
Abstract
Objectives:
Population health management is becoming increasingly important to organizations managing and providing primary care services given ongoing changes in health care delivery and payment systems. The objective of this study is to show how systems science methodologies could be incorporated into population health management to compare different interventions and improve health outcomes.
Methods:
The New York Academy of Medicine Cardiovascular Health Simulation model (an agent-based model) and data from the Behavioral Risk Factor Surveillance System were used to evaluate a lifestyle program that could be implemented in primary care practice settings. The program targeted Medicare-age adults and focused on improving diet and exercise and reducing weight.
Results:
The simulation results suggest that there would be significant reductions projected in the proportion of the Medicare-age population with diabetes after the implementation of the proposed lifestyle program for a relatively long term (3 and 5 years). Similar results were found for the subpopulations with high cholesterol, but the proposed intervention would not have a significant effect in the proportion of the population with hypertension over a time period of <5 years.
Conclusions:
Systems science methodologies can be useful to compare the health outcomes of different interventions. These tools can become an important component of population health management because they can help managers and other decision makers evaluate alternative programs in primary care settings.
Primary care in the United States is shifting rapidly from a system built around health care delivery to a system focused on the triple aim of improving population health and health care quality while reducing health care costs. 1 As a result, population-based interventions are becoming increasingly important to organizations managing and providing primary care services given that many costly chronic health conditions are preventable and that their prevalence may be driven by modifiable health behaviors such as physical activity, nutrition, and smoking. 2
Population health management (PHM) is “a set of interventions designed to maintain and improve people’s health across the full continuum of care—from low-risk, healthy individuals to high-risk individuals with one or more chronic conditions.”3,4 In primary care practice settings, proactive PHM would include identifying subpopulations of patients who need to be targeted for interventions, examining the characteristics of these populations, creating reminders for patients and providers, tracking performance measures, and making data widely available for clinical decision making at the practice level. 5 Although there are effective PHM strategies to identify population cohorts, conduct risk stratification, and monitor clinical and cost metrics, practical PHM tools to evaluate what would happen to populations after the implementation of different treatment protocols or facing different intervention scenarios are very limited. 6 These PHM tools could be useful to managers in health care systems and community health organizations interested in optimizing decision making to achieve targeted health outcomes, improve health care quality, and reduce costs.
Systems science is an interdisciplinary field that studies complex systems.
7
Modern systems science methodologies—such as network analysis, system dynamics, and agent-based modeling (ABM)—are widely used to study complex emergent phenomena in the social and behavioral sciences.8,9 A 2010 report from the Institute of Medicine proposed that the US Department of Health and Human Services (HHS) should
coordinate the development and evaluation and advance the use of predictive and system-based simulation models to understand the health consequences of underlying determinants of health. HHS should also use modeling to assess intended and unintended outcomes associated with policy, funding, investment and resource options.
10
ABM stands out among all the different systems science approaches currently in use because it is based on the development of individual-level rules of behavior and, as such, facilitates the modeling of disease progression and results in a natural representation of populations (eg, individual agents’ behavior can be synthesized and aggregated to define and understand population outcomes). 11 Applications of ABM in population health and other related fields can be found in several recent literature reviews.8,12-14
The purpose of this study is to assess how systems science methodologies in general and ABM in particular can be used to fill this gap in practice-based PHM. ABM allows us to track disease progression for a cohort of individuals, akin to the way PHM takes place in primary care practice settings. We use the New York Academy of Medicine Cardiovascular Health Simulation (NYAM-CHS) model to evaluate what would happen to short- and long-term health outcomes if a primary care practice serving a population of insured adults aged ≥65 years (ie, the Medicare-age population) implemented a lifestyle program to improve diet and exercise and reduce weight. We also compare the results for 3 key subpopulations: the Medicare-age populations with diabetes, hypertension, and high cholesterol.
