
Abstract
Introduction/Objectives:
The prevalence of thyroid disorders is high in Saudi Arabia. Among the disorders, goiter and thyroiditis are the most common and have unique ultrasound (US) features, underscoring the need for US screening for thyroid pathologies. This study aimed to determine the prevalence of thyroiditis and thyroid nodules in patients attending the Family and Community Medicine Center of Imam Abdulrahman Bin Faisal University.
Methods:
This registry-based cross-sectional study analyzed laboratory and US data from 240 patients who attended the Family and Community Medicine Center of Imam Abdulrahman Bin Faisal University from January 2020 to December 2021. Abnormalities of the thyroid gland were categorized according to laboratory and US data. Associations between different types of thyroid pathology and clinical and laboratory findings were assessed using appropriate statistical methods.
Results:
The majority of participants were Saudi women. The prevalence of thyroiditis in the study population was 43%. Approximately 25% of these patients had more than 1 nodule, and fine-needle aspiration biopsy showed that most nodules were benign. Most nodules were found in clinically euthyroid patients. Thyroiditis might be associated with abnormal thyroid function.
Conclusions:
Thyroiditis and thyroid nodules were common in our cohort. Vitamin D deficiency, other autoimmune diseases, and a family history of thyroid disorders were associated with thyroiditis and thyroid nodules. US is useful for identifying the type of thyroid disease.
Introduction
Thyroid diseases are highly prevalent worldwide and are a major health problem. 1 Thyroid diseases are the most common endocrine disorders in Saudi Arabia and other Arab countries. 2
Goiter is the most common thyroid disease. Clinical manifestations and thyroid hormone levels vary depending on disease etiology and the presence of cancerous tissues, which are found in up to 15% of patients with goiter. This high prevalence underscores the need to screen goiter patients for thyroid cancer.3,4
Thyroiditis comprises a diverse group of disorders and is classified as painless or painful. Thyroid hormone levels range from hyperthyroidism to hypothyroidism spectrum during the disease progress until it eventually normalizes in most cases. 5 Hashimoto’s thyroiditis (HT) is the most common form of painless thyroiditis. The most frequent cause of hypothyroidism in the United States is HT. 6 Thyroid peroxidase antibodies (TPOAb) and thyroglobulin antibodies (TgAb) are sensitive serological markers of HT. Moreover, there is a significant correlation between TPOAb levels and the ultrasound (US) features of HT.7,8
A palpable thyroid nodule is a common presentation affecting around 7% of people and is associated with cancers in 20% of cases.9,10 US is an invaluable tool for predicting malignant thyroid nodules. 11 Therefore, thyroid US is an important tool for evaluating patients with varying thyroid pathologies. 12 Nevertheless, few studies have evaluated the diagnostic utility of US for thyroid disorders in primary healthcare settings.
Considering the high incidence of thyroid disorders in Saudi Arabia, it becomes imperative to explore this matter. The aim of conducting such a registry-based study is to gain true access to the frequency of thyroid disorders among Saudis and non-Saudis living in the area and its associated data. Hence, the objective of this study is to determine the frequency of thyroiditis and thyroid nodules detected by ultrasound scans among our study population of patients attending the Family and Community Medicine Center (FAMCO) in Imam Abdulrahman Bin Fasial University (IAU) and its associated clinical and laboratory data
Methods
This registry-based cross-sectional study analyzed laboratory and thyroid US data from all patients who attended the Family and Community Medicine Center of Imam Abdulrahman Bin Faisal University in the period January 2020 to December 2021.
Family and Community Medicine Center
The Primary Health Care Center of Imam Abdulrahman Bin Faisal University, located in Dammam City, in the Eastern province of Saudi Arabia, has a fully functioning radiological department that serves university faculty, staff, and their family members, as well as local residents.
Laboratory and imaging data were retrieved from medical records using Quadrimed_2019_prog_Stes medicals software.
