%) who demonstrated a low level of PrEP literacy. 74.3% of participants (n = 450) reported living in a rural area, followed by 25.6% (n = 155) reporting living in an urban area. Sexual health communication self-efficacy scores ranged from 19 to 76, with a mean score of 59 and a median of 58. For a detailed description of the descriptive analysis, please refer to Table 1.
Demographics of the Sexual Communication Self-Efficacy Study Among Black and Latinx Individuals (n = 605).
Multivariable Analysis
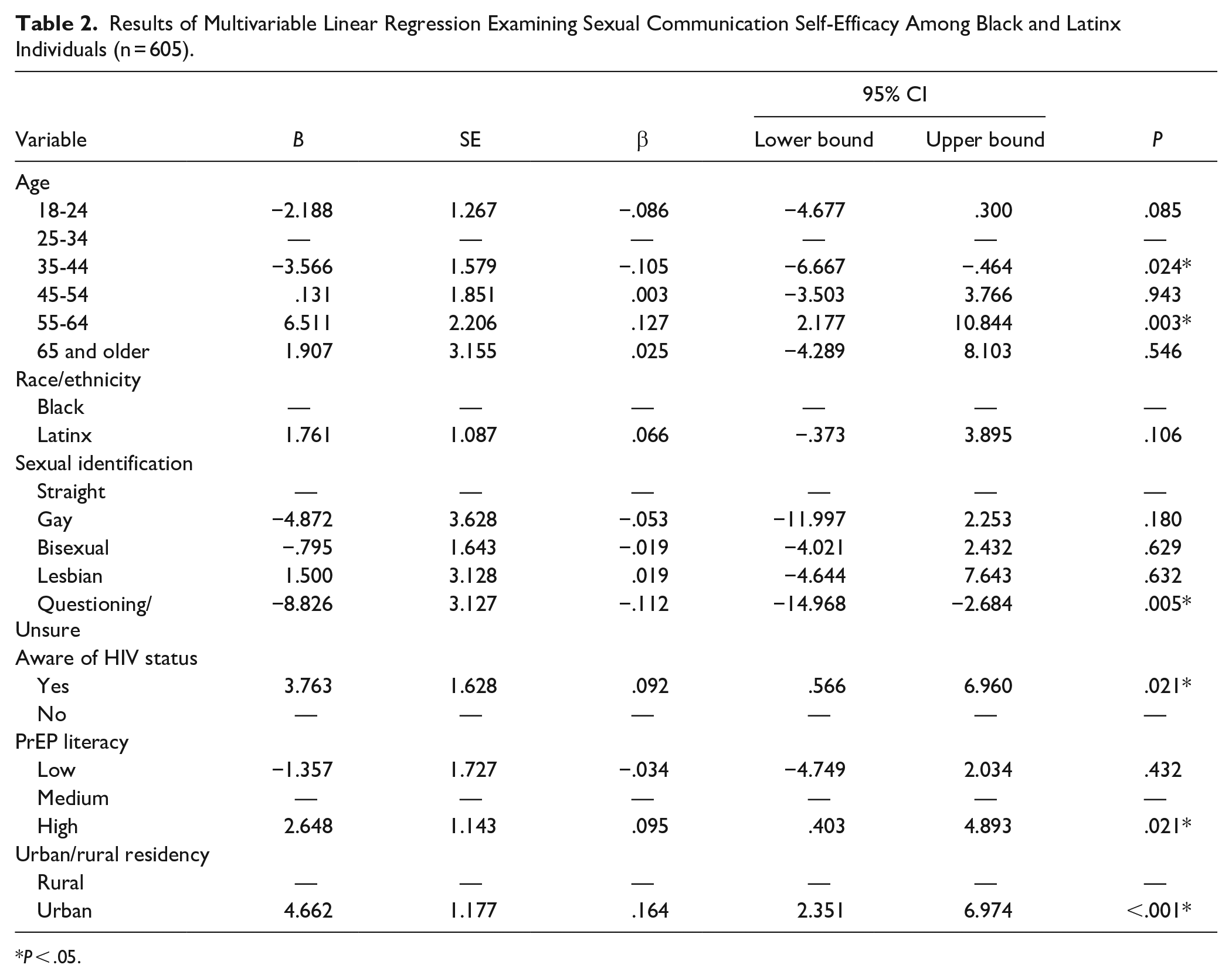
Table 2 presents a multivariable linear regression analysis examining scores reflecting sexual health communication self-efficacy. Results demonstrate the regression model was statistically significant (P < .001). Concerning predictor variables, participants with a higher level of PrEP literacy had a significantly higher level of sexual communication self-efficacy, in reference to those with a moderate level of PrEP literacy (B = 2.65, SE = 1.14, ® = .095, P = .021).