Research Design and Methods
We used data from the Behavioral Risk Factor Surveillance System (BRFSS) to identify the health and demographic profile of the population to be simulated with the NYAM-CHS model.15,16 The BRFSS is a telephone survey conducted yearly, and it includes adults aged ≥18 years living in households in the United States. The survey includes standard core questions related to preventive health practices and chronic health conditions. We extracted demographic characteristics and health profiles for the US Medicare-age population (ie, insured adults aged ≥65 years) and 3 subpopulations (the US Medicare-age populations with diabetes, hypertension, and high cholesterol). We selected these populations because they are groups of interest to managers and other decision makers in organizations focused on the delivery of effective primary care (eg, patient-centered medical homes, Medicare Advantage plans, accountable care organizations).
The variables selected included age, sex, and whether the respondent was a current smoker, had a normal weight (body mass index [BMI] < 25 kg/m2), was physically active (had >150 min/wk of moderate physical activity), had a healthy diet (ate ≥5 fruits or vegetables per day), did not have diabetes, hypertension, or high cholesterol, and had no history of myocardial infarction (MI) or stroke. Using the 2007 BRFSS data, we estimated the mean and standard deviation of age for insured adults aged 65 to 94 years (inclusive) and the proportion of each category for all the other variables. After excluding respondents with missing data, the sample sizes were 104,670 for the insured population aged ≥65 years and 19,321, 60,678, and 52,912 for the subpopulations with diabetes, hypertension, and high cholesterol, respectively.
The NYAM-CHS model is a joint ABM effort from a multidisciplinary team of experts in health services research, health economics, and systems science. The model allows the simulation of different behaviors and health conditions over time. 17 ABM has been shown to have unique advantages over other systems science methodologies (eg, discrete-event simulation, system dynamics models) in terms of the capabilities of modeling detailed individual-level behaviors and health outcomes and capturing demographic heterogeneity.18,19 Other strengths of ABM include the ability to represent stochastic variability in input variables and parameters and the possibility of including history dependence in state transitions as well as agent interactions. 20 ABM has been used widely in social sciences, but health applications have been limited mostly to modeling infectious disease and addictive behaviors.13,21-23
In the NYAM-CHS model, each agent (person) is defined according to 7 behavior and health factors (ie, smoking, physical activity, healthy diet, healthy weight, cholesterol, blood pressure, and blood glucose) as well as by age, gender, and having a history of MI or stroke. These factors were selected on the basis of the concept of ideal cardiovascular health developed by the American Heart Association, which is defined as not having cardiovascular disease while also having optimal levels of the 7 factors described previously. 24 Each agent’s behavior and health factors evolve simultaneously and interactively as time progresses in the model. The predictive validity of the model has been assessed by comparing simulated and actual health outcomes using nationally representative data from the BRFSS. 25
The NYAM-CHS model was used to assess health outcomes over time for a primary care practice serving a population of insured adults aged ≥65 years. The health outcomes of the model resulting from normal health progression were compared with the health outcomes obtained from implementing a lifestyle program designed to reduce by half the proportion of the population eating <5 fruits and vegetables per day, exercising <150 min/wk, and having BMIs ≥ 25 kg/m2. Examples of potential interventions that are consistent with our simulated comprehensive lifestyle program and can be delivered in primary care settings include the Evaluation of Lifestyle Interventions to Treat Elevated Cardiometabolic Risk in Primary Care, the 5 A’s framework (ask, advise, assess, assist, arrange), and other nutrition and physical activity health promotion programs highlighted in recent systematic reviews.26-29
Results
Table 1 reports the population characteristics for the 2007 BRFSS insured population aged ≥65 years and the 3 subpopulations described in the previous section. The mean age is about 74 years for the Medicare-age population and the 3 subpopulations. The proportion of nonsmokers is between 91% and 93% for the Medicare-age population and the 3 subpopulations. The proportion of the population with BMIs < 25 kg/m2 ranged from a low of 20.63% for the subpopulation with diabetes to a high of 32.25% for the subpopulation with high cholesterol. About one-third of Medicare-age adults (33.05%) were physically active (ie, were doing >150 min/wk of moderate physical activity), whereas this rate was lower for the 3 subpopulations studied (eg, only 25.65% of the subpopulation with diabetes was physically active). The proportion of the population who followed a healthy diet (ie, ate ≥5 fruits or vegetables per day) is between 26% and 29% for the Medicare-age population and the 3 subpopulations. The proportions of the population with no diabetes, no hypertension, and no high cholesterol for the Medicare-age population were 80.39%, 41.82%, and 49.41%, respectively. The proportions of the Medicare-age population with histories of MI or stroke were 13.26% and 8.41%, respectively. The 3 subpopulations selected had much higher proportions of history of MI or stroke than the general Medicare-age population.
