
Abstract
Alberta’s Primary Care Networks (PCNs) bring together family physicians and other health professionals to provide local, comprehensive, and readily accessible primary care services to patients. The Edmonton North PCN, one of the largest in the province, piloted the Resource in Clinic (RIC) Program with objectives to increase efficiencies in the use of physician time, increase physician workplace satisfaction, increase unattached/orphan patient access, and decrease patient wait times. An evaluation of the RIC Program employed surveys (completed by physicians with RICs, RIC staff, and patients), log chart recording, and physician billing data and cost analysis. The findings indicated high satisfaction with the model, increased physician visits, and improved access for patient with comorbidities. The study did not demonstrate increased number of patients or new patients, nor could conclusions be drawn related to patient wait times.
Introduction
Primary Care Networks (PCNs) were established in Alberta in 2003 to improve Albertans’ access to health care, increase emphasis on health promotion and intervention strategies, and enhance coordination of care in various health contexts. 1 The Edmonton North PCN is one of the province’s largest PCNs with more than 140 member family physicians providing care to more than 178 000 patients in 50 clinics.
In 2010, the Edmonton North PCN implemented the Resource in Clinic (RIC) Program loosely based on the teamlet model for primary care developed by Bodenheimer and Laing. 2 The RIC Program, a name coined by the PCN, was introduced to optimize physician efficiencies by removing some direct and indirect clinical tasks to allow physicians to spend more time providing care. Similar teamlet models employing health coaches (ie, medical assistants) have been implemented or explored in other primary care settings to better address patient health care needs during brief office visits 3 and enhance care in relation to chronic conditions. 4 A shared approach toward primary care has been suggested to have potential for improving patient–provider relationships. 5
The PCN RIC teamlet model consists of a family physician and a RIC who may be a licensed practical nurse or medical office assistant. The RIC carries out administrative tasks and provides patient triage (eg, verifying reason for visit), clinical support (eg, data entry and mining), patient education (eg, smoking cessation), and patient follow-up (eg, providing test results, booking appointments), as appropriate. The goals of the RIC Program are to increase efficiencies in the use of physician time, increase physician and RIC satisfaction with the team model, improve coordination of care, and improve patient access and wait times. The PCN funded a 2-part evaluation to determine the extent that the RIC Program achieved these goals. In RIC 1, the PCN was responsible for hiring RICs; a policy change implemented in RIC 2 required physicians to hire their own RICs with the PCN reimbursing the doctor for the majority of the cost.
Methods
The RIC Program evaluation formed part of the PCN’s ongoing internal quality improvement process and did not require ethics review. Data collection strategies included the following: tracking dyad time and activities using a log chart template; administering surveys to physicians with RICs, RIC staff, and patients; and analyzing physician billing data (Table 1). A log chart template was completed for a week long period at baseline and final points to capture physician and RIC time performing direct and indirect patient care activities. RICs were responsible for recording the condition of the patient (ie, chronic/complex, healthy/general, or acute/emergent), the type of service provided (ie, consultation, procedure, or routine exam) by which service provider (ie, physician, registered nurse, RIC, or other), and the total time required for the visit.
Resource in Clinic (RIC) Program Evaluation Data Sources.
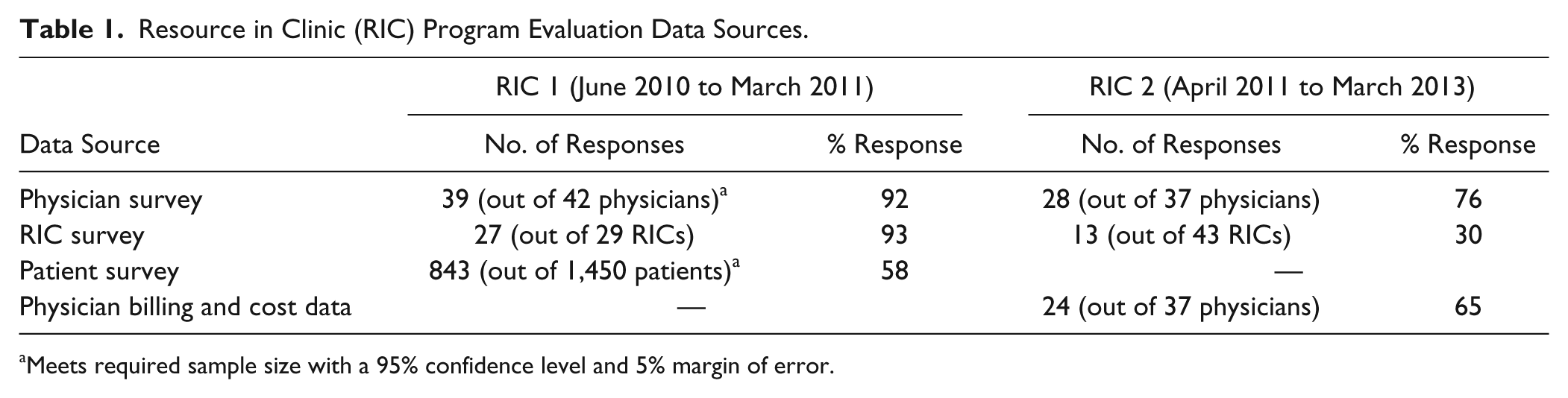
Meets required sample size with a 95% confidence level and 5% margin of error.
