
Abstract
Background:
Permanent Supportive Housing (PSH), which provides subsidies for independent housing and supportive services, is an evidence-based practice that improves health and housing for homeless experienced persons. Though most PSH is scattered-site, that is, housing dispersed throughout the mainstream rental market, project-based PSH offers housing and supportive services in dedicated facilities with on-site services. In 2013, the Veterans Health Administration (VA) at Greater Los Angeles opened a novel project-based PSH program located on a VA campus. To inform plans to expand project-based PSH at this VA, we examined participants’ experiences in this program. We aimed to identify participant characteristics that suggested they were well suited for the planned PSH expansion; to characterize services that participants found valuable in this setting; and to highlight gaps between participants’ needs and PSH services provided.
Methods:
We performed semi-structured interviews with a convenience sample (n = 24) of participants who had engaged in this project-based PSH program. Interviews asked why participants selected housing on a VA campus and explored valued program characteristics, designs, and services. Using rapid analysis methods, we generated templated summaries of each participant’s responses across the domains of our interview guide, then used matrix analyses to identify salient themes across the interviews.
Key Findings:
Participants appreciated the ease of access to medical and mental health services; however, as services were assumed to be optimized by virtue of co-location with VA healthcare, their PSH providers often did not link them with non-VA social services as assertively as desired. Many participants raised concerns about building safety and on-site substance use. A lack of participant engagement in program oversight, often leading to conflicts with staff and building management, was also highlighted in our interviews.
Discussion:
Given the value placed on ease of access to healthcare, these data suggest the value of this PSH model for persons with healthcare vulnerabilities. Specific recommendations for the planned PSH expansion include: (1) continuation of proximate, open-access healthcare; (2) clear tenant policies; (3) tenant councils for each development; (4) staff knowledgeable of non-VA resources and social services; (5) Veteran-preferred hiring practices by Property/Service management; (6) gender-specific accommodations; and (7) robust 24/7 security on-site.
Keywords
Introduction
Housing is a key determinant of health.1,2As such, the Veterans Health Administration (VA) is committed to ending Veteran homelessness, 3 with significant gains through its permanent supportive housing (PSH) initiative 4 : the Department of Housing and Urban Development-VA Supportive Housing (HUD-VASH) program. PSH is an evidence-based practice that improves housing outcomes for persons experiencing homelessness; it pairs subsidies for permanent, independent housing with supportive services.5,6 As a large healthcare system with an embedded PSH program, several VA facilities across the nation boast HUD-VASH units co-located with their medical centers; however, little is known about the perspectives and experiences of residents in these units.
The HUD-VASH program has clearly defined eligibility criteria and participant requirements; the program operates using well-established PSH principles. Specifically, HUD-VASH enrollment requires VA healthcare eligibility, current or threatened homelessness, HUD-determined income requirements, and the ability to live independently with supportive services. 7 Participants devote 30% to 40% of their monthly income to rent and the remainder is subsidized. These subsidies are offered in either of 2 PSH paradigms: “scattered-site” (92% of HUD-VASH units), that is, private market rentals in the general community; and “project-based” (8% of HUD-VASH units, including those on VA campuses), which are located in specific buildings designated at least in part for HUD-VASH, typically with on-site case management. 8 Both HUD-VASH paradigms employ the Housing First model, with all participants receiving field-based case management and non-mandated linkages to care.9,10
The VA Greater Los Angeles (VAGLA) has the nation’s largest HUD-VASH program (n = 7358 participants). In 2013, VAGLA opened 2 multi-unit project-based PSH buildings on one of its campuses, with plans to build ~1200 additional rental units on its tertiary medical center campus over the next decade. 11 There were several key reasons for this expansion. First and foremost, in large urban communities, there is a dearth of affordable housing, and the tertiary medical center is situated on land that could be devoted in part to PSH. Second, data suggest that HUD-VASH participants have high rates of healthcare utilization (inpatient, outpatient, and emergency medical services) 12 ; as such, co-locating HUD-VASH with a VA medical center can enable realized access to a breadth of health services.
