
Abstract
Adverse childhood experiences (ACEs) are potentially traumatic events that can cause lifelong suffering, with 1 out of 2 children in the United States experiencing at least 1 ACEs. The intergenerational effect of ACEs has been described, but there’s still paucity of knowledge of its impact on child development and behavior in children enrolled in Early Head Start (EHS) home visiting programs. A retrospective observational study was performed with 71 parents and 92 children participating in the EHS Home Visiting Program in Olmsted County from 2014 to 2019. Parents reported their own ACEs using a 10-item questionnaire. Children’s social-emotional status was evaluated with Devereux Early Childhood Assessment Second Edition (DECA) and development was evaluated using the Brigance Early Childhood Screens III. Referrals of children by EHS staff to community agencies were recorded. The association between parental ACEs score, developmental outcomes and referrals was analyzed. Parental ACEs score of 4 or more was associated with failing at least 1 domain on the Brigance screen (P = .02) especially adaptive/cognitive domain (P = .05), and increased risk of referral to community resources (P < .001). However, there was no association between ACEs scores and failing DECA screens. We identified an intergenerational association between parental exposure to ACEs and risk for childhood developmental delay and referrals to community services. Parental adverse childhood experiences (ACEs) have intergenerational effects on offspring. In our study, parental ACEs are associated with offspring developmental delays and referral to community resources. Screening for parental adverse childhood experiences, a key social determinant of health, is imperative and should be incorporated into primary care and early childhood settings to identify children at risk for developmental delay.
Keywords
Background
Adverse childhood experiences (ACEs) are potentially traumatic events including exposure to violence; emotional, physical, or sexual abuse; neglect; divorce; parental substance abuse, mental health problems or death; and social discrimination. ACEs can cause lifelong medical and social suffering including premature death.1-3 Cumulative stress in childhood has been associated not only with adult health outcomes like obesity, mood disorders, ischemic heart disease, and cancer, 3 but also with childhood problems including attention deficit hyperactivity disorder, asthma, and poor overall health. 4
ACEs are quite common in all children across all income and ethnicity groups with studies suggesting that approximately 1 in 2 children in the U.S. have at least 1 ACE.5,6 While many studies have investigated the impact of ACEs on later-life health outcome, quality of life, and life expectancy,4,7 little is known about the intergenerational impact of parental ACEs on offspring behavior and development.
The intergenerational effect of ACEs has been previously suggested in studies demonstrating the association between parental ACEs score and current child adversity, including prolonged separation from parents, neglect, and homelessness 8 ; and showing that for each additional maternal ACEs, there is an 18% increase in the risk for a suspected developmental delay. 9 Other studies have also elucidated the pervasive nature of parental ACEs transmitting to child behavioral problems as screened by various means of self-report questionnaires.10-12 Higher maternal ACEs scores are also associated with indirect markers of future child developmental outcome including birth complications such as low birth weight, perinatal maternal depression, and delayed infant growth.13-17
The effect of childhood trauma can be intergenerationally passed on through epigenetic mechanisms. 18 However, the interactions between genes and environment likely impact the heritability of different genetic phenotypes impacted by ACEs. 19 Methylation patterns of paternal sperm 20 and fetal reprograming 21 during pregnancy are 2 ACEs-related genetic changes that have been described. In addition, parental childhood stressors may be triggered during the perinatal period or when caring for their infants, impeding the nurture of their children and perpetuating the cycle of trauma. 22 Therefore, the negative consequences of ACEs are striking both in time, as they cycle through lifetime and across generations; and in the gravity of their impact on health outcomes.