Study Population
A total of 240 adult patients who underwent US examinations between January 2020 and December 2021 were enrolled. These patients were referred to the radiology department of our center and, if necessary, to the pathology, endocrinology, and surgical departments of King Fahd Hospital of Imam Abdulrahman Bin Faisal University.
Data Collection
Demographic data, medical history, thyroid US features, and the results of thyroid function tests and fine-needle aspiration biopsy (FNAB) were obtained from medical records.
Data Management and Analysis
Thyroiditis was considered according to the heterogenous pattern of the thyroid gland on US. The patients with free triiodothyronine (FT3) levels of 1.71 to 3.71 pg/ml, free thyroxin (FT4) levels of 0.70 to 1.48 ng/dl, and thyroid-stimulating hormone (TSH) levels of 0.35 to 4.94 µIU/ml were considered euthyroid. Hypothyroidism was considered FT3 or FT4 levels below this range or TSH levels above this range, whereas hyperthyroidism was considered FT3 or FT4 levels above this range or TSH levels below this range. The presence of vitamin D deficiency (plasma 25-hydroxy vitamin D level of less than 12 ng/ml) and comorbidities (autoimmune, hematologic, or psychiatric diseases) were assessed within 12 months before or after the thyroid US.
Patients with neck swelling, hoarseness, compression of the esophagus and/or trachea, or dysphagia were subjected to US examinations. Patient concern is upon patient request or a known case of thyroid pathology diagnosed in another center and followed up.
The data were analyzed using SPSS version 21.0. The significance level was set at P < .05. Categorical data were presented as numbers and percentages. Associations between thyroiditis or thyroid nodules and potential risk factors were assessed using the chi-square test and Z-test for proportions in cases of multiple responses. The odds ratio (OR) and 95% confidence interval (CI) were calculated for significant associations.
Two multiple logistic regression models were used to identify demographic and clinical characteristics independently associated with thyroiditis and thyroid nodules. The enter method was used, and adjusted ORs and 95% CIs were measured.
The accuracy of the clinical diagnosis of goiter by family physicians was evaluated using US as the gold standard. The following parameters were calculated based on the number of true positives (TP), true negatives (TN), false positives (FP), and false negatives (FN): sensitivity (TP/TP + FN), specificity (TN/TN + FP), positive predictive value (PPV; TP/TP + FP), negative predictive value (NPV; TN/TN + FN).
Results
A total of 240 patients were enrolled in the study. The median age was 37 (10-92) years, and 57.5% of the cohort were aged 20 to 40 years. The majority (85.4%) of the patients were women, 6% were pregnant, and 15.1% had given birth or had a miscarriage within 12 months before thyroid US examinations. At presentation, 53.8%, 29.2%, and 15.0% of the cohort were euthyroid, hypothyroid, and hyperthyroid, respectively. Our population was referred for US examination because of the presence of symptoms (38.8%), abnormal levels in thyroid function tests (36.3%), and patient request (25%).
The analysis of demographic and laboratory data according to the presence or absence of US features of thyroiditis is shown in Table 1. Almost 43% of the patients had thyroiditis based on US features, and these features were more common in women (OR, 2.46; 95% CI, 1.10-5.53). There was no significant association between thyroiditis and pregnancy or childbirth within 12 months before US examinations. Of those with thyroiditis, 80.6% were Saudi nationals. The risk of thyroiditis was higher in hypothyroid patients (OR, 5.14; 95% CI, 2.74-9.64) and hyperthyroid patients (OR, 4.02; 95% CI, 1.84-8.78) than in euthyroid individuals. The size of the thyroid gland was normal in 66% of the patients with thyroiditis. The risk of thyroiditis was higher among those with 1 enlarged lobe (OR, 4.06; 95% CI, 1.59-10.37) and those with diffuse enlargement of the gland (OR, 4.22; 95% CI, 1.75-10.16). With regards to laboratory results, the risk of thyroiditis was higher in hyperthyroid patients (OR, 4.28; 95% CI, 1.14-16.06) and lower in hypothyroid patients (OR, 0.64; 95% CI, 0.18-2.20) according to FT3 levels. Furthermore, the risk of thyroiditis was higher in patients with low TSH (OR, 5.52; 95% CI, 2.57-11.86) and high TSH (OR, 6.69; 95% CI, 3.08-14.52) than in patients with normal TSH levels (Table 1).
