
Abstract
Background
The prevalence and consequences of severe obesity among children are subjects of increasing concern.1,2 While the health effects of moderate levels of obesity vary across outcomes and demographic groups, individuals with more severe levels of obesity have consistently been found to experience a wide range of negative health effects. 3 Children treated for severe obesity often have multiple risk factors for cardiovascular disease, 4 and in adults severe obesity increases the risk of mortality, 1 and is correlated with hypertension, diabetes mellitus, 5 and other morbidities.5,6 Gender, age, socioeconomic status, and racial/ethnic group are associated with the prevalence of severe obesity in preschool-aged children in disadvantaged population groups. 1 There are relatively few data available on the prevalence of severe levels of obesity in children of different ages and in different populations, 7 in part because of evolving definitions of the levels of overweight and obesity. 8 To our knowledge no recent data have been published on the association between severe obesity and high blood pressure among children in primary care.
The purpose of this study was to examine the prevalence of severe obesity and its association with high blood pressure measurements in children aged 3 to 17 years who use Philadelphia Health Centers.
Methods
The study population was a randomly selected sample of Philadelphia Health Center patients aged 3 to 17 years with a well-child care visit during the calendar year 2010. Demographic data were obtained from electronic records, and height, weight, and blood pressure values were extracted from medical records by trained researchers for a randomly selected well-child care visit during 2010.
Body mass index (BMI) percentiles were calculated using growth charts published by the Centers for Disease and Control and Prevention. 9 Individuals with a BMI ≥35 kg/m2 or ≥120% of the 95th percentile were classified with severe obesity. 8 Blood pressure was classified using the formula suggested by the National High Blood Pressure Education Program Working Group on High Blood Pressure in Children and Adolescents. 10
Bivariate analyses were performed using exact tests to measure the association of BMI and blood pressure status with age-group, gender, race/ethnicity, and insurance status. Multivariate analysis was carried out using PROC SURVEYLOGISTIC in SAS version 9.2 (SAS Institute, Inc, Cary, NC) to adjust for clustering within health centers.
The study was approved by the Philadelphia Department of Public Health Institutional Review Board.
Results
Of the 4829 eligible patients, 800 charts were audited; 691 had height and weight data for the computer-selected date of visit. All but 4 of the 691 patients with height and weight data also had a measured blood pressure. The sample population was evenly divided by gender and 58% African American, 16% Hispanic, 4% non-Hispanic white, 8% Asian, and 14% other or unknown race/ethnicity. More than one third (35%) of patients were uninsured, 56% were covered by Medicaid, and 9% were privately insured (see Table 1).
Patient Characteristics, Severe Obesity, and Elevated Blood Pressure Measurements.

The prevalence of severe obesity in the sample was 7.7% (95% confidence interval = 5.8% to 9.9%). The prevalence of elevated blood pressure measurements was 17.5% (95% confidence interval = 14.7% to 20.5%). Differences in the prevalence of severe obesity between demographic groups were not statistically significant. High blood pressure measurements were significantly more common in teenagers (25%) than in younger children. Asian and white children had the highest frequency of high blood pressure values (28%) while Hispanics had the lowest (11%). In bivariate analyses, differences were statistically significant for Asians and Hispanics. High blood pressure values were over twice as frequent among children who were severely obese compared with the total population (38% vs 17.5%, respectively). High blood pressure values were recorded for 25% of obese and 23% of overweight children (see Figure 1).
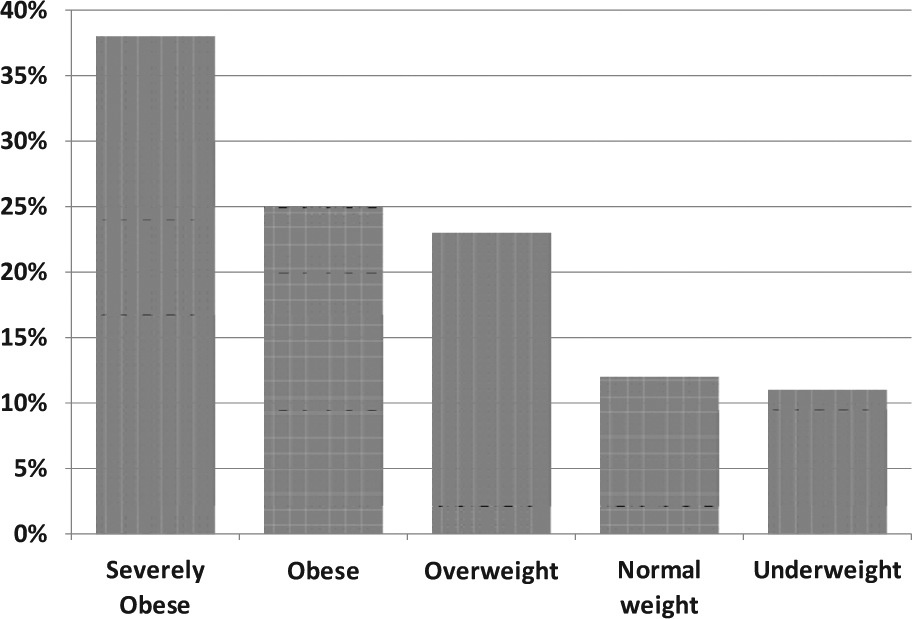
Elevated blood pressure values by weight status, Age 3 to 17 years, Philadelphia Health Centers, 2010.
