
Abstract
This pilot study examined the effectiveness of a 4-month clinic-based dietary intervention emphasizing the intake of deep yellow and dark green vegetables versus usual care on improving diet quality in postpartum women. The intervention group (n = 31) received 1 face-to-face nutrition education session with a registered dietitian, 2 follow-up phone calls, and 3 pamphlets distributed by mail. The usual care group (n = 25) received handouts with guidelines on healthy eating. Dietary outcomes were assessed from 3-day food recalls and evaluated using paired and independent t tests. Intervention women exhibited a significant increase in total vegetable intake (P < .001) and in dark green and deep yellow vegetables (P < .001). In comparison, the control group increased the intake of total vegetables (P < .001), but did not increase the consumption of dark green and deep yellow vegetables. When comparing the change in intake between study groups for both types of vegetables, the difference was not significant. Furthermore, 61% of the intervention women met the goals for total vegetable intake compared with 12% for the usual care group (P < .001). The intervention group also had a greater percentage of women (25.8%) that met the goal for deep yellow and dark green vegetable intake when compared with the usual care group (8%; P < .08). These results suggest that postpartum women are receptive to nutrition education and that nutrition education can influence vegetable intake.
Introduction
During postpartum, it is critical for women to develop healthy eating patterns to adequately support breastfeeding, optimize weight, and become a good role model to their children. 1 Previous research shows that postpartum women often quit the healthy eating patterns that they may have formed prenatally.2,3 In another study, it was found that less than 30% of mothers at 6 months after birth were eating the amount of fruits and vegetables per day recommended for postpartum women. 4 Therefore, there is a need for interventions tailored to the specific nutritional needs of postpartum women that emphasize a diet based on caloric balance and rich in nutritious foods.
Recently, the Academy of Nutrition and Dietetics (formerly the American Dietetic Association) and The American Society for Nutrition have recommended that women of reproductive age receive counseling on the importance of developing healthy eating habits, including the postpartum period. 5 Studies have shown that the postpartum period can be an opportune time to provide resources and motivation for dietary changes because women are more connected to health and nutrition services due to follow-up doctor’s appointments. 4 However, those opportunities are usually tempered by the challenges of motherhood such as the demands of a new infant, stress, lack of sleep, and pressure to go back to work. 6
In a systematic review of lifestyle interventions in postpartum women, van der Pligt et al 7 found that theory-based interventions were more effective than empirical interventions to affect dietary change; that there was a noticeable difference in the success of interventions based on the timing of intervention delivery (interventions ranged from 24 and 48 hours postdelivery and up to 12 months postpartum); and that home-based interventions via telephone or mail are less burdensome than attending regular meetings. While most of the studies included in this review focused on lifestyle interventions to limit postpartum weight retention, little is known about dietary interventions to increase diet quality in this period. Therefore, there is a need to determine if the postpartum period is an appropriate time for nutrition education.
This pilot study was designed to assess the effectiveness of a dietary intervention in overweight postpartum women on improving diet quality. The intervention focused on vegetable intake within the context of a healthy diet because vegetables are naturally low in calories and rich in nutrients, fiber and water. It was hypothesized that women who participated in the dietary intervention would be more likely to improve the quality of their diet, including a greater intake of vegetables, compared with women who received usual care.
Methods
Study Design
Subjects were assigned to one of two groups: intervention and usual care. The study was conducted between 2 and 6 months after delivery. Baseline measurements were recorded for both groups within 2 weeks of recruitment, which occurred at the 6-week follow-up with an obstetrician, and posttreatment assessment took place 6 months after delivery. All participants gave written informed consent and study procedures received institutional review board approval where the study was conducted.
Participants
Women 18 to 40 years old were invited to enroll by an obstetrician at 6 weeks postpartum through a large obstetrics clinic in the Cincinnati metropolitan area. Mothers who had a postpartum body mass index <25 kg/m2, history of a prior preterm infant or multiple birth, high risk pregnancy, in vitro fertilization, lack of medical clearance from a physician to participate, received prior maternal nutrition education, or were on special diets were excluded. Sixty-six women were randomly assigned to 1 of the 2 groups; intervention (n = 35) and usual care (n = 31).