Association Between Ultrasonographic (US) Features of Thyroiditis and Personal and Laboratory Characteristics of Patients in the Family Medicine Center, Saudi Arabia (January 2020-December 2021) (N = 239).
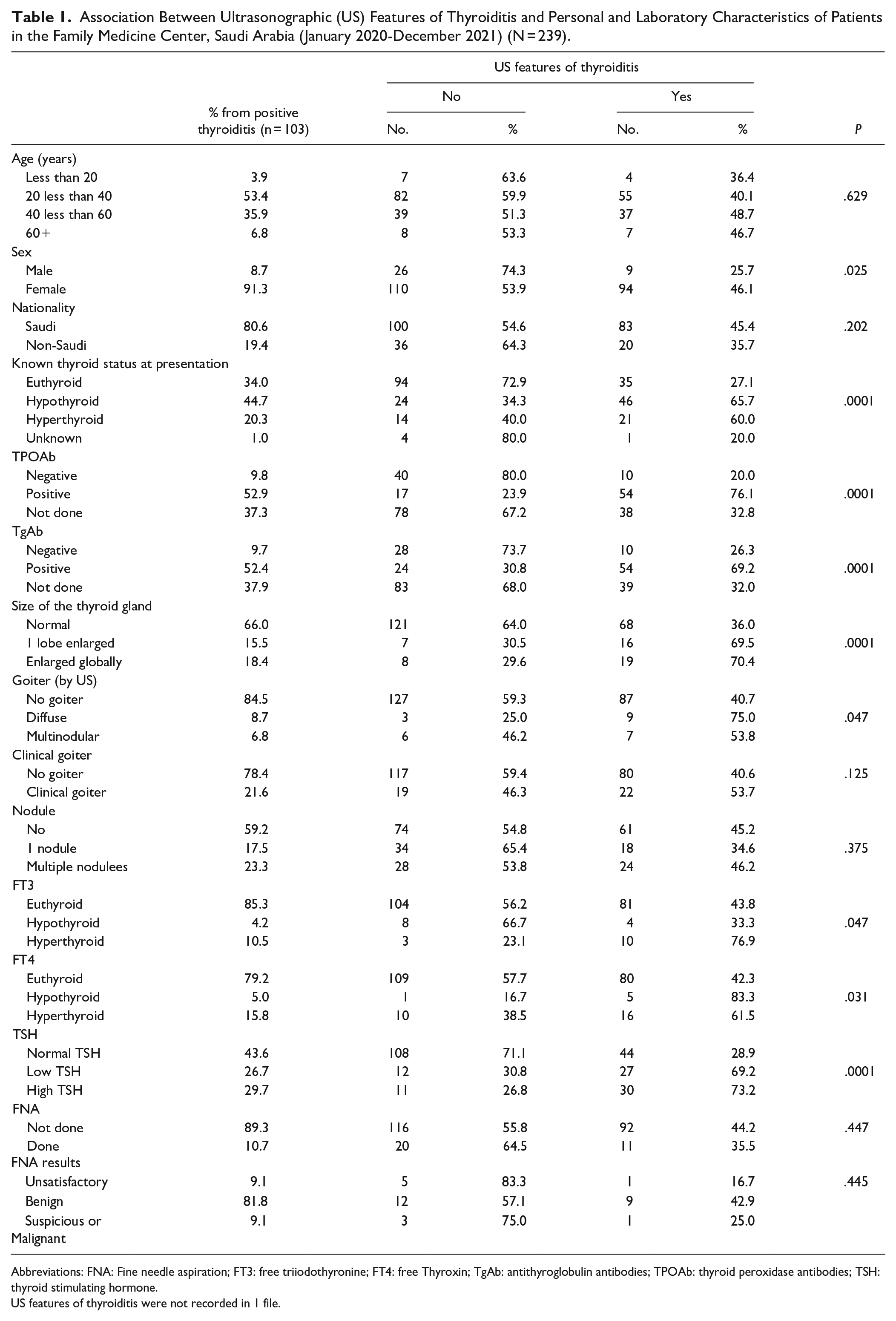
Abbreviations: FNA: Fine needle aspiration; FT3: free triiodothyronine; FT4: free Thyroxin; TgAb: antithyroglobulin antibodies; TPOAb: thyroid peroxidase antibodies; TSH: thyroid stimulating hormone.
