
Abstract
Introduction
Background Knowledge
Nigeria, the most populous African nation, has some of the worst maternal, newborn, and child health indicators in the world, and urgent efforts to improve the situation are critical as the deadline (2015) for achieving the Millennium Development Goals draws near.1,2 In Northern Nigeria, the maternal mortality ratio (MMR, ie, deaths per 100 000 live births) is estimated to be much higher than the national average 3 with recent estimates for the north exceeding 1000 deaths per 100 000 live births, compared with MMR estimates for the southern region, which is less than 300 deaths per 100 000 live births.4-6 Furthermore, maternal mortality in Northern Nigeria increased between 2003 and 2008, reflecting declines in antenatal care (ANC) utilization and deliveries with a skilled birth attendant (SBA). Between 2003 and 2008, the percentage of women who received any ANC services for births in the 5 years prior to the surveys dropped from 36.9% to 31.1% in the North West zone and from 47.3% to 43.0% in North East zone. Similarly, skilled assistance at delivery declined from 12% to 8.9% in the North West zone and from 19.8% to 13.1% in the North East zone.7,8 The decline in ANC and delivery with SBAs was largely because of a dysfunctional health system in the rural areas where most people live, with poorly equipped and understaffed health facilities, lack of basic essential medicines, low quality of care by primary care facilities, and long distances on poor or nonexistent roads to the nearest health facility. For example, Jigawa State in the North West region had 5 nurses per 100 000 population, compared with 59 nurses per 100 000 population in Enugu State, located in Nigeria’s south. 9
The Intervention
Faced with the stagnation or decline in maternal health in the North West and North East zones, the Partnership for Reviving Routine Immunization in Northern Nigeria (PRRINN) was established in 2006, and expanded in 2008 to include maternal, newborn, and child health (MNCH), becoming PRRINN-MNCH (hereafter “the program”). The program was funded by the Department for International Development of the United Kingdom (DFID) and the State Department of the Norwegian Government. The unacceptably high rates of maternal, newborn, and child mortality were addressed by comprehensive and integrated health systems changes impinging on the provision of quality maternal and child health care, including the systemic components of governance, human resources, clinical services, health information utilization, and community engagement. This report focuses on the program implemented in the 3 states of Katsina, Yobe, and Zamfara, which were supported to improve MNCH services in addition to immunization promotion.
The program organized the support for health system strengthening around the World Health Organization cluster model for the establishment of comprehensive emergency obstetric care (CEOC) services for a cluster of Local Government Areas (LGAs) comprising approximately 500 000 individuals. The CEOC facility was strengthened along with 4 Basic Emergency Obstetric Care (BEOC) facilities (each serving 100 000 persons) and eight “24/7” primary health care facilities providing obstetric care. Comprehensive primary care services at these 8 clinics were revitalized, with multiple trainings to nurses, midwives, and community health extension workers (CHEWs) who staff the primary health care centers. Particular attention was paid to upgrading routine immunization services, as well as basic antenatal care services. Supportive supervision was introduced to provide guidance in improving quality of care, and the entire health system’s information system was upgraded to an electronic health information system.
Supplementing the supply-side changes were activities that created awareness of and demand for MNCH services. Selected groups of villages served by primary care facilities linked to the upgraded emergency obstetric care (EOC) facility participated in a community engagement process, which aimed to reach entire communities and increase awareness, knowledge and practice of healthy behaviors in response to household and community level MNCH barriers. Core to this process was a community discussion group, which provided a space for reflection and problem solving for the most prevalent MNCH problems affecting the community. Community volunteers (CVs) were recruited in each community and trained to facilitate the discussion groups and other activities with the aim of mobilizing communities around an MNCH agenda. A community-wide approach was adopted where entire communities—men, older women, traditional leaders, in addition to women of reproductive age—were encouraged to participate. The CVs were taught to use a range of participatory methodologies, including communication body tools and songs, to engage the community around critical MNCH issues. Key topics covered in the discussion groups included the maternal and newborn danger signs, the need for a safe pregnancy plan, care, nutrition in pregnancy, the vaccination schedule, the benefits of ANC, and essential newborn care. Men and women participated in separate discussion groups.
The CVs were also asked to identify and refer to the primary health center any pregnant women, those nearing delivery or at risk for delivery or pregnancy complications, as well as sick children needing medical attention. As part of the community engagement approach, the program worked in partnership with the National Union of Road Transport Workers to implement a community-based emergency transport scheme (ETS). ETS drivers resided in the intervention communities and were trained to provide a fast, supportive and low-cost service in situations where women experienced a maternal complication. The CVs also mobilized their communities to establish emergency savings schemes and community blood donor schemes. These schemes addressed key barriers that the communities had identified as important in baseline qualitative studies.
The program implemented the supply- and demand-side interventions incrementally adding more clusters to the intervention group. This allowed an implementation research approach to assessing the impact of the combined strategies, where program decision makers could be informed in a timely way about what was working and what was not. About one third of the intervention clusters were implemented in the first year of the program, and in each successive year approximately 20% to 25% of the remaining clusters joined the program. By the end of 2013, the program had expanded to support CEOC/BEOC/“24/7” primary health center services in virtually all LGAs in the three MNCH states, but demand-side interventions were implemented in only 82% of the LGAs.
In this article, we report on the maternal and child health outcomes associated with the program’s implementation from 2009 to 2013. Specifically, we assess (a) the extent to which reproductive health outcomes or behaviors were significantly greater at endline in 2013 compared to baseline in 2009 and (b) whether the communities engaged in the full-range of demand-side activities experienced greater improvements in basic MNCH outcomes compared with communities with no community demand generation activities.
