
Abstract
Introduction
The negative health impacts following teen pregnancy and the benefits of routine preventive health care are well known to health care providers. What remains unclear is whether young mothers are receiving preventive health care following their pregnancy, and if so, who is providing this care. Previous research has shown young mothers want to be seen by a consistent provider, to be counseled on birth control, and to be screened for sexually transmitted infections and depression.1-3 However, because of barriers, this population has a difficult time accessing and continuing with comprehensive medical care. Barriers to care included living in poverty, lower education level than adult mothers, frequent phone service interruptions, higher likelihood of depression, decreased access to medical care, lack of health insurance, feelings of lower self-esteem, and poor parenting skills.1(p448),2(275),4-6 With regard to health care for their infants, young mothers are more likely to seek regular care in emergent/urgent care settings and less likely to utilize preventive care visits. 7
Sedgwick County is a mid-sized, urban area and compared with state-wide data, adolescent rates of pregnancy in this county are high. In 2009, the county had 35 pregnancies per 1000 10- to 19-year-olds as compared with 26 per 1000 in all of Kansas. Unfortunately, while the state-wide rate has decreased over recent years, the rate of teen pregnancy overall in Sedgwick County has increased. 8
This increased rate of teen pregnancies leads to a growing population of vulnerable young mothers in need of comprehensive medical care; however, no studies to our knowledge have addressed whether local young mothers are receiving health care. Although there are many providers who are capable of providing comprehensive medical care to young mothers, it is unclear who, if anyone, is providing regular routine health care to this population and whether demographic factors influence this care.
Methods
We developed a 24-question, paper survey that was approved by a local institutional review board. Postpartum mothers aged 12 to 21 years were eligible to participate. Surveys were administered prior to discharge at a single hospital where 75% of local infants are born. Providers with delivering privileges at the hospital were asked permission to include their patients in the study and none excluded their patients from the study. Surveys were reviewed by a panel of experts in the fields of obstetrics and gynecology (OBGYN), pediatrics, and family medicine. Nondemographic questions focused on the health care that the young mother received prior to getting pregnant and her intentions for future health care now that she was a mother. No incentives were offered to the participant for completing the survey. If a young mother was not available to immediately participate in the survey, the researcher offered to leave the survey in her room or reapproach her at another time.
Survey frequencies and percentages were calculated for all responses. Chi-square analysis was used to compare age (<18, 18, 19, 20, 21 years) and race (white, Hispanic, black, and other) with ability to identify a regular physician when not pregnant, having seen a physician in the past 3 years and receipt of minor emergency medical care during pregnancy. Responses of “no” and “don’t know” were combined.
Results
Surveys were completed by 146 young mothers. Respondents were mostly white, with a mean age of 19.5 years (Table 1); 22.6% (33) had graduated or earned their high school equivalent. The majority (52.7%; 77) of young mothers surveyed could identify a primary care provider (PCP) prior to their pregnancy and 68.5% (100) had seen their PCP in the 3 years preceding their pregnancy (Table 2). Of the PCPs identified, 54.1% (79) were family physicians, 7.5% (11) pediatricians, 24% (35) OBGYNs, 7.5% (11) indicated an “other” specialty, and 12.3% (18) could not identify the specialty of their PCP. During their pregnancy, 45.9% (67) reported receiving minor emergency medical care.
Demographics of Participants.

Comparison of Health Care–Seeking Behavior According to Age and Race.
