
Abstract
Introduction
Colonic diverticulitis is an acquired gastrointestinal disease that is relatively common in individuals older than 60 years. 1 In the United States, it has been estimated that this diagnosis was responsible for more than 300 000 admissions and more than 1 million days of hospitalization with an average cost of $42 000 per patient in 2004.2,3 Risk factors for developing diverticulitis include advanced age, constipation, low-fiber dietary intake, high meat consumption, and smoking. 4 Patients with diverticulitis can present with fever, acute abdominal pain, localized area of abdominal tenderness, occult melenic stool, overt lower gastrointestinal bleeding, and, infrequently, without symptoms but with abnormal imaging studies. 5 Diagnoses are based on clinical suspicion and confirmed by imaging studies, especially computed tomography (CT) of the abdomen without intravenous contrast.6,7 Acute uncomplicated diverticulitis is usually treated with medical management (intravenous hydration and antibiotics), whereas complicated diseases, such as abscess, fistula, or perforation, require surgery.5,8-10
Diverticulitis was once believed to be uncommon in younger adults (≤40 years old.) These patients, however, may develop more severe clinical symptoms with equivocal diagnoses, may require more frequent surgical intervention, and may have higher morbidity and mortality rates.2,3,11,12 Recent studies have reported a higher prevalence of diverticulitis in younger patients (up to 20% of population), predominantly obese, male Hispanics. 13 However, there are conflicting data on the prevalence, demographic data, clinical presentation, diagnosis, management, and clinical outcomes in diverticulitis in this age group, especially in comparison with older populations. We compared the demographic data, risk factors, clinical presentation, diagnoses, and management of diverticulitis in younger patients compared with older patients in our hospital.
Methods