These recent findings call for more research effort to better understand the link between parental ACEs and offspring health consequences to help reduce its negative effects. Interventions focused on parental strengths and positive reinforcement during this period have the potential to end the “trauma cycle.” 23 Home visiting programs have been effective in strengthening parental skills and screening of family risk factors for ACEs as part of routine childcare. Primary prevention strategies including maternal support and early referrals are some of the important services that these programs provide.24,25 These interventions can improve children’s cognitive functioning, self-regulation, and advancement of development. 26
Therefore, we conducted this study to assess the association of parental ACEs on child development, behavior, and referrals to community resources in the context of a Midwest suburban pediatric setting enrolled in an Early Head Start (EHS) home visiting program. More specifically, our objective is to understand the consequences of high ACEs scores of parents on child performance on developmental screenings, as well as child welfare measured by the number of referrals to a medical provider, mental health specialist, or social services; given the fact that children enrolled in EHS are highly exposed to socioeconomic risk factors. We hypothesize that parental ACEs exposure is associated with child developmental delay and impaired social-emotional status as well as increased referrals of children by EHS staff to community resources.
Methods
Study Design
This was a retrospective cohort observational study. Researchers received de-identified, paired questionnaire results. The questionnaires that were utilized for this study are routinely used by Head Start. The data was collected by Head Start home visitors as they would routinely do and not by study investigators. Because the data was de-identified, the Institutional Research Board exempted the protocol from review on 10/02/2017. Even though no consent process was required, Rochester Early Head implemented their own consent for ACEs screening. Study investigators who were not employed by Head Start were not a part of designing or implementing this consent process. As a part of this consent process, Head Start staff disclosed that de-identified information would be shared with Mayo Clinic and obtained a signature of consent for their records.
The use of family education materials regarding ACEs was initiated in 2014 when this screening was first introduced and was continued during this study.
Participants
All parents and children participating in the Early Head Start (EHS) Home Visiting Program in Olmsted County, Rochester, MN from 2014 to 2019 were included in this study. Because data was deidentified only general demographic information from EHS was available. In 2016, the demographics of the race distribution of children in EHS Start was 40% White, 33% Black, 10% multi-racial, 9% Asian, 5% Hispanic, and <1% American Indian/Alaska Native. While only 5% identified as Hispanic race, 35% identified as Hispanic/Latino ethnicity (Personal communication with Sandy Simar, Director of Families First Minnesota, Rochester, MN, 2016).
Early Head Start
The EHS Home Visiting Program provides education to families with children up to age 3 years of age that meet the federal poverty guideline. Children are voluntarily registered in the program via recruitment, referral, or word of mouth. They receive a minimum of 48 weekly visits per year with each visit 90 min long focusing on evidence-based parent education and child development guidance. A home visitor (usually a social worker) observes the child’s developmental progress and parent-child interactions, and makes recommendations via the evidence-based Growing Great Kids/Growing Great Families curriculum (GGK/GGF). 27
Study Instruments
ACEs screen
Parents were screened for ACEs using a 10-item questionnaire created by Felitti et al 3 that identified childhood abuse (physical, sexual, emotional), neglect (physical, emotional) and household dysfunction (parental mental illness, incarceration, substance abuse, divorce, or mother treated violently). A score of 0 was given for every negative answer, 1 for every affirmative answer, resulting in a total ACEs scores between 0 and 10. The ACEs screen was translated into Spanish, Somali, and Arabic for this study by institutional translation service. Parents had the choice to complete their own questionnaire or have the EHS staff complete it with them. There is no standardized cutoff value to define a “high score.” However, Felitti et al 3 in their ACEs study reported increased risk for health conditions with a score of 4 or more. In our study, like many others, 4 or more ACEs is considered a high score which is associated with higher risk for developing child adversity.8,9
Developmental screens
The web-based Devereux Early Childhood Assessment Second-Edition (DECA) is a nationally standardized and validated social and emotional health screening tool that measures behavioral risk and protective factors of children ages 2 to 5 years old. 28 DECA has been shown to be reliable in evaluating at-risk children, including those enrolled in Head Start (HS). 29 DECA consists 38 questions on 2 scales, the Total Protective Factors (TPF) scale and the Behavioral Concerns (BC) scale. The TPF scale consists of the Initiative, Attachment/Relationship, and Self Regulation scales, each containing 9 items. There are 11 items for the Behavior Concerns (BC) scale, all involving behavioral concerns, such as “fight with other children” or “destroy or damage property.” The rater, who is either a parent, family caregiver, or a childhood professional who has daily contact with the child, is asked to respond how often a behavior has been observed in the past 4 weeks. The DECA assesses social and emotional health such as whether a child acts happy when praised, self-calms, or tries to comfort others. The web-based DECA contains programs that generate t-scores for initiative, self-regulation, attachment, and total protective factors. The t-score descriptions are Need (t-score ≤40), Typical (t-score 41-59), and Strength (t-score ≥60). 30 When “Need” is identified on any scale, the program generates a report of classroom and/or home strategies.