Physicians and RICs completed surveys at 2 points (a few questions were added to the second survey iteration). Questions during the first round of physician surveys were embedded within a survey of the entire PCN member physicians, enabling comparison of responses on 3 relevant satisfaction questions. Examples of the log chart template and survey questions asked of physicians, RICs and patients are included in Appendices A and B.
Physician claims data 1 year before and after participating in the RIC Program were requested from Alberta Health for the April 1, 2007 to December 31, 2012 period. The PCN database provided additional data, such as physician and RICs program start dates, as well as the full-time equivalency (FTE) of physicians. Paired t-test mean and sign rank test median statistical analyses were used to compare patient outcomes before and after physician participation in the RIC Program. Billing and PCN data from 24 RIC physicians were included in the analysis (1 RIC physician was excluded for not having early data). Outcomes analyzed using claim data included number of physician visits and revisits, number of regular and new patients, number of patients with comorbidities by type, and number of patients by diagnosis.
Results
Physician Perspectives
According to survey findings, the majority of physicians with RICs expressed satisfaction with the RIC Program overall (93%, 2013; 98%, 2011) and thought the program was important (89%, 2013; 79%, 2011), meeting its intended goals (93%, 2013), contributing to increased work satisfaction (93%, 2013), and resulting in greater efficiency at work (93%, 2013; 90%, 2011). Overwhelmingly, physicians believed the RIC Program helped reduce workload for clinic staff (96%, 2013; 95%, 2011) and that the RICs worked to full scope of their practice (85%, 2013).
Physicians indicated increased satisfaction with the amount of time spent with patients (97%, 2013; 85%. 2011), as well as high satisfaction with teamlet coordination (96%, 2013; 98%, 2011) and appropriateness of patient care (93%, 2013). The majority of physicians claimed to change their patient care delivery practices (86%, 2013; 74%, 2011) and experienced improved patient relationships (90%, 2013; 74%, 2011) through the RIC Program. Physicians believed that the RIC Program decreased patient wait times (86%, 2013) and increased their ability to see new patients (89%, 2013).
According to log chart data, physicians spent less time (baseline 69% to 57% final) in direct patient care and increased time (baseline 23% to 38% final) in indirect patient care (eg, lab reports, referrals). In addition, physicians served more patients daily (baseline, 20, and final, 26).
In open-ended survey responses, physicians felt positive about their ability to hire RICs who best fit with their clinics’ work environment. They noted challenges concerning additional time needed to complete hiring and payroll tasks and mentor RICs to ensure that patients receive accurate information and quality care.
Comparative analysis of relevant survey questions posed to physicians with an RIC and without an RIC revealed a statistically significant difference in perceptions that PCN services have freed up their time to provide more care to their patients (89% positive ratings for RIC physicians; 79% for non-RIC physicians; P ≤ .05). Nonsignificant but positive differences were also found in response to the question “since becoming a member of the PCN, I have felt increased satisfaction in my job” (79% RIC physicians; 70% non-RIC physicians) and the statement that PCN services have resulted in an ability to accept new patients (71% positive for RIC physicians; 37% for non-RIC physicians). The latter difference was not significant because of small sample size.