Methods
Study Design
We used a quasi-experimental design using pre- and postintervention household surveys in the intervention and control communities. The preintervention or Baseline Household Survey (BHS) was conducted in April-May 2009 and the postintervention household survey, the Endline Household Survey (EHS), was conducted in May-June 2013. The impact evaluation contrasted respondents according to where program activities had been implemented in the sample communities and whether they had been aware of or participated in them. Availability of the program activities was assessed by a combination of information from program staff and from the community-level survey, which asked what activities had taken place in the sample village.
As the baseline was entirely preintervention, all responses in the BHS were considered control. By 2013, virtually all 55 of the LGAs in the original sample had received the statewide supply-side interventions, for example, training of health care workers or facility upgrades, and 82% of the LGAs had received the community engagement package. Therefore, in the EHS, the control areas were defined as those that had not yet received the integrated community engagement package.
A core strategy of the program was to ensure maximum spread of MNCH knowledge and of the capacity to address these issues. After becoming fully operational, namely with CVs who were fully operational and community engagement activities completely implemented, known as “Community Engagement Complete” or “CE Complete,” the CVs in these CE-Complete communities were given minimal support to extend their activities and share their knowledge with neighboring communities, known as “Community Engagement Light” or “CE Light.” It was also recognized that even without a proactive dissemination effort, residents from these neighboring communities might participate in some of the CE activities at the CE-Complete community. The program kept track separately of the CE-Complete and CE-Light communities, and the EHS included these as distinctive strata in the sample. Thus, we are able to exclude the CE-Light in order to ascertain the intervention effects without spread or “contamination” effects.
Individual exposure to the program was assessed by woman’s responses to questions eliciting sources of information or health care advice and her explicit response to questions about observing or participating in activities introduced by the program. The study was approved by state ethics review committees in each of the states. The ethics review committees are certified by the Nigerian Federal Government’s National Health Research Ethics Committee to review and approve health research protocols for their states.
Study Sample
The sampling plan was a stratified 2-stage cluster sample, with oversampling of individuals in the MNCH intervention clusters. Individuals from MNCH clusters were oversampled using a ratio of 2:1, because MNCH clusters cover a significantly lower proportion of the population of each state. Oversampling provided an opportunity to generate a sufficient sample in the intervention areas to assess the impact of key elements within the intervention package on the key MNCH outcomes. The primary sampling unit for this sample was the LGA, for which there were 24 in the BHS and 51 in the EHS. For the EHS, for comparability, we included in the sampling frame all LGAs in the BHS except the LGAs comprising the state capitals. The latter were excluded in the EHS because the focus of the integrated program interventions was the rural communities. The state capitals were excluded from the BHS in the comparisons reported here. The number of households selected per LGA was proportional to the size of the LGA.
The study was designed with an 80% power to detect a 2.5% change in the percentage of women delivering with the assistance of skilled birth attendants between the BHS (11%) and the EHS. The BHS was designed to be representative of all ever-married women in the household and required a sample of 5,560 households, while the EHS was designed to be representative only of ever-married women with a birth in the previous 5 years, with a minimum sample requirement of 2310 households.
Oversampling was used to increase the number of intervention community respondents to provide additional power for behaviors with a lower frequency but which were of particular interest to the program, such as receiving advice from a community health worker. Because stratified sampling was used with differential sampling proportions for the intervention and control strata, weights are used in the analysis.
Within the LGA, the sample of households was allocated to each stratum in proportion to the size of the community or village. The sampling fraction for each community was determined by information on the total households from community leaders. Households within each selected community were randomly sampled using a procedure similar to that used in the WHO-EPI cluster surveys, namely by numbering and then sampling households according to the community sampling fraction along randomly selected paths leading out from the center of the village.
The household was the ultimate sampling unit. In compounds that comprised 1 to 3 households, 1 household was randomly chosen for interviews; in compounds with 4 to 6 households, 2 were surveyed; in compounds with 7 or more households, 3 were surveyed. Within each randomly selected household, in the BHS, all ever-married women of childbearing age (15-49 years) were interviewed, whereas in the EHS only 1 ever-married woman with at least 1 child born in the past 5 years was selected for interview. The inclusion criteria were changed for the EHS because of the need to focus on women with pregnancies and births during the time period during which the interventions were implemented. The completed interviews were 6842 in the BHS, of which 2360 are retained as having a birth in the previous 5 years, and 4628 in the EHS.
Interviewers who had completed secondary school or higher were selected and trained to visit women at home. They administered a questionnaire that included translation of key concepts and terms in the local languages (eg, Hausa, Kanuri). Most of the interviewers were women, in accordance with cultural expectations that women would only be interviewed by other women. The questionnaires were standardized across the 3 survey rounds and used close-ended questions from the 2008 Demographic and Health Survey 8 to allow comparisons of results with other national- or state-level data. The question topics covered age, parity, economic status, literacy in any language, wife marital rank, antenatal care and delivery characteristics, source of health advice for the woman or the baby during last pregnancy, experience of labor and delivery complications, knowledge of maternal and newborn danger signs and how to respond to them, actual response to danger signs of infant and child illness, and infant and child mortality. Questions and/or their response codes were modified in line with the program goals in order to focus on the specific components included in the PRRINN-MNCH program. In addition, the EHS respondents were asked to give feedback on several of the program interventions, such as what improvements they had noticed in the clinic in the past year or whether they had observed anyone using specific program components.