The Brigance Early Childhood Screens III screens development from birth to 7 years 6 months of age. Screens include skills across 3 domains with corresponding subdomains (ie, skill areas). These include (1) Physical Development (gross and fine motor skills), (2) Language Development (receptive and expressive language skills), and (3) either Adaptive Behavior for infants and toddlers (self-help and social-emotional skills) or Academic Skills/Cognitive Development for children 2 years of age and older (literacy skills and mathematical concepts). 31 Our study used data sheets for infant (0-11 months) with 85 items, toddler (12-23 months), with 83 items, and 2-year-old with 43 items. Data sheets were hand scored. The skills are weighted and generate a total score of 100 points. For example, language skills such as toddlers being able to point to pictures that are named is a critical skill and receives more weight in scoring. Total scores are compared with the child’s age-appropriate cutoffs. The child’s total score is identified as advanced (infant and toddler), may be gifted or academically talented (2-year-old and older), age-appropriate, or developmentally delayed/academic delays. A total composite score can be generated, with an average range of 90 to 110, and ranges from <60 to >125. A composite score can also be generated for each domain, and the subdomains of self-help and social-emotional. The test’s sensitivity is 76% and specificity is 86%. 32
Procedures
Families were informed of the ACEs screening at a home visit by an EHS home visitor and subsequently were given and/or read an ACEs explanation pamphlet. The pamphlet covered what questions the ACEs screen would ask, explained that honesty was best when answering. A short video was shown which explained the definition of ACEs, how they affect parents and their children and tips/skills/resources to support families. The home visitor informed parents that the results of the ACEs screening process and child health outcomes would be shared with a study team but that no data would be shared that would personally identify them. Prospective participants were told that the aim of this study was to determine how their possible ACEs impact the health and development of their children. A signature of consent to share this de-identified information was completed before the screen was administered. Parents were asked by the EHS staff to report their own ACEs using the 10-item ACEs questionnaire. This questionnaire and the consent signature were completed between the 4th and 36th home visit, depending on when the home visitor felt it was appropriate to administer the ACEs screen; with the exception of children less than age 1 year whose parents were informed of the study plan and completed the signature of consent regardless the number of home visits completed up to that point.
The EHS staff completed the DECA and Brigance screens for children in the program. If children had more than 1 screening with either the DECA or Brigance during the study time period, then the first one was used for the analysis. For children who were screened with both the DECA and Brigance screens, this occurred at different timepoints as the Brigance was in children less than 3 years old and DECA was used in children 3 years old and older, as per EHS programs budget. The number of referrals to a medical provider, school district, mental health, or social services was recorded by Head Start staff.
Parental ACEs score, children developmental screening results and number of community referrals were shared with study team with a de-identified, paired database. However, the reasons for referral were not available to research staff.