Resource in Clinic Perspectives
The majority of RICs indicated that they clearly understood their role expectations (85%, 2013; 88%, 2012), believed that their work made a difference (85%, 2013; 92%, 2012), were satisfied with coordination of care between themselves and the physician (92%, 2013), and felt that the RIC Program allows the right health care professional to provide the right service to patients (100%, 2013). Log chart data revealed that 71% of their day was spent in direct and 21% in indirect patient care activities. The most negative survey response pertained to RIC perceptions of whether they were working to full scope of practice (77%, 2013; 63%, 2012). In open-ended survey responses, RICs commented on the challenges they experienced; for instance, becoming more integrated within their clinical setting, improving on time and task management and distinguishing their roles and responsibilities from those of physicians and other staff members. RICs spoke positively about their working relationships with physicians and the meaningful contributions they made to patient care and education.
Patient Perspectives
The majority of patients were aware of the RIC assisting their family physician (94%) and were highly satisfied with the care they received from the dyad (93%). High patient satisfaction was also recorded in relation to RIC communication (86%), as well as physician (95%) and RIC (82%) knowledge of patient health conditions.
System-Level Perspective
In all, 25 of 35 physicians with a RIC consented to participate in an analysis of their billing data; conducted from 1 year before to 1 year after each RIC’s start date (3 years prior data were used for calculation of new patients). Analysis (Table 2) revealed statistically significant increases in the number of visits claimed (average 12% increase per physician FTE), repeat visits claimed (average 18% increase per physician FTE), patients with comorbidity (41% increase per physician FTE), and visits with comorbidities (62% increase per physician FTE). Statistically significant increases in the mean and median number of patients seen per physician FTE were observed for those with diagnoses of mental disorders (average 36% increase), endocrine, nutritional, and metabolic diseases, immunity disorders (31%), diseases of the genitourinary tract (22%), and diseases of the digestive system (17%). No statistically significant difference was found in the mean or median number of patients claimed or the mean or median increase of the number of new patients claimed. The average increase in revenue per physician FTE equated roughly to the average PCN RIC Program cost per physician FTE.
Before–After Changes in Outcomes of Interest. a

Abbreviations: FTE, full-time equivalency; RIC, Resource in Clinic.
Data were available for 24 physicians (representing 22.3 FTEs) for all but one outcome. Number of new patients was based on 21 physicians (representing 19.3 FTEs), as 3 physicians did not have 3 years of data before the RIC started.
Significant at P < .05; **significant at P < .01; ***significant at P < .001 (paired t-test used to compare means and sign rank test used to compare medians).
Discussion
Data were collected over time as the RIC Program became more established at the PCN. The program appears to have improved physician time management, physician and RIC workplace satisfaction, and coordination of care. The evaluation findings demonstrate
high levels of satisfaction among physicians with RICs, RIC staff and patients
enhanced productivity as reflected by increased numbers of patient visits and repeat visits
increased access for patients with complex needs.
Strong support was evident for this model and there was evidence that physicians with a RIC were more positive than physicians without a RIC about their work-life satisfaction and ability to provide more direct care and accept new patients.
The shift in focus on patients with comorbidities may reflect, in large part, the emphasis placed by the PCN and Alberta’s health system, generally, on increasing access to primary care for patients with complex needs; this was one of the primary goals for the establishment of PCNs in Alberta. Of note is that the comorbidities with the greatest improved access correspond directly to the PCN’s emphasis on mental health, diabetes, and weight management. It is difficult to directly and solely attribute this shift to the RIC Program as it may reflect a general shift in practice among Alberta physicians; however, it could be argued that the availability of RIC, by removing some day-to-day routine activities, enabled physicians to increase their focus on more complex patients, in keeping with the desired direction of the health system.
While physicians with RICs perceived that the RIC Program enabled them to see more patients, this outcome was not confirmed in the billing data analysis. Similarly, physicians believed that the RIC Program improved patient wait times; however, this outcome was not quantitatively evaluated, thus firm conclusions cannot be drawn about this outcome.
Conclusion
The RIC Program dyad model of primary care demonstrated positive outcomes that may encourage family physicians to coordinate service delivery with other health providers. This team approach has potential to increase satisfaction for health providers and patients, improve physician efficiencies and enhance access to primary care for patients with comorbidities. Such a model is potentially applicable in all general practice settings and could be replicated in family physician clinics with or without PCN supports.
Footnotes
Appendix A
Appendix B
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.