Analysis
At the analysis stage, the inclusion criteria for both surveys were narrowed to ever-married women, aged 15 to 49 years, with a birth in the 5 years prior to the survey. The data from the BHS and EHS were merged into 1 combined data set, using 1 uniform variable format. Respondents were assigned to the control or intervention groups based on the level of program intervention at the time of the survey. MMRs were calculated using the sisterhood method. The dependent variables are the key health behaviors pertaining to maternal health outcomes. The bivariate analyses of the merged data sets were conducted using sampling weights based on different sampling fractions in the intervention and control areas. We examined changes in the proportion with the designated MNCH behaviour or outcome, contrasting all BHS responses versus the EHS responses, intervention versus control.
In order to isolate the intervention effects without the possible spread to CE-Light communities, the EHS comparisons between the control and the intervention groups are restricted as follows. The control group (n = 1410) includes communities where no CE activities were documented in the community questionnaire administered to the village elder prior to the survey, that is, no CV and no community dialogues. The intervention group (n = 2451) was restricted to the communities where the village documented the full set of CE activities, including having CVs, community discussion groups, community savings schemes, an ETS, and other support systems for pregnant women. They may also have received visits from trained community health workers circulating among the hard-to-reach villages. Thus, the control and intervention group comparisons are for a subsample of the EHS without the possible contamination or spread of community engagement activities to neighboring communities.
Because of the exclusion of the communities with CE-Light from the assessment of the impact of the complete intervention, the totals reported for the BHS versus EHS (pre–post comparison) are not the same as those used for the Complete CE vs. No CE (intervention vs control at endline). Thus, the analysis of the impact of the intervention is according to actual exposure to the full intervention, excluding those in communities with only partial exposure. We assessed the degree to which the intervention and control groups differed using the Chi-square statistic. Analyses were performed using Stata 12.1 (Stata Corp, College Station, TX).
Results
Background Characteristics of Respondents
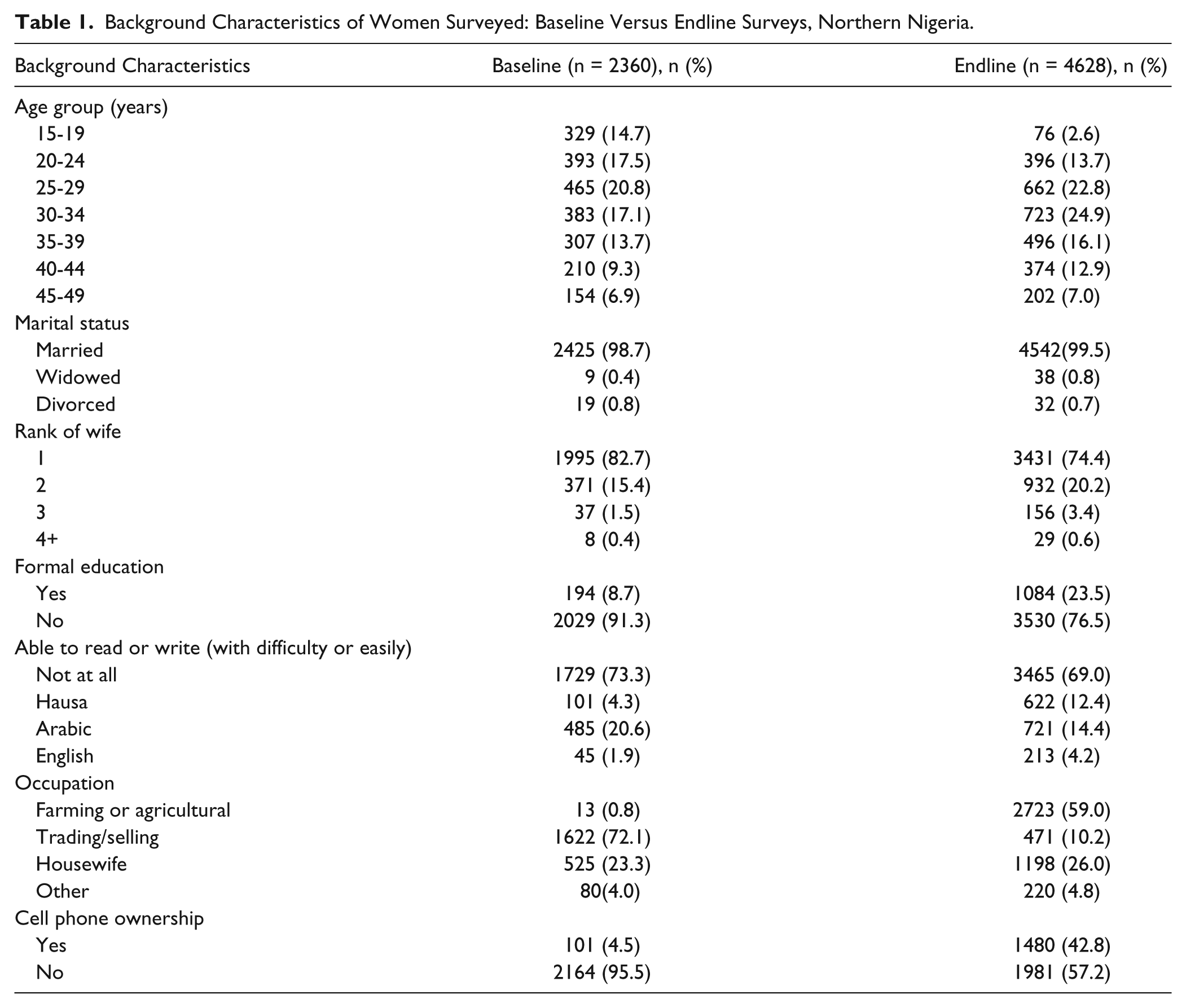
After restricting the analysis to the 2360 women in the BHS who are comparable to those sampled in the EHS, the BHS and EHS respondents were fairly similar in their background characteristics (Table 1). The age distribution of the BHS and EHS respondents is very similar, with about one third of respondents aged 20 to 29 years, with slightly more teens in the BHS than EHS and slightly more women aged 30 to 34 years in the EHS. At both times all women were currently married, but the EHS had slightly more women who were polygynous, second or higher ranked wives. The percentage of women with formal education increased from 8.7% to 23.5%. However, the proportion unable to read in any language decreased only slightly from 73.3% to 69.0%. In the EHS, more women classified their work as farming or agricultural, while in the BHS most women classified their work as trading or selling. The women interviewed in the EHS were also much more likely to have access to a cell phone (4.5% vs 42.8%), reflecting the rapid country-wide expansion of cell phone access since 2008. These differences reflect the transformations to these communities as more women are being drawn into the labor force in order to complement the meager family income.