Results of Multivariable Linear Regression Examining Sexual Communication Self-Efficacy Among Black and Latinx Individuals (n = 605).
P < .05.
It was found that those who are unsure or question their sexual identification are significantly more likely to have a lower level of self-efficacy when it comes to communicating their sexual health (B = −8.83, SE = 3.13, β = −.11, P = .005). As compared to individuals who are unaware of their HIV status, those who are aware of their HIV status report significantly higher levels of sexual communication self-efficacy (B = 3.76, SE = 1.63, β = .09, P = .005).
Participants ages 35 to 44 were more likely to report a lower level of sexual communication self-efficacy in reference to those ages 25 to 34 (B = −3.57, SE = 1.27, β = −.11, P = .024). Conversely, those between the ages of 55 and 64 reported a higher level of sexual communication self-efficacy (B = 6.51, SE = 2.21, β = .13, P = .003). Finally, participants who live in urban areas demonstrated a significantly greater level of self-efficacy in the area of sexual health communication compared to participants who live in rural areas (B = 4.66, SE = 1.18, β = .16, P < .001). Rural residence was the strongest predictor variable in the model (β = .164).
Discussion
People of color continue to be adversely affected by HIV at a disproportionate rate, and despite recent advances in HIV prevention, PrEP use remains low among those most likely to benefit. Several factors have been identified in the literature as influencing lower PrEP uptake; however, the relationship between rurality, PrEP literacy, and sexual health communication among people of color has not been well explored. Most studies that examine HIV among people of color focus on urban areas and the Deep South but overlook the experiences of people in the Midwest and other moderately rural areas of the United States. Our study aimed to learn how rurality may affect sexual health communication, and the results suggest that living in a rural area can negatively affect an individual’s self-efficacy in sexual health communication.
According to our findings, residents in urban areas demonstrate significantly higher self-efficacy than those living in rural areas. This is in agreement with a prior study of HIV-negative MSM in rural and urban China which found that rural residents exhibited lower PrEP self-efficacy compared to urban residents. 24 This was attributed to several factors, including conservative ideology, insufficient access to health information, and a lack of confidence in engaging in healthy behaviors among participants from rural China. Additionally, this population reported higher levels of anxiety and depression overall, with anxiety negatively associated with PrEP efficacy. Further, age was a negative predictor of PrEP self-efficacy. With the use of educational interventions targeted at older adults, providers may be able to increase protective health behaviors and increased sexual health self-efficacy.
Conversely, when analyzing younger populations, different strategies may prove to be effective in rural populations. In a study of high school girls in a rural district in the south-eastern United States, social self-efficacy, sexual assertiveness, and sexual communication self-efficacy were positively associated. 14 Among girls currently in a relationship, social self-efficacy and communication frequency were directly related, even when controlling for sexual activity status. Considering that sexual communication is associated with healthy sexual behaviors, such as condom use, positive communication strategies, including sexual assertiveness and frequency of sexual communication with dating partners, should be targeted to improve self-efficacy among rural adolescents.