Population Characteristics from the 2007 BRFSS.

Abbreviations: BMI, body mass index; BRFSS, Behavioral Risk Factor Surveillance System; MI, myocardial infarction.
Table 2 reports the simulated results of the 3 key health conditions for the Medicare-age population and the 3 subpopulations. We compared the normal progression of these health conditions with a proposed comprehensive lifestyle program designed to reduce by half the proportion of the population eating <5 fruits and vegetables per day, exercising <150 min/wk, and having BMIs ≥ 25 kg/m2. One-, 3-, and 5-year end points were used to evaluate the effect of the comprehensive lifestyle program on health progression over the short, medium, and long terms. One-tailed, two-proportion z tests were conducted to assess whether the changes in health conditions were statistically significant.
Simulated Population Health Outcomes (n = 10,000) for Normal Health Progression and Comprehensive Lifestyle Program a .
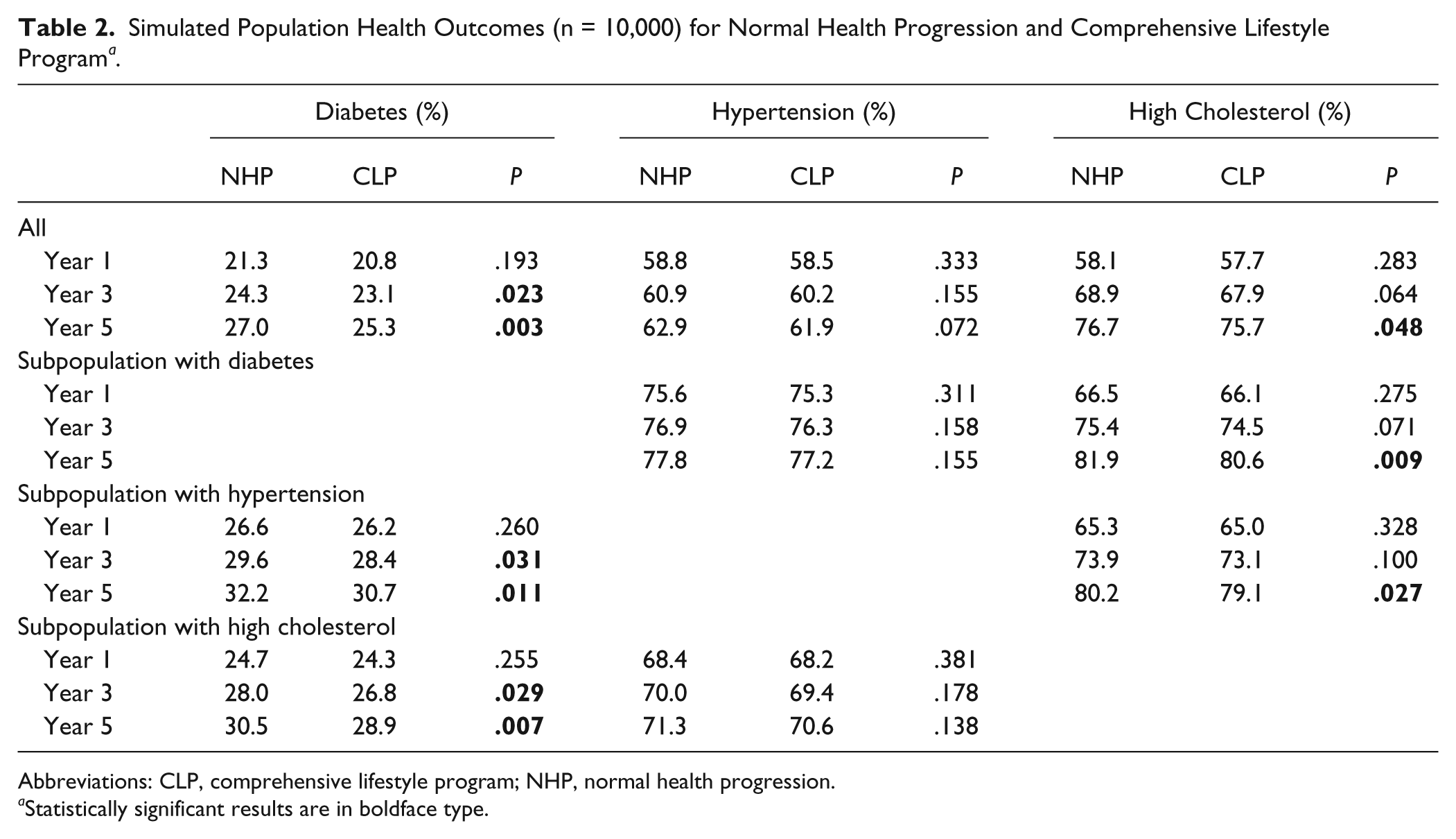
Abbreviations: CLP, comprehensive lifestyle program; NHP, normal health progression.
Statistically significant results are in boldface type.
As Table 2 shows, there were significant reductions in the proportion of the population with diabetes (p<.05) after the lifestyle program was implemented for the medium and long terms (three and five years) for the Medicare-age population and the two subpopulations with hypertension or high cholesterol. A significant reduction in the proportion of the population with high cholesterol was also observed after the lifestyle program was implemented for five years. However, the NYAM-CHS Model predicts that the proposed lifestyle program would not have a significant effect in the proportion of the population with hypertension over a time period less than five years.
Discussion
PHM strategies to help managers and other decision makers optimize health care processes are becoming increasingly important in primary care settings given changes in health care delivery and payment systems that emphasize value and accountability for targeted populations. Interventions targeting chronic health conditions that can be prevented or managed using PHM approaches are particularly important because they can lead to substantial cost reductions if they are well designed. 4 PHM in primary care includes a broad set of effective strategies (eg, identifying patient subpopulations for targeted interventions, creating reminders for patients and providers, tracking performance measures), 5 but PMH tools that managers and other decision makers can readily use to evaluate how different treatment interventions would work in a given population are needed.