US features of thyroiditis were not recorded in 1 file.
Among patients with US features of thyroiditis, 17.5% had 1 nodule, and 23.3% had more than 1 nodule. FNAB was performed in 11 patients with thyroid nodules; of these, 1 case was suspicious, 9 cases were benign, and 1 patient had unsatisfactory results (Table 1).
Goiter was detected clinically in 41 patients (17.2%) and ultrasonographically in 25 patients (10.4%). The accuracy, sensitivity, specificity, NPV, and PPV of the clinical diagnosis of goiter using US as the gold standard were 90.3%, 87.5%, 90.7%, 98.5%, and 51.2%, respectively.
Nodules were detected in 104 (43.3%) patients; of these, almost 50% had 1 nodule, and the remaining patients had multiple nodules. Nodules were located unilaterally in 96% of cases and bilaterally in 3.9% of cases. The nodule size was >1 cm in 73 (71%) of patients. The nodules were solid, cystic, or mixed in 56.4%, 17.8%, and 24.8% of cases. The nodules had a heterogeneous pattern in 66.3% of patients. The US pattern was hypoechoic, isoechoic, hyperechoic, mixed, or anechoic in 23.8%, 14.0%, 10.0%, 49.5%, and 3.0% of cases.
The analysis of clinical data according to the presence or absence of US features of thyroiditis is shown in Table 2. The risk of thyroiditis was higher among participants with vitamin D deficiency (OR, 5.75; 95% CI 2.10-15.72) and those with comorbidities (autoimmune diseases and iron deficiency anemia) diagnosed within 12 months before or after the diagnosis of thyroiditis (OR, 3.07; 95% CI, 1.63-5.78). Moreover, a family history of thyroid diseases significantly increased the risk of thyroiditis (OR, 4.93; 95% CI, 2.83-8.59).
Association Between Ultrasonographic Features of Thyroiditis and Clinical Characteristics of Patients in the Family Medicine Center, Saudi Arabia (January 2020-December 2021) (N = 239).

1 patient may have more than 1 answer.
% calculated from positive comorbidity.
Autoimmune: varied cases of systemic lupus erythrematosis, rheumatoid arthritis, Type 1 diabetes mellitus, Graves’ disease, Multiple sclerosis, Vitiligo. Psychiatric disorders: anxiety, depression, 1 patient with schizophrenia. Others: malignancy (breast, nasopharynx, pituitary), neurological (trigeminal neuralgia, migraine, disc prolapse), dermatological (acne vulgaris, urticaria), irritable bowel syndrome.
Others: Malignancy (leukemia, breast), Osteoporosis, Migraine, Fatty liver.
The analysis of demographic, laboratory, and imaging data according to the presence or absence of thyroid nodules is shown in Table 3. The number of nodules was higher in older patients. The risk of developing nodules was lower among men (OR, 0.40; 95% CI, 0.17-0.89). In addition, 67.3% of patients with nodules were euthyroid at presentation. The risk of nodules was lower in hypothyroidism (OR, 0.38; 95% CI, 0.20-0.71) and hyperthyroidism (OR, 0.37; 95% CI, 0.16-0.81) than in euthyroidism before adjusting for potential confounders. Goiter was not diagnosed clinically in 74.8% of patients with nodules. However, the risk of nodules was higher in the group with goiter (OR, 2.72; 95% CI, 1.35-5.46]). The majority of patients with nodules were euthyroid based on FT3, FT4, or TSH levels.