The study was conducted at the University Medical Center (UMC), a 408-bed university-based academic hospital in Lubbock, Texas. The study protocol was reviewed and approved by the Institutional Human Research Review Board at Texas Tech University Health Sciences Center. The study population was divided into 2 groups (group 1—patients ≤40 years old and group 2—patients >40 years old.) We retrospectively reviewed all patients presenting to the UMC emergency department from October 1, 2009, to September 30, 2010, with the diagnosis of acute diverticulitis by using International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) codes (562.11 and 562.13). Patients’ medical records were individually reviewed to verify the diagnosis of diverticulitis using clinical symptoms and signs with radiographic evidence of diverticulitis. Patients who had the diagnosis of diverticulitis in the past but did not have acute diverticulitis at the index emergency department visits were excluded from the study (Figure 1). All eligible patients in group 1 were enrolled. One out of every 3 patients in group 2 was randomly selected as representatives of group 2 (1:3 ratio).
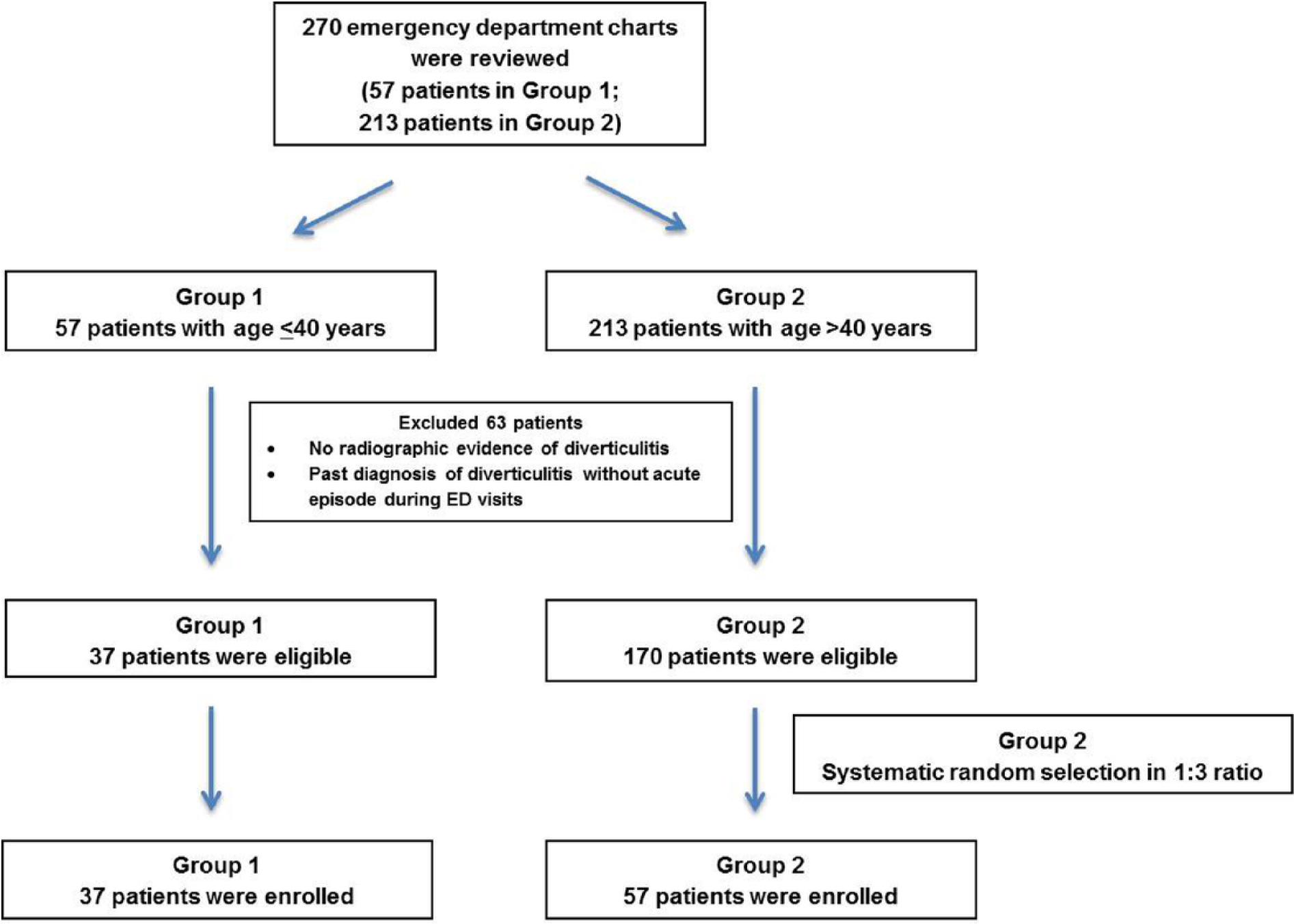
Flowchart for patient selection.
All the medical records were retrospectively reviewed; comparison between the 2 groups included evaluation of demographic data (age and sex), body mass index (BMI), other medical comorbidities, symptoms at presentation, duration of symptoms, prior history of diverticulitis, vital signs at presentation, basic laboratory data, including complete blood count and complete metabolic panel, CT scan findings, anatomical location of the involved colon, length of stay, medical or surgical management, and in-hospital mortality. The medical comorbidities identified included hypertension, diabetes mellitus, dyslipidemia, gastroesophageal reflux, asthma, and a history of smoking. Information on ethnicity was collected from the administrative information in the medical record, and all designations represent self-identification by the patient.
All statistical analyses were carried out using SPSS software version 20 (IBM SPSS Inc, Armonk, NY). The demographic data, clinical presentation, radiographic findings, management, and hospital course were compared between the 2 groups using Pearson χ2 tests, Student’s t tests, and analysis of variance. P values ≤.05 were considered significant.