Yet, though plans to expand HUD-VASH at VAGLA are actively underway, fundamental questions about this plan remain unanswered: Which participants are best served by this co-located housing? What program characteristics, designs, and services are most beneficial to participants? To address these questions and inform program planning, we used qualitative interviews to glean the perspectives and experiences of residents in the current on-campus buildings.
Methods
Setting
At present, VAGLA has 3 co-located HUD-VASH buildings: 2 (149 units) at a suburban, ambulatory care VAGLA site described here; and 1 (54 units) at the tertiary medical center. These buildings are first steps in dramatically expanding VAGLA-based HUD-VASH.
Participants
We obtained a roster of current and formerly housed Veterans in the first 2 project-based buildings (n = 702). We used phone calls and letters to invite a random sample of 49 Veterans for semi-structured interviews. Most remained housed in the program; some had exited prior to this data collection. We interviewed 24 Veterans prior to reaching data saturation. 13
Data Collection
Semi-structured interviews (~30 minutes each) were conducted by one author (H.W.), a doctoral-level social worker. The interview guide was developed collaboratively with VAGLA homeless program leadership to support plans for on-site HUD-VASH expansion. To ascertain which participants are best suited for housing in this setting, we asked participants why they selected housing on a VA campus. To understand what program characteristics and services would be most beneficial to future participants, we explored services that participants utilized and asked about program characteristics perceived to support or impede housing retention. We also asked about unmet needs that could influence housing retention, inquired about changes in participants’ informal (families, friends) supports since moving into HUD-VASH, and sought general feedback to improve experiences with HUD-VASH co-located with the VAGLA campus. The data collection was deemed quality improvement by the VAGLA Institutional Review Board (IRB) administrator; all participants provided verbal informed consent for project participation. Of note, under this quality improvement determination, we were not able to collect data on participants’ demographic and clinical characteristics.
Data Analysis
Interviews were audio-recorded and professionally transcribed. Two authors (M.N. and J.P.) developed a template derived from our interview questions. Applying rapid turn-around qualitative methods, 14 they independently used this template to develop structured summaries of 3 interviews to ensure consistent use of template categories. They worked iteratively with additional authors (H.W., A.R., S.G.) to refine the template, applying the finalized template to each interview transcript. Matrix analyses 15 and constant comparison 16 were used to identify widely-held perspectives on strengths and weaknesses of HUD-VASH experiences on the VAGLA campus, with a lens towards informing the expansion of VAGLA campus-based HUD-VASH.
Results
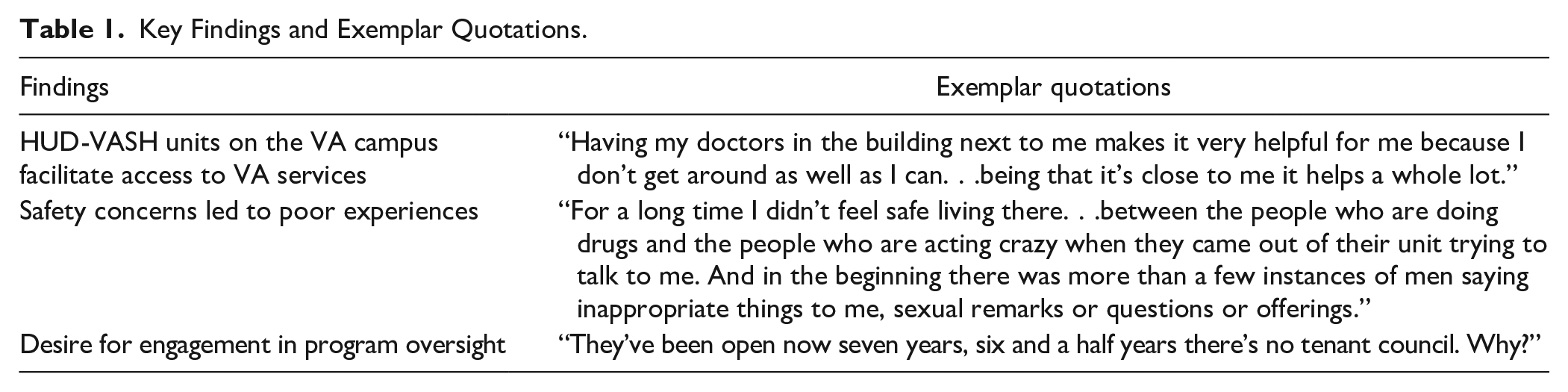
We had 3 salient findings from these interviews that may aid with program planning, summarized in Table 1 and detailed further below. First, participants appreciated the ease of access to VA services that comes with PSH co-located on a medical center. However, participants expressed safety concerns, largely related to behavioral health problems among residents in these buildings. Last, participants valued engagement in program oversight and desired more involvement along these lines.