Background Characteristics of Women Surveyed: Baseline Versus Endline Surveys, Northern Nigeria.
Key Maternal Health Outcomes
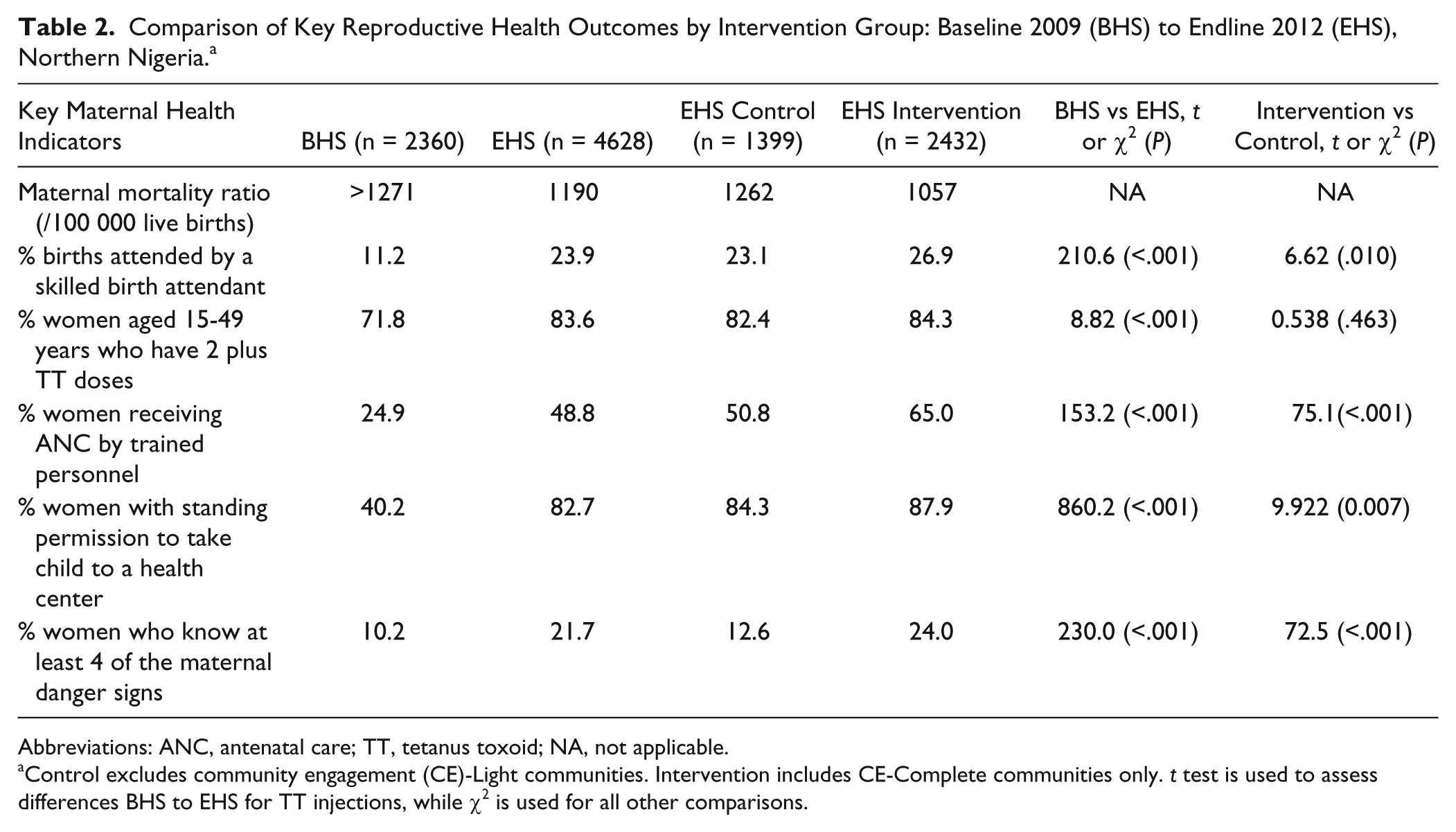
The estimated MMR at baseline was at least 1270 per 100 000 live births, which was calculated using the sisterhood method using the PRRINN-MNCH midterm survey of 2011. 1 This figure is considered conservative given other estimates for MMR in Northern Nigeria, which average 2420 per 100 000 live births. 2 Using the sisterhood method with data from the EHS, the MMR is estimated to have declined to 1190 per 100 000 live births. In the control communities that did not have the complete intervention the MMR had decreased marginally to 1262 in the CE-Complete intervention communities a bigger decrease (to 1057) was recorded.
Improvements were seen in the proportions of women delivering with an SBA, which increased from 11.2% to 23.9%; having 2 or more anti-tetanus vaccinations from 71.8% to 83.6%; and having at least 1 ANC visit, which doubled from 24.9% to 48.8% (see Figure 1).
