
Abstract
Keywords
Introduction
The concept of the medical home was developed as far back as the 1960s in pediatrics. The idea was to establish a system of care for the child in partnership with the family and community, to coordinate care and to apply the principles of family-centered care.1-4 This past decade, with opportunities embedded in health care reform, the concept of “patient-centered medical home” (PCMH) has been launched. 5 This model seeks to deliver high-quality care during a dynamic period in US health care history.
Patient-centered medical homes should deliver care that is accessible, continuous, comprehensive, compassionate, family-centered, coordinated, and culturally effective.2,4 The inclusion of these elements can be challenging to a health care system that serves a changing, diverse population.6,7 We are challenged to seek alternative, innovative models of care.
One such model to deliver comprehensive, culturally effective care was developed and involves the integration of community health workers (CHWs) into the PCMH. CHWs have historically and globally played an integral role in the health and well-being of communities. With strong community ties they are uniquely able to help patients navigate systems of care and can serve as peer-educators and supporters.8 -10 They have also been viewed as promising in narrowing health disparities and improving outcomes and access for patients with chronic disease in PCMHs.11 -13
Health disparities in pediatric asthma are well recognized and the use of CHWs has demonstrated improved outcomes although little is known about CHWs in the PCMH setting.14 -16 In 2011, we leveraged the strengths of a proven CHW program to integrate CHWs within PCMHs. The goal was to understand the impact of this integration on the delivery of comprehensive asthma care to predominantly Latino children.
Program
Setting
This study took place in 5 PCMHs in Northern Manhattan that serve a predominantly Latino population. Demographic data of the community reveals that 75% of adults are Latino, 70% speak Spanish, and 43% of children live below the poverty line. The PCMHs have approximately 22,000 patients between birth and 21 years, an asthma prevalence of 18% to 22% and more than 95% are insured by Medicaid. 17 The practices were part of an initiative to achieve National Committee on Quality Assurance (NCQA) recognition as level 3 PCMHs and are staffed by faculty, residents, and a nurse practitioner.
The 8 CHWs are part of a community-academic partnership program working with caregivers of children with high asthma utilization over 1 year. The CHWs are hired by a community-based organization and supervised jointly through a contract with the academic medical center. They connect families to services when obstacles are identified, which compete with families’ ability to manage asthma such as housing and immigration. The CHWs are all female, Latino, bilingual, and are knowledgeable about local resources. 15 They participate in a 2-week CHW training and receive basic asthma education (medications, triggers, integrated pest management, and a modified National Cooperative Inner-City Asthma Study home environmental assessment) by the director. 18
Existing Challenges
As large, urban practices with trainees there were existing barriers in delivering comprehensive care. Care focused largely on medications and due to time constraints and challenges with social circumstances of the population, less time was allotted to risk assessment and education. Few children were referred for care coordination by providers within the PCMHs. Finally, the baseline use of asthma care plans was less than 5%.
Intervention
From February 2011 through December 2013, each CHW was scheduled for 2 sessions (8 hours) per week within each PCMH. CHWs used a peer-based approach to reinforce key messages with families on triggers and control. CHWs received training on the use of the “Asthma 101”, a form developed to document the interaction with families and on how to communicate with staff.
The nurse in-charge served as the liaison for CHWs. CHWs “rounded” on all patients regardless of asthma severity. All PCMH staff helped CHWs identify patients. CHWs met with families prior to or after the visit.
The CHWs documented the encounter by completing an “Asthma 101” form, a copy of which was shared with the team in real-time, to enhance assessment of the families’ asthma. This included the family’s definition of asthma, triggers and how they achieved control. Additionally, CHWs identified and communicated needs for medications or care plans.
In October 2012 providers in 5 PCMHs were surveyed through an institutional review board–approved survey via e-mail using a 5-point Likert scale to assess workflow impact.
Data Sources
Data were collected by the CHWs using the “Asthma 101” screeners, which identified those who received the intervention; educational topics addressed and team recommendations. Also collected were the numbers of referrals to the care coordination program. All data related from the provider survey about PCMH workflow were collected and analyzed.
Results
From February 2011 to December 2013 there were an increasing number of families receiving education and support. Additionally, the number of referrals to the care coordination program increased 7-fold (P < .001). Figure 1 demonstrates these trends over 3 years.