Key Findings and Exemplar Quotations.
HUD-VASH Units on the VA Campus Facilitate Access to VA Services
Nearly all participants identified ease of access to VA healthcare as the salient benefit of living on the VA campus. Participants valued timely access to their providers and easily getting to their appointments. One participant described that moving on campus facilitated linkages with a primary care team tailored for homeless Veterans that offered rapid access to comprehensive care. As he described, “When I first came here, they wanted me to wait six months to see a doctor. And then I came [to see the homeless primary care team] . . . and I got seen in two weeks.” Participants with chronic medical conditions highlighted that living near their healthcare teams improved their overall sense of wellness and safety. As one participant stated, “I know I’m safe here. It’s an ambulatory care center [and] I have mild heart disease. . . I have diabetes. . . All of the opportunities to get [care] fast are here on campus.”
Despite easy access to VA healthcare services, some participants noted suboptimal linkages to social services, particularly those offered outside the VA. Often, participants desired referrals to social services in the community, but felt that staff did not effectively facilitate use of these services. As one participant described, “Not having information was what held me back a lot of times. There were things available to me that I didn’t know were available to me and even [my case manager] didn’t seem to know. . .So that just kind of comes back to the lack of information. I just didn’t know what was out there.”
Safety Concerns Led to Poor Experiences
Many participants lived at this site because of its low barriers to housing placement. In turn, participants viewed their peers as often suffering from behavioral dysregulation, substance use, or criminal justice involvement. As such, many participants voiced concerns surrounding safety, primarily in 3 domains: substance abuse, physical violence, and sexual harassment. One participant expressed concerns about drug use in the building negatively affecting his recovery from substance abuse, describing that: “I can get any kind of drug I want here; heroin, cocaine, speed, acid. It’s been offered to me.”
Compounded by peers’ visible mental health symptoms, many participants cited feeling unsafe in the building’s common spaces. As one participant said, “I don’t want to have anything to do with them. . . they’re on speed and they’re on drugs. . . I just stay away from them.” Another noted, “There’s a lot of real dangerous people that don’t know how to channel their problems correctly. . . so they take their anger out on innocent people and it really isn’t a healthy environment.” Other participants described issues with physical safety, feeling threatened by other tenants. As one participant described, “I’m disabled and I have a prosthesis. I’ve been slapped around in my chair. . . I’m disabled and I’m easy prey.”
Female participants highlighted a need to ensure women’s safety. They reported sexual harassment from other tenants and desired gender-specific additional safety precautions. One participant noted, “The situation about the sexual harassment. . .how many of those women are living on VA benefits that have to do with military sexual trauma. . .they bring in an extra security guard so the women [on] staff feel safe but he leaves at 5:00.”
Desire for Engagement in Program Oversight
Many participants described building management as ill-informed about residents’ experiences and interests, resulting in tension and unmet needs. Participants also cited a lack of clarity around building policies, causing frustration and conflicts with management. One participant described, “If the rule comes—you do something wrong [and] they make a rule for it right then and there.” Some participants felt that those who shared their lived experiences were best-suited to manage the building. As one participant noted, “Why not find Veterans to run it? Professional Veterans in this field? That’s what I would do.”
Overwhelmingly, participants did not feel engaged in their building’s oversight and desired increased resident advocacy, potentially through a resident council. One participant posited, “I think that the Veterans should have [their own] committee that [residents can] go [to] instead of the manager. . .there should be a set process for grievances instead of going to a counselor and the next counselor above [being] the one that decides. . .there should be a set process for, hey, this isn’t working.”