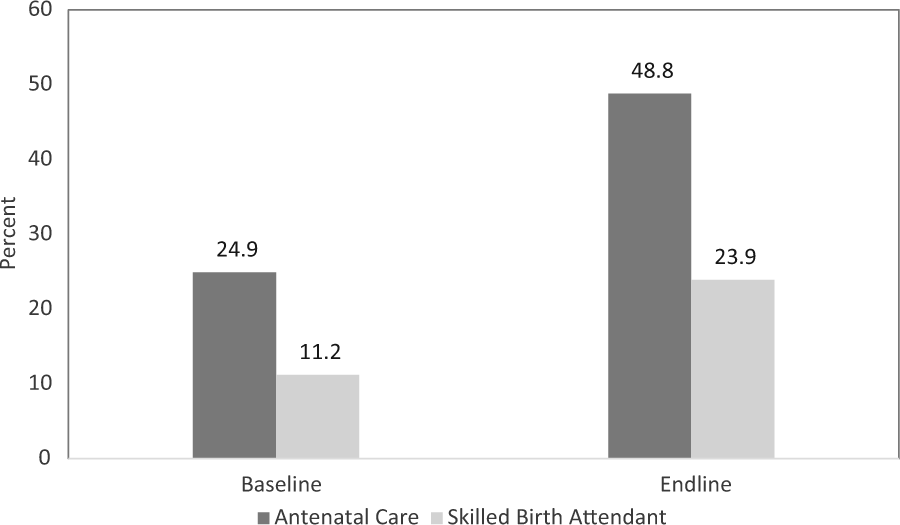
Percentage of women who had antenatal care or skilled birth attendant for their last pregnancy and delivery: baseline versus endline surveys, Northern Nigeria.
At endline, both ANC and skilled birth attendance were significantly higher in the intervention than control communities. In the intervention communities with CE-Complete, the proportions with any ANC visit were 65.0%, versus 50.8% in the control communities; 26.9% delivered with an SBA in the intervention with CE-Complete versus 23.1% in the control communities, which did not have community engagement.
At endline, and little changed from baseline, close to two thirds of women (64.5%) considered it very important or essential to obtain their husband’s permission prior to going for an ANC visit, and another 22.9% considered it advisable. Consistent with these views, most women responding to the EHS had obtained their husband’s permission to use MNCH services, increasing the percentage from 40.2% at baseline to 82.7% at endline, with the increase even greater in the intervention communities, to 87.9% (see Table 2).
Comparison of Key Reproductive Health Outcomes by Intervention Group: Baseline 2009 (BHS) to Endline 2012 (EHS), Northern Nigeria. a
Abbreviations: ANC, antenatal care; TT, tetanus toxoid; NA, not applicable.
Control excludes community engagement (CE)-Light communities. Intervention includes CE-Complete communities only. t test is used to assess differences BHS to EHS for TT injections, while χ2 is used for all other comparisons.
In 2009, virtually all ANC visits were provided by the doctor, nurse, or midwife. By 2013, after the efforts to increase the number of midwives at primary health care facilities and to provide CHEWs in the facilities with training on ANC visits, more than a third of women received ANC from a CHEW in the facility or in the community, as part of her community rounds (see Figure 2).

Source of antenatal care for last pregnancy in previous 5 years: baseline versus endline surveys, Northern Nigeria.
In addition to a doubling of the percentage of women making any ANC visits between 2009 and 2013, there was greater understanding about the correct timing of ANC. By 2013, 62% of respondents said they knew when they should initiate ANC. However, only 44.2% correctly specified the first trimester as recommended timing for the first ANC visit. As shown in Figure 3, the percentage of ANC visits in the first trimester increased from 25.2% in 2009 to 36.4% in 2013. Half of all women who had any ANC (55%) did so in the first trimester of their pregnancy in the intervention communities, compared with only 41% in the control communities (χ2 = 28.3, P = .002). The majority of women surveyed (87.2%) knew that they should have a minimum of 4 ANC visits. Along with this change in knowledge, the proportion who had at least 4 ANC visits increased from 66.3% to 77.6% of all women with any ANC visits for their most recent pregnancy (χ2 = 195.4, P < .001). Significantly more women had 4 or more ANC visits in the intervention with CE-Complete than in the control communities (80.0% vs 74.6%, χ2 = 42.8, P < .001).

Timing of first antenatal care (ANC) visit for those with any ANC: baseline versus endline surveys, Northern Nigeria.
Women reported receiving more complete ANC services in 2013, compared with 2009 (see Figure 4). By 2013, 80% or more of the women received the basic package of ANC services: weighed and having the infant’s growth assessed; blood pressure taken; given supplements and antimalarials; advised to sleep under a bed net; and advised on newborn care and exclusive breastfeeding. The only element of ANC which did not increase significantly from BHS to EHS was education about danger signs, which was received at ANC by only 66% of the women with any ANC.

Services received during antenatal care (ANC) visits for those with any ANC visits: baseline versus endline surveys, Northern Nigeria.
While only two thirds of women heard about danger signs of pregnancy and delivery during their ANC visits, this was one of the most important reasons women gave for an antenatal consultation, with 42.4% of the women saying this was one of the main benefits of an ANC visit, about the same percentage who said they valued learning about their baby’s growth (44.0%; Figure 5). Fewer than one fifth rated the other ANC activities as an important reason for the visit.

Most important reason for antenatal care visits, endline survey, Northern Nigeria.