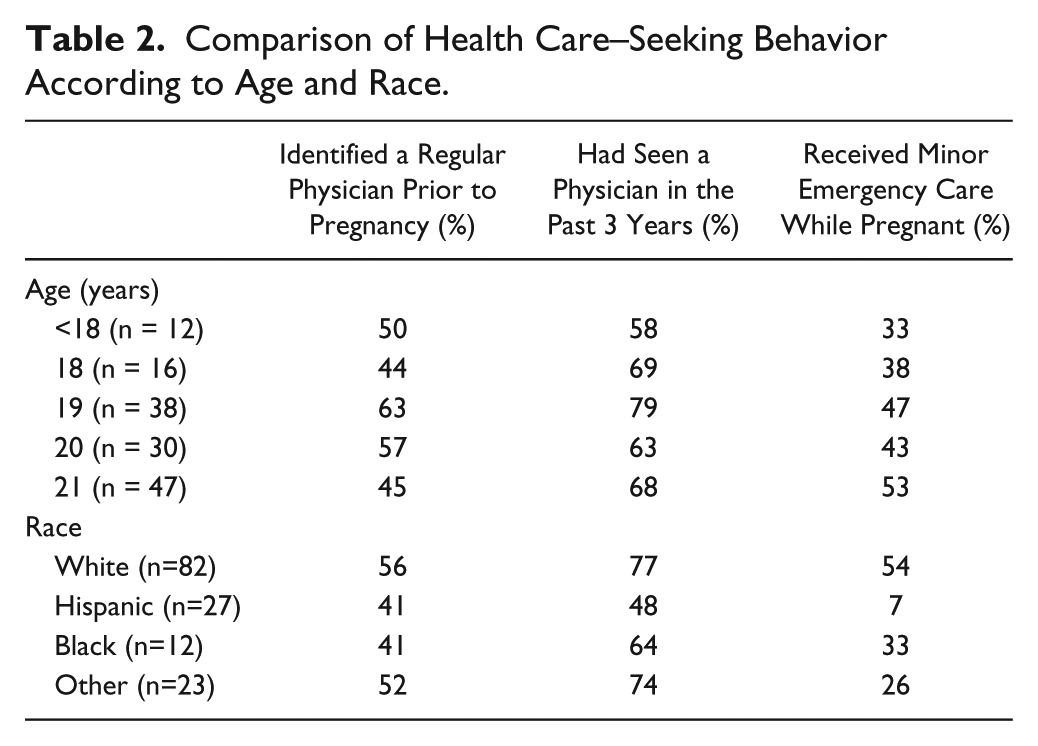
In subgroup analyses, white mothers were significantly more likely than Hispanic to report having seen a physician in the 3 years preceding pregnancy (P = .040). White mothers were also significantly more likely than Hispanic mothers or mothers of other ethnicity to have received minor emergency care while pregnant. Black mothers were significantly more likely than Hispanic mothers to have received this care (P < .001).
Age was not significantly related to ability to identify a regular physician when not pregnant (P = .461), having seen a physician in the past 3 years (P = .579), or receipt of minor emergency medical care while pregnant (P = .675). Race was also not significantly related to ability to identify a regular physician (P = .555). Only a minority of participants planned on receiving preventive health care from pediatricians (5.5%, 8), family physicians (17.8%, 26), or OBGYNs (48.6%, 71) after pregnancy. A greater proportion of participants planned on seeing pediatricians (12.3%, 18), family physicians (67.8%, 99), or emergency department physicians (16.4%, 24) when they were ill. Only 7.5% (11) planned to see their OBGYN for acute visits. Eleven percent (16) had not thought about their future health care (Figure 1).

Mothers’ plans for health care.
Discussion
The results of this study suggest young mothers lack plans for utilization of regular preventive primary health care. Only half entered parenthood with regular health care, and once they became mothers, few planned on receiving routine preventive health care. Based on the results of this preliminary study, young mothers tended to identify OBGYNs as their source of routine care most often and pediatricians least often. Furthermore, this research suggests that adolescent mothers are more likely to plan for acute types of health care than they are to plan for preventive health care visits for themselves.
To our knowledge, this is the only study to date that has attempted to measure the intentions for preventive care utilization of young mothers for their own health care. One other study measured the effects of home visits on linkage to primary care for adolescent mothers. About half of participants in that study could identify a personal physician at the 2-year postpartum mark, which is consistent with our results, but in that study the type of physician was not identified.4(p228) Our findings that young mothers are more likely to plan for acute types of health care complement previous studies. Adolescent mothers have been shown to be more likely to access care for their infants in urgent care type settings and less likely to utilize preventive care services.8,9
Our study had a number of limitations, including the vulnerable time after delivery during which the study was administered. We chose this time period for 2 reasons. First, our study population is known to be transient with frequent changes in contact information and we wanted to have a representative sample of young mothers. Second, we did not want to risk biasing our sample by surveying mothers already engaged in care for themselves or their infants or who were participating in community programs. Another unanticipated limitation was that the majority of the participants were in the 18- to 21-year age-group, which may have skewed our data away from pediatric primary care. We had no respondents from the 12- to 14-year-old age range though 4 infants were born to mothers in that age range during our study period.
Despite these limitations, the findings of this study spotlight the lack of consistent preventive care intentions for young mothers. These findings are important because they show young mothers are more likely to plan for acute care visits than preventive visits for themselves, thus making it important for the provider to use the time spent in an acute visit to either link the patient to a PCP or provide comprehensive preventive care. Also, because nearly half of young mothers plan to see their OBGYN routinely, this specialty has an opportunity to either provide comprehensive preventive care to this population, or to connect young mothers with other PCPs. Future studies should explore the components of health care young mothers receive from specific primary care specialties and strategies to increase use of a medical home in this population.
Footnotes
Acknowledgements
The authors wish to acknowledge Joy Nimeskern, Leenah Abugisisa, Lindsay Blick, and Teolinda Milsap, MD, who contributed to the project.
Authors’ Note
Research from this project was presented in poster format at the Association for Reproductive Health Professionals National Conference in September 2013 and the corresponding abstract was published in the August issue of Contraception.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by a grant from the Kansas Bioscience Authority and the Wichita Center for Graduate Medical Education (QW850023).