Participants who were unsure of their sexual identification had a lower self-efficacy compared with participants who confidently identified as “straight.” Uncertainty in one’s identity and poor self-concept can cause a lack of confidence in individual behavior; in fact, one of the strongest predictors for higher sexual self-efficacy scores is high self-esteem, even after controlling for demographic variables, knowledge of sexual risk, and previous coital experiences. 25 Self-esteem is an important prognosticator for determining HIV risk, as high self-efficacy is correlated to increased ability and effort made to adopt and maintain behavior and an increase in confidence in that behavior. 26 Confidence in behavior likely influences one’s willingness to avoid and refuse risky sex practices that could negatively impact their health.27-29
PrEP uptake and adherence in association with self-efficacy among communities of color is an important area of study. In a study of urban Chinese MSM, high PrEP adherence was associated with PrEP knowledge and confidence in PrEP efficacy of HIV prevention, indicating that increasing PrEP literacy has a positive impact on sexual self-efficacy. 30
The communication strategies employed by healthcare providers can impact how a patient interprets PrEP, and it represents a potential intervention point to increase confidence in safe sex practices and behaviors while concurrently dispelling stigma and increasing PrEP literacy. The most common communication barriers cited by patients are: (1) Poor engagement in non-judgmental, open-ended discussions about sexuality and sexual history; (2) Insufficient PrEP knowledge by providers and a need for patients to educate their own providers; (3) Lack of initiation by providers on conversations about PrEP; and (4) Worry about cost and lack of information about options for payment assistance. 31 Three out of 4 of these communication barriers are based in stigma and overall discomfort with discussing medical information about sexual health.
Improved communication about all facets of sexual health is a vital step in dismantling stigma around PrEP and HIV. Our study found that PrEP literacy is increased among patients reporting more contact with their provider, especially with PCPs who screen for HIV regularly. Respondents who utilize their PCPs are more confident accessing HIV services and are more able to discern fact from fiction around PrEP. PCPs who serve as a primary source of information may also serve as the patient’s sole, accurate source of sexual health education.
Awareness of HIV status is associated with higher self-efficacy compared to those who are unaware of their HIV status. Those participants who were aware of their HIV status also had some level of HIV and AIDS comprehension. Studies have shown that increases in AIDS-related knowledge bolster confidence in HIV preventative medicine. 32 Knowledge is a tool for participants to confirm accurate health beliefs and increase confidence in safe sex behaviors. Therefore, efforts by providers should be made to disseminate correct health information specifically to increase self-efficacy and confidence in positive sexual health behaviors.
PrEP is only efficacious if there is also widespread implementation of HIV testing. Until people are aware of their HIV status, these methods of expanding PrEP knowledge will not reach them because they will not be looking. In a study of 118 Spanish-speaking Latinx Gay men, Bisexual men, and other MSM, the most common barriers to accessing HIV testing were (1) not knowing where to get tested (35.6%), (2) not having health insurance (33.9%), (3) fear of being HIV positive (28.8%), (4) practicing safer sex and perceiving not needing to be tested (27.1%), and (5) not being recommended to get tested (22.0%). 33 Participant characteristics that were associated with enduring more barriers to HIV testing were those who were Spanish-only, unemployed, or adhered to more traditional notions of masculinity.
The study has some limitations, including the fact that the survey contains sensitive and personal questions that may have caused discomfort among participants, potentially affecting the truthfulness of their answers. Because of the cross-sectional nature of the study, we were only able to examine behaviors and attitudes at a single point in time, rather than a trend over time. The data were collected from Black and Latinx individuals who reside in Indiana; therefore, the results may not be applicable to persons of color living outside of Indiana, or individuals. The survey did also not assess sexual debut or sexual activity, potentially limiting the discussion concerning those factors. Finally, as a result of the limited scope of this study, the results are not generalizable to other populations. In addition, the study only looked at a limited number of variables that could potentially affect health outcomes. For example, we did not examine access to or quality of healthcare, which are important factors that can influence health. Future research should aim to address these limitations in order to provide a more complete picture of the determinants of health among Black and Latinx individuals.
Conclusions
Effective PrEP communication can only occur if PCPs are engaging patients in sex-positive dialog and creating a non-judgmental environment for disclosing sexual health concerns. HIV testing and PrEP counseling must incorporate culturally congruent approaches, such as hiring PCPs of color and using community leaders to encourage health interventions, including dispelling misconceptions and promoting safe sexual practices to ensure sustainable adherence to the PrEP regimen. Additionally, speaking Spanish-only generated the highest barrier to HIV testing, indicating that access must also incorporate improved bilingual approaches to raising awareness.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Indiana Minority Health Coalition.