Analysis
Descriptive statistics of participant demographics and screening results were produced using Microsoft Excel and the statistical software JMP (John’s Macintosh Project Pro Version 14, SAS Institute Inc, Cary, NC, USA). 33 The association between parental ACEs scores (≥4 vs <4) and DECA outcomes (typical or strength/need), Brigance outcomes (pass/fail), and referrals (yes/no) were analyzed using Pearson’s chi-square test. For the Brigance screen, developmental or academic delay were categorized as “fail” and all other results were categorized as “pass.” All statistical analysis was performed with JMP.
Results
There were 71 parent participants in the study (7 males, 63 females, and 1 unknown). The Head Start staff reported that no families declined sharing de-identified information with the investigative team so all eligible children were included in this study. Among them, 70% reported an ACEs score of at least 1, and 40% reported an ACEs score of at least 4. The range of scores represented among the parents was 0 to 10 with mean ACEs score of 3.07 (standard deviation 3.06). A total of 92 children participated in the study including 45 males and 47 females. From those 92 children, 21 were siblings and the same parent participated with both. The median age was 24 months with an interquartile range from 9.2 to 33.8 months. From those 92, 47 children (51%) were screened with both Brigance and DECA, 23 children (25%) were only screened with Brigance, and 17 (18%) were screened with the DECA.
The results of the DECA are presented in Table 1. Out of the 64 children evaluated with DECA, 9% of them had the outcome of “need” in at least 1 category. However, there was no statistically significant difference between parental high ACEs scores (defined as more than 4 ACEs) and failing any aspect of the screen (P = .57).
Association of Child DECA Developmental Screen Results With Parental ACE Score.*

Pearson’s chi-square test.
The total number of parents participants was 58, 37 of those had an ACEs score <4 and 21 had an ACEs score ≥4.
The results of Brigance screens are present in Table 2. Brigance screen included 3 domains: adaptive/cognitive, language, and physical. Out of the 70 children evaluated with Brigance, 20% of them were determined to have developmental delay in at least one of these domains. Overall, parental ACEs score of 4 or more was associated with failing at least one domain on the Brigance screen (P = .02). High parental ACEs score was associated with an increased rate of failing adaptive/cognitive (P = .05) domain. However, there was no statistically significant difference in language (P = .37) or physical domains (P = .16).
Association of Child Brigance Outcome With Parental ACE Score.*
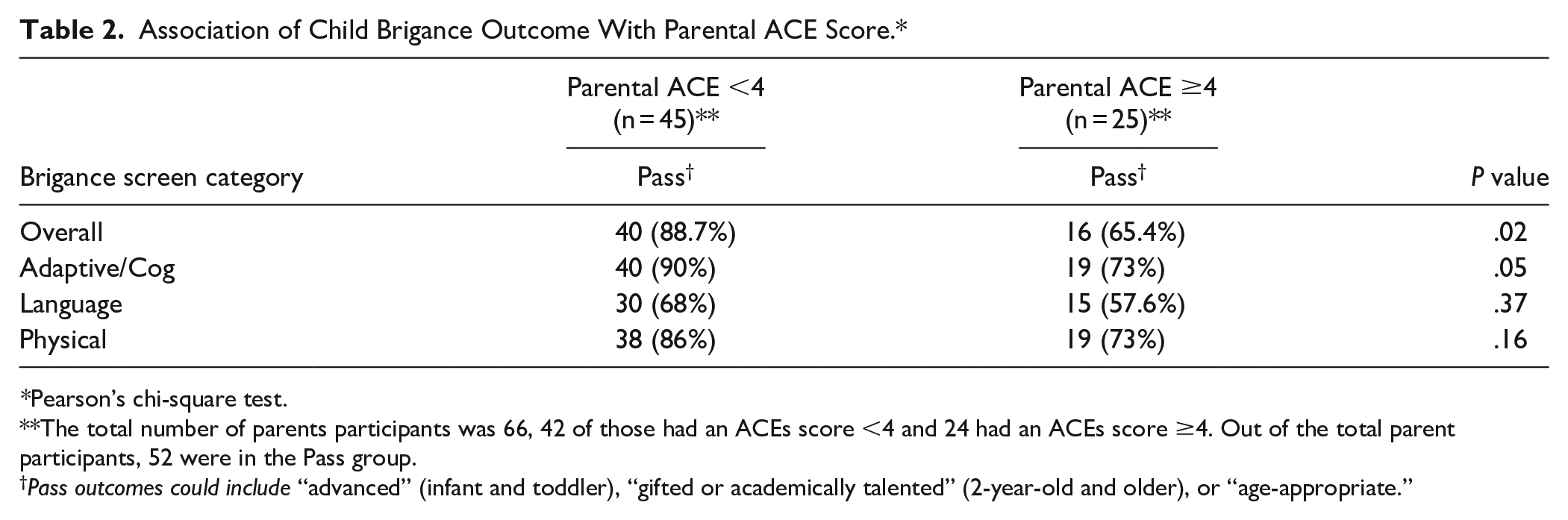
Pearson’s chi-square test.