Association Between Thyroid Nodule(s) and Personal and Laboratory Characteristics of Patients in the Family Medicine Center, Saudi Arabia (January 2020-December 2021) (N = 240).
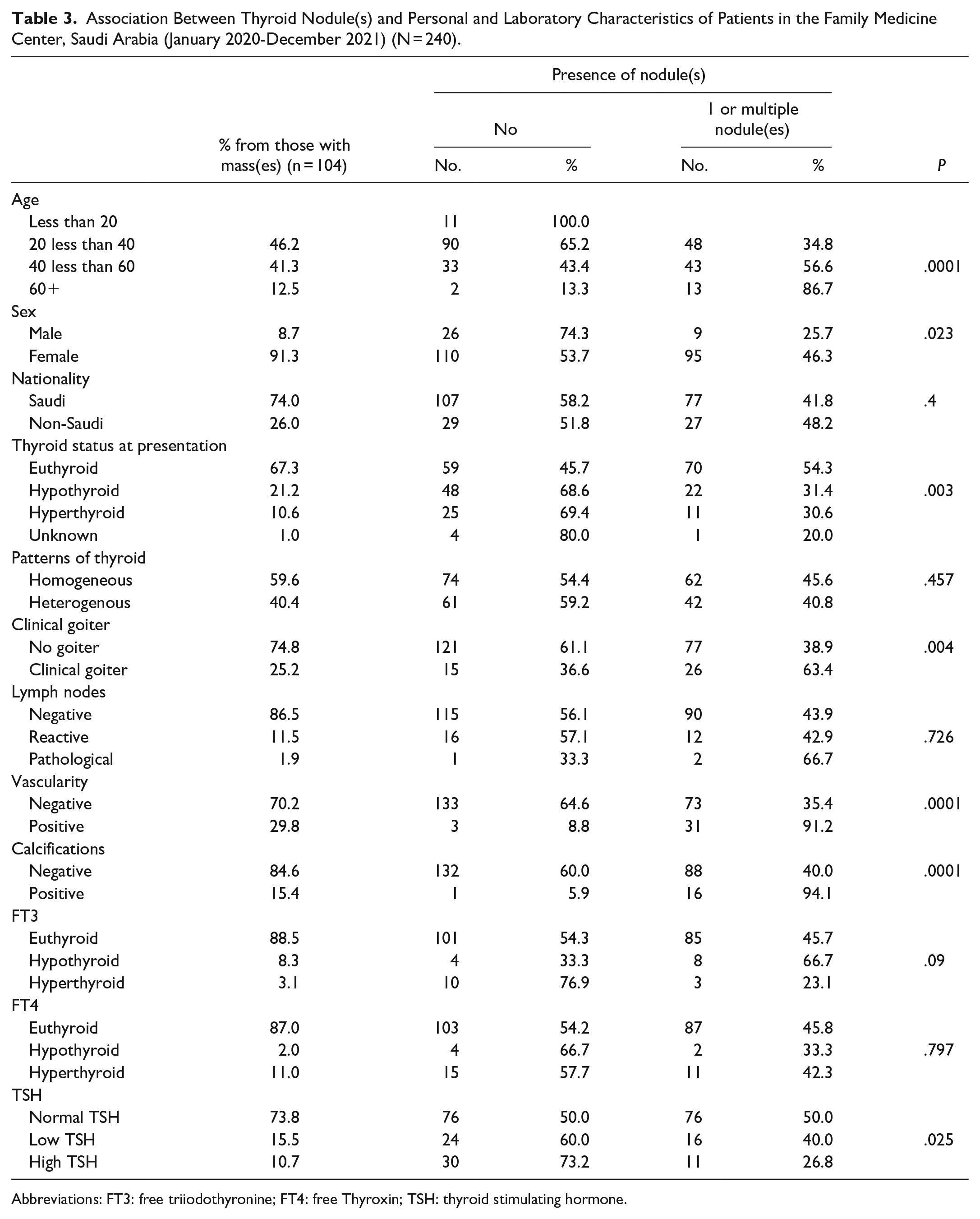
Abbreviations: FT3: free triiodothyronine; FT4: free Thyroxin; TSH: thyroid stimulating hormone.