Results
Baseline Demographic Characteristics
Of 270 emergency room visits with the coded diagnosis of diverticulitis, 94 patients were reviewed in this study (37 patients from 57 emergency department visits in group 1 and 57 patients from 213 emergency department visits in group 2, Figure 1). There were 46 men (48.9%) and 48 women (51.1%) with a mean age of 45.5 ± 15.3 years (range 18-87 years). The mean body mass index (BMI) was 31.0 ± 7.0 kg/m2 (range 21.8-52.5 kg/m2); 50 patients (53.1%) had a BMI ≥30 kg/m2. The study included 54 Hispanic patients (57.4%) and 36 non-Hispanic Caucasian patients (38.3%). There were more Hispanic patients in group 1 than in group 2 (75.7% vs 45.6%, P = .004). Fifty-three patients (56.4%) had at least 1 underlying comorbidity at the time of presentation (12 group 1 patients [32.4%] vs 41 group 2 patients [71.9%], P < .01). The most common comorbidities were hypertension (8 group 1 patients [21.6%] vs 26 group 2 patients [45.6%]), diabetes mellitus (3 group 1 patients [8.1%] vs 8 group 2 patients [14%]), and dyslipidemia (1 group 1 patient [2.7%] vs 9 group 2 patients [15.8%]). There were no significant differences in gender, ethnicity, or BMI between the 2 groups (Table 1).
Baseline Patient Characteristics in Each Age Group.
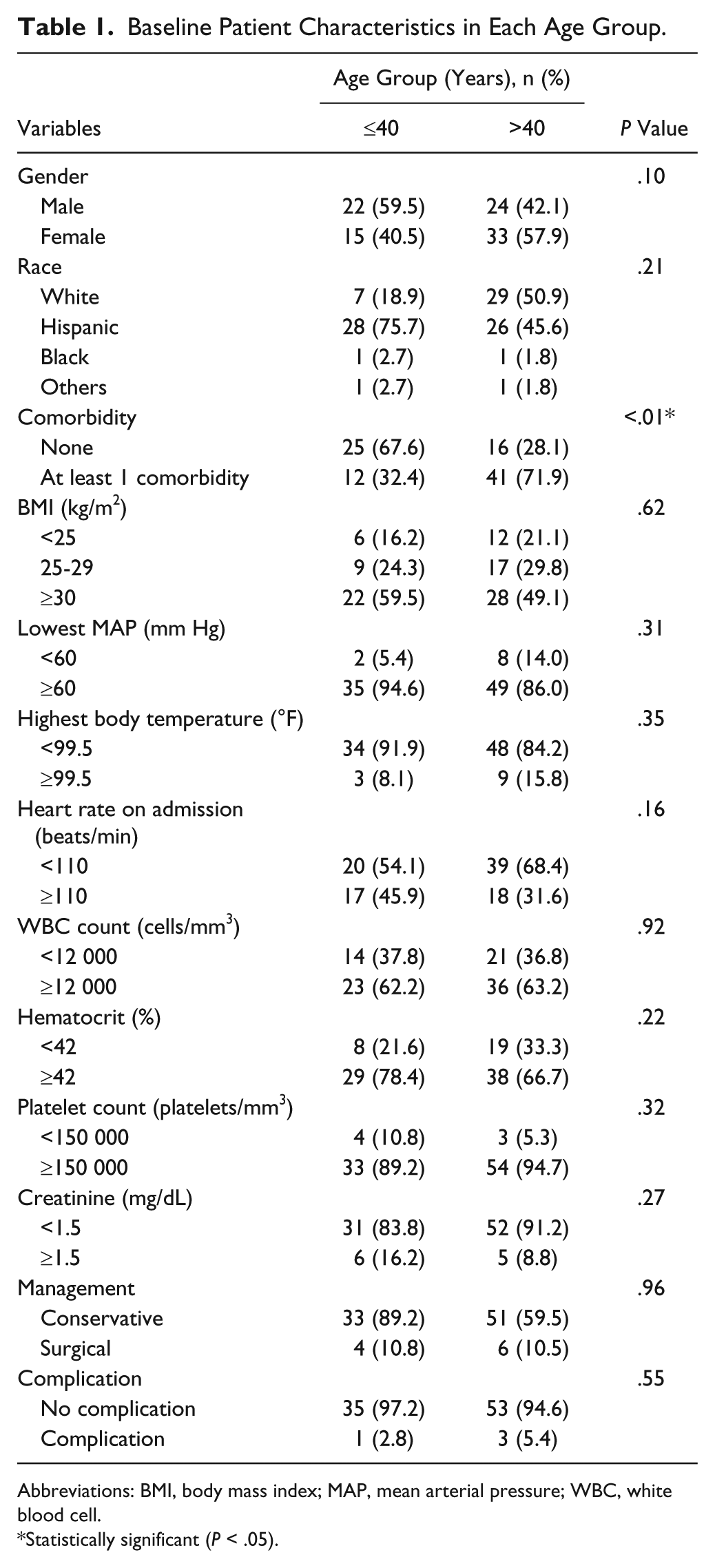
Abbreviations: BMI, body mass index; MAP, mean arterial pressure; WBC, white blood cell.