Dietary Intervention
Intervention Group
The social cognitive theory 8 provided the theoretical basis for the 4-month dietary intervention. The intervention emphasized various aspects of the theory, including clear expectations (improve diet quality and health), environment (availability of vegetables), self-efficacy (choosing vegetables in a variety of settings), and self-monitoring (tracking weekly vegetable intake). The goals of the nutrition education were (a) eat at least 5 servings of vegetables daily (1 serving = one-half cup to one cup depending on vegetable type) and (b) choose at least 2 servings of deep yellow (carrots, squash, and sweet potatoes) and dark green vegetables (green beans and peas).
To accommodate the lifestyle of a new mother, the intervention consisted of 1 face-to-face education session with a registered dietitian, 2 follow-up phone calls, and distribution of 3 pamphlets that were mailed at regular intervals to the mother’s home. The 60-minute nutrition education session took place in the obstetrician’s office approximately 2 months after delivery, a convenient location for the mother. The topics covered during the session integrated strategies to improve knowledge and skills, eating habits, food choices, and self-monitoring related to increasing vegetable intake. Two follow-up phone calls reviewed the mother’s food choices from monthly vegetable intake logs and helped the participants set new goals for increasing vegetable intake. In addition, 3 pamphlets were distributed by mail throughout the intervention, which presented supplemental information such as recipes and shopping lists.
Usual Care Group
The usual care group received handouts with guidelines on healthy eating. Formal dietary education sessions, phone calls, and pamphlets were not included in this usual care group.
Measures
A registered dietitian conducted three 24-hour food recalls to obtain dietary data from both groups. Recalls were randomly collected over a 1-week period at baseline and 6 months postpartum. Dietary intakes were analyzed using the University of Minnesota’s Nutrition Data System for Research (software version 2010, Nutrition Coordinating Center, University of Minnesota, Minneapolis), and were used to determine the level at which the participants adhered to dietary goals of the intervention. Participants were trained during recruitment in the use of a poster with shapes and sizes of food 9 in an attempt to minimize food recall errors and enhance accuracy of food volumes and dimensions.
Statistical Analysis
Descriptive statistics were used to summarize age, race, education level, height, weight, and body mass index. Paired t tests were used to examine changes in vegetable consumption between pre- and posttests for both groups. The differences in the changes between intervention and usual care groups were compared using independent t tests. Vegetable consumption was also analyzed using percentages and χ2 statistics to compare those who met dietary goals in each group at the 6-month point.
Results
Fifty-six women completed the study (31 intervention and 25 usual care; 85% retention). Reasons for discontinuing the study included lack of time and relocation. There were no demographic differences between participants that discontinued the study and those that completed the study. Table 1 shows demographic data of the study sample. Mothers were between 29 and 31 years old, white, and completed college.
Descriptive Statistics for Baseline Demographic Characteristics of the Study Participants.

Table 2 shows changes in vegetable intakes for the intervention and usual care groups. In the intervention group, the number of total vegetable and dark green and deep yellow vegetable servings increased significantly (P < .001) from baseline to postintervention. However, in the usual care group, only the number of total vegetable servings increased significantly (P < .001). There were no significant differences in total and dark green and deep yellow vegetable servings when comparing the change in intake between groups. At postintervention, a significantly greater percentage of the intervention group met the goal of 5 total serving of vegetables. Sixty-one percent of the intervention group had an intake of 5 or more servings of vegetables compared with 12% in the usual care group (P < .001). Although it was not statistically significant (.82), the intervention group had a greater percentage (25.8%) of women meet the goal of 2 servings of either deep yellow or dark green vegetables when compared with the usual care group (8%).
Three-Day Mean Dietary Intake.