The total number of parents participants was 66, 42 of those had an ACEs score <4 and 24 had an ACEs score ≥4. Out of the total parent participants, 52 were in the Pass group.
Pass outcomes could include “advanced” (infant and toddler), “gifted or academically talented” (2-year-old and older), or “age-appropriate.”
A total of 22 (23.9%) of children who were referred by EHS staff to community resources as shown in Table 3. Referrals were made to mental health specialist (2), medical doctors (5), the social services (7), or school district (8). Parental exposure to 4 or more ACEs was associated with a significantly increased risk of referral to community resources (P < .001).
Association of Child Referrals to a Community Resource With Parental ACE Score.*

Pearson’s chi-square test.
The total number of parents participants was 71, 46 of those had an ACEs score <4 and 25 had an ACEs score ≥4.
Discussion
The present study shows a statistically significant association between higher parental ACEs score and offspring’s developmental delays, with higher referral rate to community agencies for those children. In contrast to previous research, our study fails to demonstrate a significant association between higher parental ACEs scores and offspring socio-emotional/behavioral difficulties.
Many studies have associated a high parental ACEs scores with child adversity.8-10,12 Randell et al reported a strong association of child adversity and parental ACEs score of 4 or higher in a study conducted in a Midwest Head Start population. The study involved 400 families, with 81% of African American children aged 6 weeks to 5 years old. 8 Child adversity included prolonged separation from parents, neglect, homelessness, death of a family member/close friend, and exposure to community violence, family violence, household criminal activity, or household substance abuse. Folger et al reported developmental delays at age 24 months for children whose mother’s ACEs score was 3 or more. The study conducted in a primary care practice from a metropolitan area in Portland, Oregon, involved 363 predominantly white (53.4%) families. Developmental delays were described in several domains, however, communication and motor skills were the only ones that presented a statistically significant association. 9 Higher ACEs scores were also associated with more missed well child visits by 2 years of age. 34 Our study results add to present evidence demonstrating that several child developmental domains can be affected by higher parental ACEs scores. 9 Like Folger et al our study showed increased delays in motor skills, even though it was not a statistically significant association. In contrast to that study, we reported increased delays in adaptive/cognitive behavior, but failed to show any difference in communication skills. Further research should focus on determining if there are child developmental domain-specific delays associated parental ACEs and the timing and duration of these delays.