In this study, we showed how systems science methodologies could be used to evaluate interventions and programs for different populations in primary care. We did this using the NYAM-CHS model and looked at health outcomes within a hypothetical primary care practice serving a population of insured adults aged ≥65 years. The NYAM-CHS model is interactive and lends itself to PHM in primary care settings in the sense that it allows users to describe a specific population on the basis of a set of basic demographic and health characteristics, and then it permits the tracking of population health outcomes over a given period of time. The model can help primary care providers identify subpopulations of patients who need to be targeted for interventions and evaluate health outcomes of different interventions to achieve PHM goals.
Although there are important limitations to this work (eg, systems science models may not be able to predict all outcomes accurately given limited data and information about how different health behaviors and factors interact in real life; more external validation work is needed; undiagnosed cases in health conditions such as diabetes and hypertension, as may be the case with BRFSS data, may bias results in clinical settings), we have shown how systems science models can be used to enhance PHM as it is currently used in primary care practice. We analyzed health outcomes over time, but the model proposed here can be expanded to include cost and quality-of-life outcomes (to compare the costs of different interventions, conduct cost-effectiveness analysis, and identify whether a given intervention is worth paying for), to allow interaction among individuals and capture social network and area effects, and to develop better ways to make the simulation results more useful to primary care practices by improving how these results are visualized and reported.
In the end, systems science models will become increasingly attractive to primary care practices interested in PHM approaches, but the rate of adoption of these models will be driven by the continued development of new payment and reimbursement systems, together with the availability of information technology resources and specialists doing applied work in the intersection between PHM and systems science modeling.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.