Four Saudi women had malignant thyroid nodules based on FNAB results (2 aged 20-39 years and 2 aged 40-59 years); of these, 2 patients were euthyroid, 1 was hypothyroid, and 1 case was unknown. Four patients had a normal-sized thyroid gland on US, and 2 were clinically diagnosed with goiter. The thyroid pattern was homogenous in 3 cases and heterogeneous in 1 case. One patient had no nodules, 2 had 1 nodule, and 1 had 3 nodules larger than 1 cm. The nodule was solid in 2 cases and mixed (solid and cystic) in 1 case. Pathological lymph nodes were present in 1 patient. An increase in vascularity in 1 patient and all were negative for calcification.
The analysis of vitamin D status and comorbidities according to the presence or absence of thyroid nodules is shown in Table 4. Autoimmune diseases, diabetes mellitus type 2, hypertension, iron deficiency anemia, vitamin D deficiency, and a family history of thyroid diseases were associated with the presence of thyroid nodules.
Association Between Thyroid Nodule(s) and Clinical Characteristics of Patients in the Family Medicine Center, Saudi Arabia (January 2020-December 2021) (N = 240).

1 patient may have more than 1 answer.
% calculated from positive comorbidity.
Autoimmune: systemic lupus erythrematosis, rheumatoid arthritis, Type 1 diabetes mellitus, Graves’ disease, Multiple sclerosis, Vitiligo. Psychiatric disorders: anxiety, depression, 1 patient with schizophrenia. Others: malignancy (breast, nasopharynx, pituitary), neurological (trigeminal neuralgia, migraine, disc prolapse), dermatological (acne vulgaris, urticaria), irritable bowel syndrome.
Others: Malignancy (leukemia, breast),Osteoporosis, Migraine, Fatty liver.
The results of logistic regression analysis suggest that the risk of thyroiditis was higher in patients with an enlarged thyroid gland, autoimmune diseases, vitamin D deficiency, and a family history of thyroid disorders. The risk of developing thyroid nodules was higher in patients with iron deficiency anemia, autoimmune diseases, hypertension, vitamin D deficiency, and a family history of thyroid disorders. The risk factors for developing thyroiditis and thyroid nodules are presented in Table 5.
Logistic Regression Models for Personal and Clinical Predictors Associated With Thyroiditis or Thyroid Nodule(s) Among Patients in the Family Medicine Center, Saudi Arabia (January 2020-December 2021) (N = 240).

Discussion
Although different types of thyroid disease are being diagnosed and treated, benign thyroid diseases are more prevalent in Saudi Arabia and other countries.13,14
Thyroid diseases are managed medically and surgically. Thyroiditis was highly prevalent among female Saudi nationals who tested positive for autoantibodies in our study. These are some of the known associations of autoimmune diseases in general and autoimmune thyroid diseases specifically. 15 Most of these conditions are benign and self-limiting and require treatment only when associated with hypo- or hyperthyroidism.15,16 Association between US echogenicity of the thyroid and thyroid functions has rarely been reported before. 17 Patients with thyroid dysfunctions in our study were more likely to have US features of thyroiditis, consistent with a previous study. 18 Using heterogeneity of the thyroid gland pattern on the scan as an indicator of thyroiditis, an inflammatory process of the thyroid gland, has been reported in other international studies with other markers such as US echogenicity and Doppler US have been used to differentiate acute from subacute thyroiditis.17,19 These techniques are useful to detect thyroid pathologies but may vary across regions according to the level of experience of radiologists and the methods adopted for analyzing and reporting US results. Our radiologist was an experienced radiology consultant certified in the United Kingdom with more than 10 years of experience in thyroid US.