Statistically significant (P < .05).
Clinical Presentations
Table 1 reports baseline clinical findings in each age group. Twelve patients (12.8%) were febrile with a temperature ≥99.5°F at presentation (3 patients in group 1[8.1%] vs 9 patients in group 2 [15.8%], P = .35). Fifty-nine patients (62.8%) had leukocyte counts ≥12 000/mm3 (23 patient in group 1 [62.2%] vs 36 patients in group 2 [63.2%], P = .92). There were no differences between the 2 groups in white blood cell counts, hematocrits, platelet counts, and creatinine levels.
Radiographic Findings
Eighty patients (85.1%) had mild diverticulitis with localized wall thickening or pericolic fat stranding on CT scans. Fourteen patients (14.9%) had complicated diverticulitis on the CT scans (abscess, extraluminal free air, or bowel necrosis) per Ambrosetti’s criteria. 9 The diverticulitis was in the sigmoid colon (52 patients, 56.4%) and the descending colon (20 patients, 21.3%). There was no difference between the 2 age groups in the location of the diverticulitis (P = .21).
Management
Sixty-nine patients (73.4%) were admitted into the hospital. Patients in group 1 were more likely to be discharged from the emergency department (21 patients in group 1 [56.8%] vs 4 patients in group 2 [7%], P < .01). Conservative management with medical therapy was used much more frequently than surgical management (89.2% of group 1 vs 89.5% of group 2, P = .96). All patients (94 patients, 100%) received antibiotics. The most common antibiotic regimen was a combination of a broad-spectrum fluoroquinolone (ciprofloxacin or levofloxacin) and metronidazole (67 patients, 71.3%).
Clinical Outcomes
Group 1 patients had longer lengths of stay than group 2 patients (median 5.7 days vs 3.1 days, P = .16). Factors associated with longer lengths of stay are summarized in Table 2. Four patients (4.3%) developed complications from diverticulitis (1 patient in group 1 [2.8%] vs 3 patients in group 2 [5.45], P = .55). Three patients had bowel perforation, and 1 other patient had bowel obstruction. Only 1 patient died during the study period. She was a 73-year-old patient who died from Enterococcus faecalis sepsis as a complication of an intra-abdominal abscess.
Clinical Factors and Association With Length of Stay (LOS) of Hospitalized Patients.

Abbreviations: BMI, body mass index; MAP, mean arterial press; WBC, white blood cell; CT, computed tomography
Statistically significant (P < .05).