Knowledge of maternal danger signs significantly increased between 2009 and 2013. As was seen in Table 2, there was a doubling in the percentage of women who knew at least 4 maternal danger signs (10.2% to 21.7%). In the intervention communities, 24.0% of women knew at least 4 maternal danger signs, compared with 12.6% in the control communities (P < .001). Significantly more women knew specific danger signs, and with few exceptions, those in the intervention communities knew more of the danger signs of pregnancy and delivery (see Table 3). At endline in the intervention communities, only 19% knew no danger signs, compared with 33% in the control communities. Also, in the intervention communities, 30% or more knew the following danger signs: severe headache, swollen hands, convulsions or “fitting,” severe bleeding, high fever and foul discharge, labor lasting 12 hours or more, and placenta not coming out in 30 minutes, which were explained by the community volunteers during community forums or discussion groups with both men and women.
Knowledge of Pregnancy or Delivery Danger Signs for Most Recent Pregnancy in the Past 5 Years by Intervention Group (Percentage), Baseline Versus Endline Surveys (BHS vs EHS), Northern Nigeria. a
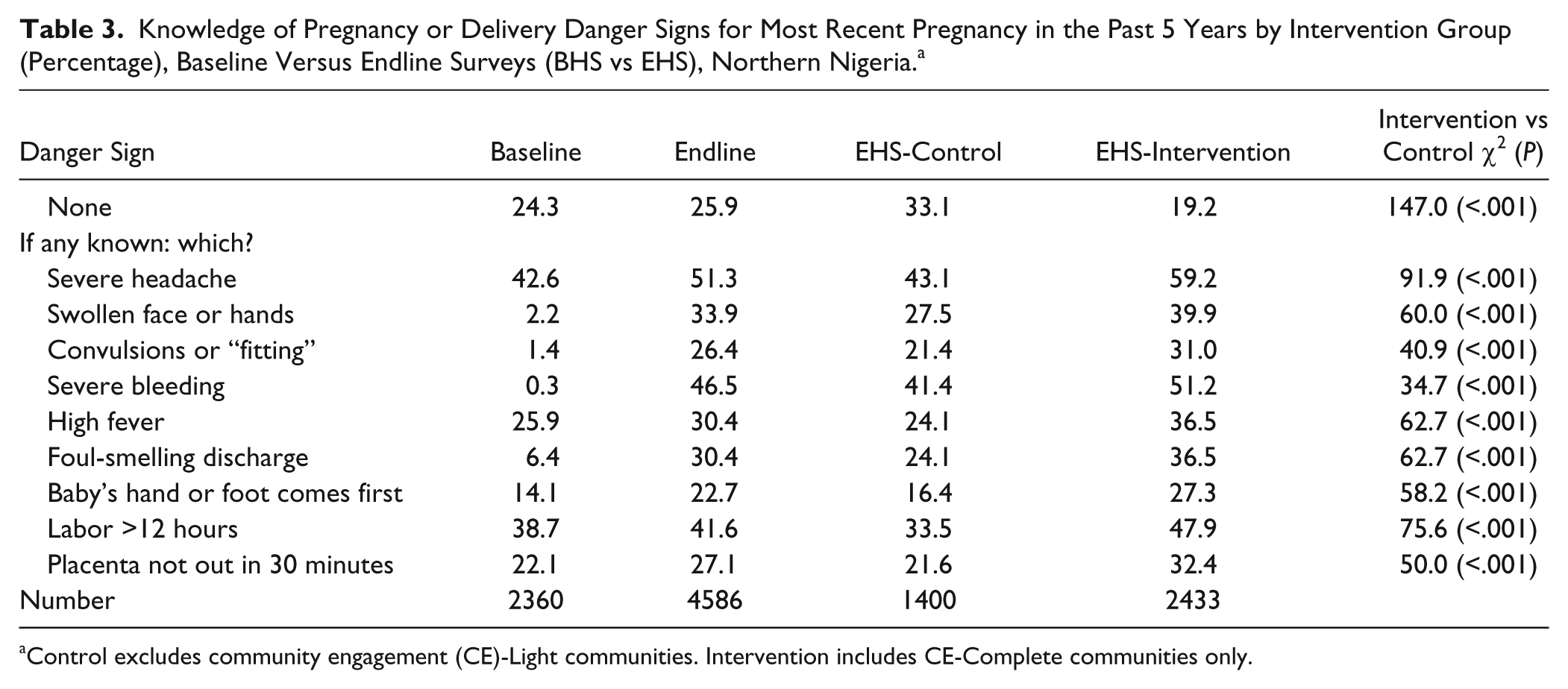
Control excludes community engagement (CE)-Light communities. Intervention includes CE-Complete communities only.
As shown in Table 4, many more women were seeking advice about their health during pregnancy in 2013, as compared with 2009. The proportion not receiving any advice fell from 74.9% at baseline to 31.2% at endline, with a further decrease to 24.3% in the intervention or CE-Complete communities. Importantly, there was a shift away from simply asking friends and family or the traditional birth attendant (TBA) for advice toward seeking advice from trained health workers, including the CHEWs, or the CVs. In 2013, more women received information from the midwife, nurse or doctor (from 5.7% to 14.5%), but, importantly, more than one-third (37%) of the women received advice from the CHEW in the facility or community or from the CV. In the intervention communities with CE-Complete this percentage rose to 44.5%. The radio jingles developed by the program’s communication component were a source of information for only 4% of women who otherwise had no information from a health care worker or CV. Thus, fewer women were relying on the TBAs or friends and family as their main source of advice about their pregnancy and delivery. This shift toward getting advice from a health worker was even greater in the intervention or CE-Complete communities, where 44.5% relied on a CHEW or CV for this advice.