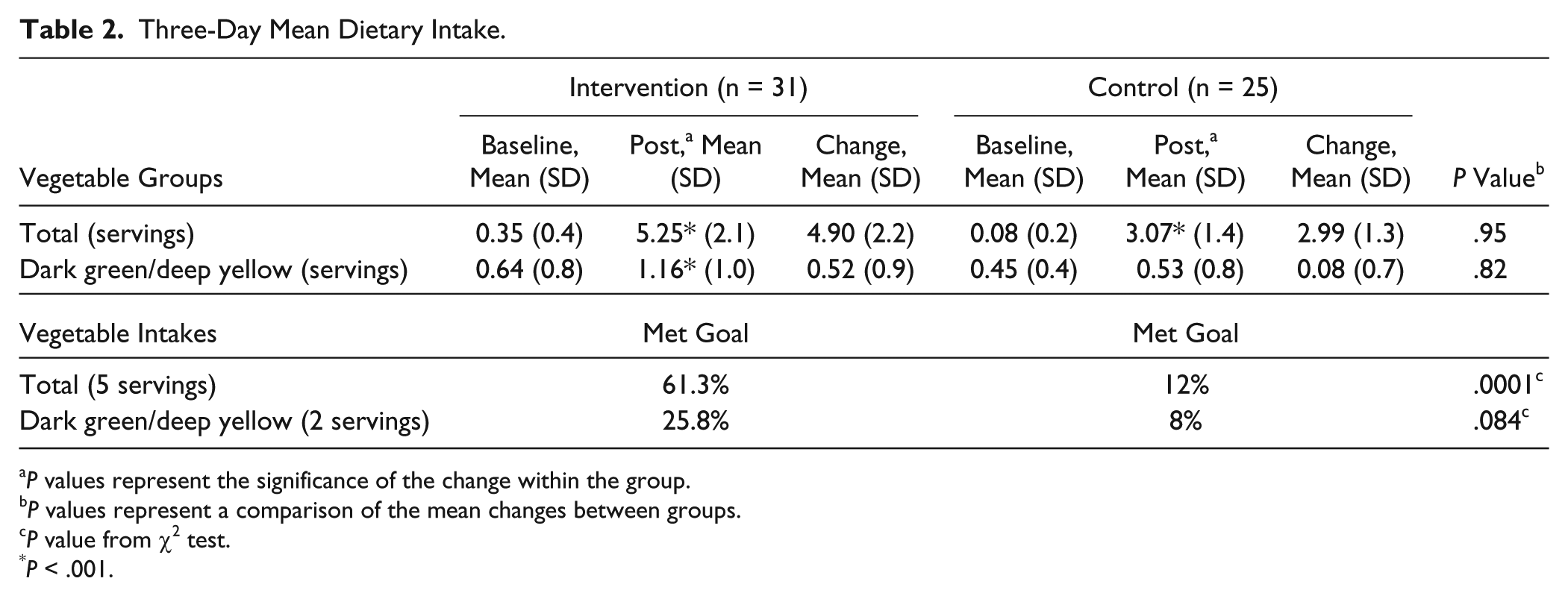
P values represent the significance of the change within the group.
P values represent a comparison of the mean changes between groups.
P value from χ2 test.
P < .001.
Discussion
This pilot study provides evidence to support an association between a dietary intervention emphasizing vegetables and the subsequent improvements in vegetable consumption of postpartum women, thus recognizing the postpartum period an effective teachable time. Mothers in the intervention group consumed significantly more servings of total and deep yellow and dark green vegetables, while the usual care group experienced a significant increase in total vegetable intake only. This study’s findings agree with a systematic review on nutrition interventions to increase vegetable intake that resulted in an average increase of 0.39 servings of vegetables per day. 10 Importantly, when intervention mothers were compared to control mothers, a higher percentage of intervention mothers met the goals for total vegetable intake and there was a trend toward significance for dark green and deep yellow vegetable intake.
Previous research has indicated that development of a suitable intervention that can fit seamlessly into the busy lives of new mother’s remains a challenge. 4 This study’s intervention suggested that theory-based nutrition education that is administered with minimum face-to-face contact during regular doctor’s visit coupled with telephone and mail delivery was suitable for mothers. Also, our intervention suggests that nutrition education administered in the first 6 months postpartum was effective in increasing vegetable intake.
A limitation of this study was that the sample was not representative of all overweight postpartum women. The study included predominantly white, highly educated women; therefore additional data are needed from various socioeconomic levels and ethnic backgrounds. For future studies, the duration of the intervention should be considered if the goal goes beyond vegetable intake and diet quality, such as improving maternal weight.
In conclusion, this study suggests that the early postpartum period is an appropriate time for dietary intervention. These findings suggest that nutrition education may be an important adjunct to postnatal care.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.