Discussion
We gathered participant perspectives about a current project-based HUD-VASH program on a VA campus to inform plans for large-scale expansion of HUD-VASH at this VA. Ease of access to healthcare services was a key program benefit, though many participants expressed safety concerns and desired greater engagement in building oversight.
Not surprisingly, participants emphasized ease of access to health services as the primary advantage of living on a VA campus. As homeless experiences are highly correlated with acute and chronic health problems, 17 paradigms that enhance access to care are important. Prioritization of the most vulnerable is a tenet of the Housing First model used by HUD-VASH, which may contribute to the value participants attributed to improved access to care. 18 Participants’ appreciation regarding ease of access to physical and mental health services suggests that persons with high healthcare needs, and/or difficulty accessing services, should be prioritized for VA-based housing. As social service referrals, especially outside VA, were described as suboptimal in a setting where access to care was presumed, these data suggest the importance of educating VA-based HUD-VASH staff about key community resources.
Many participants expressed safety concerns despite on-site security; this finding highlights the delicate balance between providing low barrier housing and ensuring safety. Some literature supports mixed-population housing (co-locating residents across socio-economic statuses and vulnerabilities) as a way to increase housing quality and safety; others argue that this model lessens housing opportunities for the most vulnerable. 19 Regardless, our interviews highlight the importance of well-developed safety practices for a highly vulnerable population. The concerns expressed by female participants may be exacerbated by the VA context; >50% of homeless female Veterans experienced military sexual trauma and most HUD-VASH participants are male.20,21 Gender-specific accommodations, for example, female only hallways, may improve the well-being of female residents.
Concerns about resident engagement in building oversight were important. Difficulty complying with HUD-VASH policies is a barrier to housing retention. 22 Among persons with homeless experiences, perceived autonomy is associated with improved motivation to maintain positive outcomes. 23 In assisted living facilities, resident councils increase perceived autonomy by engaging residents in decisions impacting their daily lives. 24 Employing individuals who share lived experiences with residents may also increase engagement while bridging the disconnect between residents and staff. Such “consumer providers” are widely used within and outside the VA, and have been found to increase trust and engagement over traditional staff.25,26 Moreover, clear and consistent program policies and goals, refined in an iterative and collaborative process, were desired by participants.
This project has limitations. PSH programs co-located with medical centers are rare. As a single case study, these findings may not extrapolate outside VA, or to VA populations in different settings. As we interviewed a convenience sample, the perspectives described may not reflect all participants in the initial HUD-VASH buildings at VAGLA. Moreover, participants with strong viewpoints about the VA-based HUD-VASH program may have been more likely to volunteer for interviews, potentially resulting in skewed data.
Conclusions
Characterizing participant experiences and perspectives in different PSH models is important to facilitate quality improvement and program planning. Given the limited supply of PSH units—particularly in tight rental markets—it is critical to understand participant characteristics (eg, healthcare need or access barriers) that suggest a good fit for a given housing model and setting. Moreover, it is important to identify unmet needs in PSH settings and to learn how to optimize participant experiences. Our findings are highly relevant for VAGLA’s plan to develop significantly more HUD-VASH units on its tertiary medical center campus. We found that individuals with significant mental and physical health morbidities are likely to benefit the most from collocated PSH. Specific recommendations for future expansion of this housing model include: (1) continuation of proximate, open-access healthcare; (2) clear tenant policies; (3) tenant councils for each development; (4) staff knowledgeable of non-VA resources and social services; (5) Veteran-preferred hiring practices by Property/Service management; (6) gender-specific accommodations; and (7) robust 24/7 security on-site.
Additional data collection would further inform these efforts, including eliciting clinician and staff perspectives, and assessing health and social outcomes among program participants, for example, health service utilization, housing retention, and community integration. Improvement trials of interventions suggested by these interviews, for example, resident councils, may be valuable as VAGLA’s expansion plans are implemented.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received funding from a VA RR&D Research Enhancement Award Program (REAP) on Enhancing Community Integration for Homeless Veterans (PI: Green) pilot award (pilot PI: Reddy).