Principal Source of Advice About Maternal Danger Signs and Care During Most Recent Pregnancy in the Past 5 Years (Percentage) by Intervention Group: Baseline Versus Endline Surveys (BHS vs EHS), Northern Nigeria.

Abbreviations: CHEW, community health extension worker; NA, not asked.
Control excludes community engagement (CE)-Light communities. Intervention includes CE-Complete communities only.
Part of the program’s strategy was to encourage women to make preparations for their delivery. In 2009, only 37.8% of women made any preparation for their delivery, with the most common preparation being setting aside money and preparing for a home delivery, namely having a clean razor blade to cut the umbilical cord and clean clothes ready to wrap the baby in. Only 5.1% had arranged for transport to a facility for delivery. Between 2009 and 2013, after expanding the sources of information about maternal danger signs and the importance of being prepared for a safe pregnancy, more women were making preparations that included being ready for maternal emergencies (see Table 5). One-third reported learning the maternal danger signs, and 16.4% had identified someone who would monitor labor to watch for danger signs. One- fourth had obtained standing permission from their husband to be transported to a facility for delivery, and 10.4% had already identified the ETS driver. Well more than half, 60.4%, had saved money for the delivery, and 14.3% had informed their family about the community emergency savings scheme which was available to help defray costs if needed. Almost all these preparations were more likely in the CE-Complete or intervention communities, where the radio jingles reaching all communities in the state were complemented by a structured program of community discussion groups and other dialogues led by the community volunteers.
Birth Preparations in Most Recent Pregnancy in the Past 5 years (Percentage) by Intervention Group: Endline Survey (EHS), Northern Nigeria.

Control excludes community engagement (CE)-light communities. Intervention includes CE-Complete communities only.
As shown in Table 2, the proportion of women delivering at home dropped from 89.0% to 76.1%, with significantly fewer women having a home delivery in the intervention than the control communities. In 2009, 54.7% of deliveries were attended by a TBA, while in 2013 TBAs assisted at only 39.1% of deliveries. Between 2009 and 2013, the proportion of deliveries attended by a doctor, nurse, midwife, or trained CHEW at the facility rose from 11.2% to 23.9%, with the increase greater in the intervention communities, to 26.9%, compared with 23.1% in the control communities.
Perhaps because of greater community-wide awareness of and vigilance for danger signs, the percent of women who reported experiencing serious complications rose from 2.1% in 2009 to 12.7% in 2013, with the most common complications cited by those women with any complications being prolonged labor of more than 12 hours (33.9%), severe bleeding (31.7%), high fever (24.2%), and severe headache (23.1%).
In the EHS, the women were asked to comment on the overall quality of the services they had received at the facility, and whether they had seen improvements in the past 5 years (ie, since the beginning of the program). Half of the respondents (52.2% or 2418 out of 4624 respondents) had visited their primary health clinic within the previous 6 months. Those in the intervention communities were significantly more likely to have made a clinic visit in the previous six months, 54.6% versus 49.9% in the control communities (χ2 = 10.36, P = .001). Two-thirds (67.6%) had noticed at least 1 of 10 different improvements to the services provided at their closest clinic, with the following noticed by 25% or more: more equipment in the clinic (42.8%), staff more welcoming (26.6%), open more often (25.8%), and staff better able to handle problems (24.6%). About 20% also noticed more female staff (19.3%) and that the clinic was less costly (19.0%). When asked what they liked the most about their health clinic, 23% said the friendliness of the health workers, 21% said they gave the care that was needed, and 17% said that drugs were available. Overall satisfaction with the care at the clinic was rated as good by 63.4% of respondents, and 76.6% considered the relationship between the community and the clinic to be good.
In addition to noticing improvements in the quality of service at their clinic, 75.2% of respondents had been aware of or participated in at least one of the CE activities introduced by the program, with significantly more in the intervention communities, which had complete set of CE activities, than in the control communities with no CE activities, 79.8% versus 64.6% (χ2 = 130.5, P < .001).
Discussion
Summary
Between 2009 and 2013, there was significant improvement in nearly all maternal health indicators assessed. By 2013, the majority of women (82.7%) had standing permission from their husband to go to the health center, and health care utilization went up. Skilled attendance at delivery increased from 11.2% to 23.9%, and the proportion of women having at least 1 ANC visit doubled from 24.9% to 48.8%. More women started ANC early in their pregnancy (36% in the first trimester), up from only 25% in 2009, and the percentage completing at least 4 ANC visits rose from 66% to 78%. ANC was increasingly being provided by trained CHEWs at the primary health center, who provided ANC to 34% of all women with recent pregnancies in 2013. The quality of ANC care also improved during this period. In 2009, only 60% of respondents received 4 out of 6 key services of ANC, and by 2013, 80% or more had received 5 of the 6 key services of ANC.
These improvements in women’s use of services available at the health facilities reflect the 2-pronged approach of the program. The PRRINN-MNCH Program invested in upgrading facilities, assuring that they were staffed, supplied and equipped, and that the staff were well trained. These improvements were noticed by two-thirds of those interviewed in the EHS. While more women noticed improvements in the intervention than control communities (71.7% vs 63.5%), the improvements were experienced throughout the program states, reflecting the state-wide distribution of the supply-side programmatic activities.