The association between parental ACEs scores of 4 or more and child socio-emotional/behavioral problems has been reported in 1 previous U.S. general population study of 2529 children, a majority (80%) who were Caucasian.10,11 Socio-emotional problems were measured using the Behavior Problems Index (BPI) and the Positive Behavior Scale (PBS). Both tests were administered to the primary caregiver. Increased internalizing and externalizing behavior, lower measures of positive behaviors and increased odds of ADHD were reported. 10 Conversely, our study did not show a positive association between high parental ACEs score and socio-emotional/behavioral problems. Even though TPF and BC scales, used in the DECA, are similar to both BPI and PBS; these were designed for children older than 4 years old. Social-emotional problems can be assessed in younger children. 35 However, there are no gold-standard measurements to detect socio-emotional problems in infants and toddlers. The median age of our population was 24 months and previous research has shown that the most comprehensive/ accurate tools in this population are the Ages and Stages Questionnaires: Social-Emotional—2 and the Brief Infant-Toddler Social and Emotional Assessment.36,37 Thus, lack of findings could be explained by the tool used in the study. It is plausible that social-emotional problems are more frequent or severe in older children and easier to detect in this population. It is also possible that our study was underpowered for this study outcome as our population size was smaller. Future studies should focus on the timing, duration, and severity of socio-emotional problems in preschool age children whose parents have experienced ACEs.
Screening for ACEs in the primary care home has been recommended by the American Academy of Pediatrics since 2013 but this recommendation has not been well followed. A study from 2016 found that 61% of pediatricians did not ask most or all parents about any parental ACEs, 24% asked about 1 to 2 parental ACEs, and only 15% asked about 3 or more parental ACEs. 38 Screening for parental ACESs with home visitors is a potential supplemental or alternative option. The screening was feasible in our study with no families declining participation when informed that they would be asked these sensitive questions. The acceptability of screening by home visitors may have been impacted by the fact that parents were not asked about ACEs until at least the fourth home visit, allowing time to develop rapport and trust with the families. In addition, the home visitors introduced the topic using a video and informational pamphlet. Screening for parental ACEs is imperative as it is predictive of future developmental and behavioral problems in children and, in this study, we found that it may also predict the need for community referrals. This is important because there is strong evidence of effective interventions in families that have experienced ACEs. A recent review 39 found that integrated, medium (home-visits or multiple follow-ups for 4-18 months) to high intensity (home visits for 3-5 year) interventions can improve children’s behavioral and mental health problems and child-parent relationship. Evidence supports that home visiting programs mediated by community nurses 40 or mental health professionals 41 that included parenting education and connections to community resources are the most effective.
There are a few limitations in our study. First, ACEs score was measured by participant self-report and type of ACEs (various forms of abuse, neglect, household dysfunction) was not individually considered or taken into consideration when analyzing the impact on children’s health. Second, although the ACEs screening instrument that we utilized is commonly referenced and used, it has not been validated. Unfortunately, most other ACEs screening tools for this age group have not been validated.42,43 Third, our intervention occurred at 1 EHS site in 1 Midwestern city and may not be applicable to other locations with different socio-demographic factors. Fourth, almost 50% of children only received 1 screening tool depending on their age, but also due to dropping out of the program or transitioning to another program. Lastly, there were 21 siblings (out of 92 participants) in the study which shared a parent and home environment with at least 1 other study participant. While this potentially could add bias, we included siblings as it increased the number of child developmental and referral outcomes.
In summary, we identified an intergenerational association between parental exposure to adverse childhood experiences and risk for childhood development delay and referral to community services. The health effects of ACEs may not be limited to the exposed individual, highlighting the need for a 2-generation approach. Furthermore, we believe that early screening and referrals are key to addressing the social determinants of child health. Further research is needed to understand the psychological and biological mechanism of these intergenerational health effects.
Footnotes
Acknowledgements
We would like to thank all Early Head Start Home Visiting Program staff from Rochester Families First of MN (Head Start) staff for their support of the project and especially thank Ivana Rukavina for her leadership and collaboration. We also thank undergraduate research assistant, Alicia Woodward, for her aid with data collection for the project.
Authors’ Note
Its contents are solely the responsibility of the authors and do not necessarily represent the official views of the NIH.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was co-funded by the Mayo Clinic Center for Clinical and Translational Science and the Mayo Clinic Children’s Research Center. This study was supported by CTSA Grant Number UL1 TR002377 from the National Center for Advancing Translational Science.