In multivariable analyses, severe obesity and older age-group were independently associated with high blood pressure measures, while racial/ethnic differences were not statistically significant.
Discussion
The association between obesity and high blood pressure in children is well established, 11 but to our knowledge, the frequency of high blood pressure measurements among severely obese and other children in primary care have not recently been presented. The association in this urban, low-income, primarily minority patient population was strong, with 38% of severely obese children having high blood pressure values recorded.
The appropriateness of routine blood pressure screening for pediatric patients is controversial. 12 In 2008-2009, a national sample indicated that blood pressures were recorded in two thirds of preventive care pediatric visits. However, among children who were diagnosed as obese, this proportion rose to 84%. 13 This study establishes neither the proportion of severely obese patients with persistently elevated blood pressures, nor the long-term consequences of screening blood pressures for any patient population. 12 But it does provide evidence that the proportion of patients with blood pressure levels of concern is substantially increased among severely obese children.
The associations examined here are with a single measurement of blood pressure taken in a clinical setting. There is substantial intraperson variability in blood pressure, especially in children, so this variable would not justify a diagnosis of hypertension. 12 In research conducted in school settings, fewer than one third of children with elevated blood pressures on one occasion had elevated blood pressures on 2 subsequent occations. 14 Other limitations include the retroactive use of data recorded by health care professionals at 8 different sites with potential for inconsistency in measurement between health centers. Blood pressures were measured by health center nurses (and occasionally repeated by physicians) using manual equipment, including a range of cuff sizes for children, and nurses were trained to use appropriate size cuffs and have the child sit quietly for several minutes before taking the measurement. In the context of busy health centers, we cannot ensure that these policies were universally adhered to, and failure to ensure a resting period could have increased the frequency of elevated blood pressure measurements, Such inaccuracies in measurement do not seem likely to have been differential by weight status, so they would most likely reduce the apparent magnitude of the association with severe obesity. Having a sample limited to patients with well-child care visits and excluding patients without complete data creates some potential for selection bias.
Strengths of the study include having a large sample of children from a disadvantaged public health center patient population, including substantial representation of racial and ethnic minorities. The height and weight data were measured by health center nurses, providing more accurate information than self-reported data. The overall prevalence of severe obesity in this sample (7.7%) is similar to that found among local public school children in the 2009-2010 school year (7.9%), 15 suggesting that it is reasonably representative of the population. The prevalence is higher than that found among members of Kaiser Permanente Southern California in 2007-2008 (6.4%), 16 suggesting that severe obesity may be more prevalent in disadvantaged inner-city children.
The study results show that severe obesity affects almost 8% of children in this disadvantaged patient population, across all demographic groups, and that among these children, more than one third also exhibit high blood pressure values that further increase their health risks.
Pediatric health care providers play a key role in managing comorbidities associated with childhood obesity, including an emerging co-epidemic of obesity-related hypertension. If elevated blood pressure readings continue, appropriate blood and urine tests need to be ordered; additional tests (eg, looking for specific kidney and cardiovascular disorders) should be considered. If blood pressure measurements do not return to a normal range, exercise and dietary recommendations, possibly including sodium intake limits, may need to be made. Referrals to specialists such as pediatric nephrologists or pediatric cardiologists may be sought, and medications may be needed for blood pressure control.
Further research should clarify whether physicians should take additional measures to detect and treat hypertension in the presence of severe obesity in children. Interventions at all levels to prevent and treat child obesity remain a critical public health priority.
Footnotes
Acknowledgements
The members of the Philadelphia Health Centers’ Pediatric and Adolescent Continuing Quality Improvement Committee contributed to the conception and completion of the study, which could not have been carried out without their contributions.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.