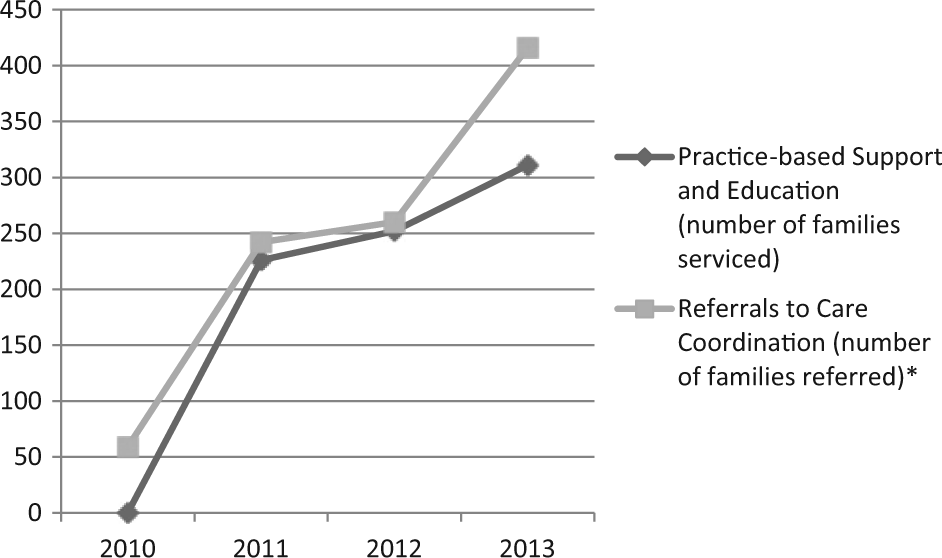
Community health worker outcomes in the patient-centered medical home: 2010-2013.
Surveys were completed by 55 out of 100 providers for a response rate of 55%. Of these, 38% were attendings and 62% were residents with 77% females and 23% males. Table 1 describes the results from the provider survey on the impact of CHW integration. Twenty-two percent reported they did not refer patients for the 1-year care coordination program before the intervention compared with 6% after the intervention. The percentage of providers who reported referring patients to care coordination prior to the intervention increased from 67% to 79%. Thirty-nine percent of providers responded that they gave a care plan when prompted by a CHW. Additionally, 55% responded that they referred patients for CHW education.
Provider Feedback on Community Health Worker Integration Into the Patient-Centered Medical Home: October 2012 (n = 55).

Discussion
The results of this intervention suggest that CHWs can be integrated into PCMHs as valued members of the team and impact comprehensive care delivery. CHWs were able to provide support and education to hundreds of patients. Provider behavior regarding referrals for care coordination changed as a result of the intervention which is supported by increased referrals. Identifying high-risk children with asthma for a 1-year intervention including home visits, education, and resources offers an opportunity for decreased morbidity. Outcomes for participants in care coordination demonstrate decreased emergency department utilization and hospitalizations for asthma resulting in overall improved outcomes. 15 The reported use of care plans increased from less than 5% at baseline to 39% when prompted by a CHW. This demonstrates the benefit of CHWs working with providers to enhance care by raising awareness to the use of this educational tool.
Apart from the impact in care delivery it is also important to understand the process of CHW integration into PCMHs as observed over time. Initially, program leadership received many questions about CHWs and what they added to PCMHs. Multiple meetings with staff were held to discuss the CHW role and their strengths and limitations. CHWs are not well established or licensed in our state and overall few staff was familiar with them. Providers were aware they were part of a care coordination program, but some were hesitant to have them discuss asthma in the “doctor setting.” They were also unsure how to interpret “Asthma 101” forms. These questions and barriers decreased overtime. CHWs were eventually invited to team huddles and PCMH meetings.
Through informal feedback, providers noted that some never interfaced with CHWs because of the schedule. As a result, CHW sessions were adjusted to work with a variety of providers. This was important feedback and demonstrated early impact as the desire of providers to participate and benefit from the intervention was critical. Feedback also included that the “Asthma 101” form was not practical. This led to the development of a note in the electronic medical record and enabled data collection for NCQA reporting.
Little is known about the processes of integrating CHWs into the PCMH and about the impact on outcomes and systems. This study offers insight into the potential for CHWs to affect care and identify high-risk populations for care coordination. As CHWs interact with families they assess and determine which may have high-risk asthma and share this directly with the team. It demonstrates that CHWs can be integrated into PCMHs and that challenges can be overcome through enhanced education and communication. In this case, responding to the concerns of the PCMH team and clarifying roles proved essential to integration. This focus on educating teams about CHWs’ strengths and limitations are essential to attempts by organizations at integration. This study also demonstrates the benefit to organizations of partnering with community agencies as a means toward improved success in establishing PCMHs. Limitations to this study include the lack of feedback from families and the impact CHWs have from their perspective. Additionally, providers’ responses about the use of care plans were limited by self-report. Finally, this intervention occurred during the early stages in PCMHs and it is unclear how other workflow changes could have led to the observations.
Further research is needed to better understand this emerging area. Having a broader understanding of the CHW impact in bridging cultural or language barriers in the PCMH would be of interest as well as better understanding the families’ perspectives on the value of CHWs in the PCMH setting.
Footnotes
Acknowledgements
The authors would like to thank the community health workers who were critical to the success of this integration. We also thank Dr Patricia Hametz for her editorial review of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.