The greatest impact on maternal health indicators, however, was seen in the communities which had the fully implemented and fully integrated intervention, with the complete set of community engagement activities. While at baseline there were only negligible differences between the intervention and control communities, by 2013 significantly greater improvements in key maternal health indicators were seen in the intervention communities. Compared with the patterns observed in the control communities with no community engagement activities, women in the intervention communities learnt more about maternal danger signs and the steps they need to take to protect their health and that of their baby. Compared with only half of respondents in the control communities, two-thirds of the women in the complete intervention communities went at least once to ANC during their last pregnancy, they knew more danger signs, made more birth preparations, and were more likely to have a skilled birth attendant for their deliveries. Many more of the women in these complete intervention communities had received advice from community health workers either in their village or at their closest health facility. These results suggest that this advice in combination with the support received via the community engagement activities (which included access to community systems established to address physical access, affordability, and other barriers) were sufficient for them to follow the advice and make changes in how they managed their pregnancies and deliveries—and how they responded to maternal emergencies.
The significantly greater improvements in the intervention than control communities for several of the MNCH behavioral indicators highlight the importance of the program’s community engagement approach. The community engagement activities were remarkably participatory, designed to be community-led, and had a strong emphasis on local capacity-building so that changes could be sustained. The CVs were recruited from the community and trained to facilitate a structured program of participatory community discussions using active learning methods which were suitable in a low literacy context. The involvement of men and older women in the discussion groups alongside women of reproductive age helped to create an enabling environment for behavior change, allowing social norms to shift. The effect of the shift in knowledge and attitudes was quick to see, with fewer women and babies dying during pregnancy and childbirth. This created a momentum behind the work of the CVs who became highly self-motivated. Social norms can take a long time to change, but PRRINN-MNCH’s participatory group process appears to be a lever which has started a shift in thinking about what might be best for women and children.
Almost all the maternal and newborn health knowledge and behavior indicators improved between 2009 and 2013, and most of them showed a greater improvement in the complete intervention than control communities without the demand-side activities. It appears that the additional changes in awareness and ability to act on them came through the multiple and participatory channels used by the program to convey information. In the intervention communities only 5% heard about pregnancy and birth preparations on the radio, while 93% heard about these critical issues from both the radio and from participatory group discussions led by the community volunteer. This hear–say–do process of learning contributed to the increase in awareness and its translation into action in the full intervention communities. As a result, more women were making preparations that included being ready for maternal emergencies.
Because between half and two-thirds of the women made any ANC visits in their most recent pregnancy, these changes in maternal awareness and preparations reflect the combined influence of consultations with health care workers at the clinic and with the CHEWs, volunteers, and other community mobilization activities facilitated by the program. The intervention communities were engaged in a wide variety of community mobilization and health promotion activities that aimed to empower local people to devise their own community-led response to poor MNCH indicators and to build confidence in the health care system. Community-managed support systems were established that helped women obtain the services they needed, such as free emergency transport services, community emergency savings schemes, and community blood donor groups. The majority of women (80%) in the intervention communities reported being aware of or participating in at least one of the many different community engagement activities and the changes in maternal care and behaviors observed in 2013 reflect this high level of participation.
The combined health system and community-based interventions contributed to the changes observed in the proportion of women with an SBA for their most recent pregnancy, which doubled from 11% to 24%, and to 27% in the intervention communities. Fewer women gave birth alone, and, as noted earlier, more women asked one of their family members to watch for danger signs and to be prepared to take them to the clinic for delivery if complications emerged. This change in birthing practices reflects the uptake of recommendations spread throughout the community about the importance of these preparations. Furthermore, communities participating in the community engagement activities supported women’s trips to the facility for a delivery with the availability of free transport, blood donations, and a loan or gift from the community savings. While there are still further changes to be made that will make women more comfortable delivering at a facility, these changes have definitely been started.
The net impact of these changes in the intervention communities was a decline in the MMR from 1271 to 1057 deaths per 100 000 live births. There was virtually no change to the MMR in the control communities, suggesting that the critical element was highly likely to have been the effect of the community engagement activities on saving mothers’ lives. Implementation of the integrated supply-side initiatives focused on strengthening EOC services in the target clusters, support midwifery skill enhancement, the availability of community-based emergency transport, and the community engagement efforts to promote birth preparedness and planning appear to have contributed to the maternal mortality reductions observed in the intervention communities. Further, the sisterhood method of calculating the MMR is based on the history of maternal death for the woman’s sisters; the historical reference period is likely to go back more than five years. Hence, it is likely that the actual levels of change in the MMR could be greater than what was estimated by the sisterhood method.
Limitations
While it is likely that most of the changes observed in the intervention communities relate to interventions introduced by PRRINN-MNCH, initiatives sponsored by other agencies or programs, such as the child nutrition program implemented by Save the Children International or other Safe Motherhood initiatives, could have independently raised health outcomes in both the intervention and control areas. In addition, intervention activities and particularly the community demand-generation activities were rolled out by cluster, and by the time the EHS was conducted, the vast majority of the LGAs had some exposure to the intervention. While we controlled for spread or partial intervention by removing the CE-Light communities from the intervention group, this did not control for the possibility that some of the intervention communities may not have received all the supply-side activities being implemented from the state on down to the primary health center.
Conclusions
After 4 years of implementation, there were significant improvements in maternal health outcomes in the PRRINN-MNCH supported states. This was observed most clearly in the comparison of the outcomes for the women living in communities with the complete supply- and demand-side intervention versus those living in control communities with only the statewide supply-side interventions. The additional changes observed among women where they had the opportunity to learn about health issues in their own community, alongside men who also were engaged in this learning process, underscores the importance of integrating bottom-up and top-down activities, with great care to ensure that they intersect and support communities in making the changes needed to safeguard their health.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Health Partners International received funding for PRRINN-MNCH from Department for International Development of the United Kingdom (DFID) and the State Department of the Norwegian Government. The authors’ contributions to this study were funded as part of their participation in PRRINN-MNCH.