Discussion
Diverticular disease is an abnormal out-pouching of the colonic wall through the muscularis mucosae layer, most commonly seen at the weakest point where the colonic wall receives its blood supply by the penetrating vasa recta. It commonly occurs in the sigmoid colon because of its small luminal diameter. Classic symptoms of acute diverticulitis include left lower quadrant abdominal pain, nausea, vomiting, fever, diarrhea, and a palpable mass.14,15 Acute diverticulitis may progress to more severe conditions, such as peritonitis, abscess formation, colonic perforation, colovesical fistula, pyogenic liver abscess, and pylephlebitis.1,14 Over the past decade, the importance of diverticulitis in younger patients has become more apparent, 16 especially in men and in obese patients. 17 In our study, 39.4% of patients presenting to the emergency department within 1 calendar year were younger than 40 years. There were no overall statistically significant differences in gender, BMI, and ethnicity between the 2 groups. Most of our patients were Hispanic, especially in the younger group (75.7% vs 45.6%, P = .004), which agrees with previous studies (Table 3). 85.1% of the patients had mild diverticulitis based on Ambrosetti’s CT criteria, and 14.9% of the patients had complicated diverticulitis on their CT scans. The diverticulitis occurred in the sigmoid colon (52 patients, 56.4%) and in the descending colon (20 patients, 21.3%). There was no difference between the 2 age groups in location of the diverticulitis (P = .21). There were no differences in vital signs and laboratory values between the 2 groups.
Diverticulitis in the Young: Summary of Previous Studies.

Diverticular disease in younger patients may present a greater clinical challenge than in older patients. It has been reported that younger patients have more severe disease with higher rates of surgical intervention; however, not all studies support this concern (Table 3).1,11,18-21 Freischlag et al 22 reported that emergency surgery in young patients was often secondary to an uncertain preoperative diagnosis and the presumptive clinical diagnosis of acute appendicitis without confirmation by CT scan. Our study demonstrates that younger patients are more likely than older patients to be discharged from the emergency department (56.8% vs 7%; P < .01). However, if they were to be admitted, the younger patients tended to have longer hospital stays than older patients. Although obesity was previously reported as a risk factor, 23 the typical patient with a longer hospital stay in our cohort had a BMI <25 kg/m2, a lower blood pressure at presentation, hypoalbuminemia, physical signs of peritonitis, and complicated findings on CT scan. We observed comparable in-hospital mortality rates in the 2 groups, but longer follow-up is needed to determine recurrence rates and long-term outcomes.
The management of acute diverticulitis usually involves conservative treatment with broad-spectrum antibiotics covering Gram-negative rods (Enterobactericiae, principally Escherichia coli) and anaerobes (Bacteroides fragilis). Suggested antibiotic regimens include either a third-generation cephalosporin and metronidazole or single-agent treatment with second-generation cephalosporins. 14 Fewer than 10% of hospitalized patients require surgical treatment by either 1-stage or 2-stage operation; this is usually indicated in patients with complications, such as undrainable abscess formation, uncontained visceral perforation, generalized peritonitis, fistula formation, failure to respond to medically managed treatment within 3 days, bowel obstruction, CT scan characteristics of Hinchey stage 3 or 4 disease, or, in some cases, recurrence of diverticulitis. Conservative treatment with medical therapy was the main approach in our 2 patient groups.24,25 The most common antibiotic regimen at our institute was the combination of a fluoroquinolone (levofloxacin or ciprofloxacin) and metronidazole. Only 4 patients required surgery.
Our study has some limitations. First, our study is a retrospective study, and the source of information was from medical records. Second, this is a single-center study, and our results may not be generalizable to other patients or health care organizations. Third, the use of ICD codes during emergency department visits might have overlooked patients who presented initially with uncertain diagnoses and were not coded as diverticulitis. Finally, our study did not follow the patients after hospital discharge. Therefore, the rate and severity of disease recurrence and long-term outcomes cannot be determined.
Conclusions
Our study is one of a few studies that have evaluated clinical parameters, management, and outcomes in 2 distinct age groups. We found that diverticulitis occurs in younger patients more frequently than previously thought and that its short-term clinical course is similar to older patients. Clinicians need to consider this diagnosis when younger patients present with acute abdominal symptoms.
Footnotes
Authors’ Note
This article was presented as a poster at the ACG (American College of Gastroenterology) 2012 Annual Scientific Meeting, Las Vegas, Nevada, October 19-24, 2012.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.