The risk of thyroiditis in our study was higher among patients with vitamin D deficiency. There is a correlation between vitamin D deficiency and autoimmune thyroiditis, especially HT, and other autoimmune diseases, including systemic lupus erythematosus and rheumatoid arthritis, suggesting that vitamin D plays a major role in immune regulation.20 -22 Moreover, vitamin D deficiency is closely related to higher levels of thyroid peroxidase antibodies, especially in HT. 23 Autoimmune thyroid diseases are characterized by enlargement of the thyroid gland, 24 consistent with our findings.
The prevalence of goiter is high worldwide but has decreased significantly after implementing salt iodization programs.25,26 The high accuracy of the clinical diagnosis of goiter by primary care physicians in our study using US as the standard demonstrates the adequate training of these professionals. Similar results have been reported in other studies that advocated the ability of family physicians to clinically diagnose goiter and thyroid gland enlargement. 27
The prevalence of thyroid nodules in our study was more than 40%, and US allowed assessment of the nodule size, location, number, pattern, margins, echogenicity, and acoustic transmission. Furthermore, other features were examined by the radiologist in cases in which lymph nodes were suspicious or reactive. Calcifications and vascularity were also assessed. These features were evaluated to categorize patients into most likely benign or most likely suspicious that need further evaluation by FNAB. Most of these features were reported by other various studies worldwide to evaluate thyroid nodules.28 -31 Thyroid nodules are more likely to develop in women in the study. This is consistent with worldwide reports, as nodules are 9 times more common in women. 32
A family history of thyroid disease was a strong predictor of the development of thyroid nodules in our study. The presence of a first-degree relative with a thyroid malignancy increases the risk of thyroid cancer by up to 9-fold.33,34 The nature of the family history of either malignancy or otherwise needs to be clarified to stratify the risk, which is a limitation of the study. Thyroid nodules were more common in patients with iron deficiency anemia, which might be due to disease chronicity or severe illness, such as thyroid cancer.35,36 Other factors that can cause anemia, including heavy menstruation, should be controlled to obtain a clearer picture.
The prevalence of malignancy in thyroid nodules was not assessed in our cohort because the number of patients who underwent US-guided FNAB and had malignant lesions was small. Therefore, none of the above-mentioned features could be accurately assessed to generalize the results of malignancy on thyroid ultrasound. However, 1 study reported a percentage approaching 90% in the sensitivity of ultrasonography-based diagnosis of thyroid malignancy when confirmed by histopathological examination after FNAB. 37 Barriers to the use of FNAB should be addressed in future studies.
To the best of our knowledge, this study is the first to determine the prevalence of thyroiditis and thyroid nodules according to clinical and laboratory findings at the primary health care level, all available literature reported these data at the secondary and tertiary levels of care. Using an electronic filing and record system to extract patient data minimized the risk of recall bias in this study.
This study has limitations. First, although the data from all patients who underwent thyroid US in our center were included in the analysis to minimize selection bias, the sample size was small.
Therefore, the analysis of imaging and laboratory data from a larger number of patients and corresponding demographic and family history characteristics is necessary to generalize the results to the Saudi population. Second, pregnant women were included in the study, and pregnancy can potentially influence thyroid gland function.
Conclusion
Thyroiditis and thyroid nodules were prevalent in our study. The presence of thyroid enlargement increased the risk of US-detected thyroiditis, and iron deficiency anemia and hypertension increased the risk of developing thyroid nodules. In addition, vitamin D deficiency, other autoimmune diseases, and a family history of thyroid disorders were associated with thyroiditis and thyroid nodules. This study raises family physicians’ awareness of the high prevalence of thyroiditis, thyroid nodules, and associated risk factors, increasing the suspicion of these entities, especially in patients with multiple risk factors. Further studies exploring other factors that were not investigated in this study are required. Moreover, patient perspectives on barriers to the use of FNAB should be assessed in future studies.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
This study was approved by the Institutional Review Board of Imam Abdulrahman Bin Faisal University (IRB number: IRB-2019-01-235).