
Abstract
Introduction
Children’s healthy development is influenced by parents’ ability to obtain primary health care services, including preventive care, immunizations, screenings, and annual well-child visits. Estimates of the number of children who attend all recommended well-child visits and receive comprehensive preventive care at those visits, range widely from a low of 37% to a high of 81%.1-3 While studies have found evidence that the lack of health insurance is a significant barrier to children’s receipt of preventive care, 4 no studies to our knowledge have studied other barriers particular to working parents. This is an important gap in the literature. The vast majority of parents (75%) of children younger than 18 years are working at a paid job, 5 and while some pediatricians’ offices have begun offering extended hours for nonurgent care and preventive visits, most still provide this care during the day when most employed adults are at work. While older children could potentially transport themselves, the vast majority of children younger than 18 years cannot obtain preventative care without an adult to accompany them to a clinic or doctor’s office. In this study, we use a unique, unexplored, nationally representative survey to examine whether employed parents report they are able to meet their children’s preventive health needs, and how working conditions affect their ability to do so.
We focus on 4 workplace policies that would potentially enable working parents to attend preventive, well-child visits. We examine the ability to make or receive a phone call during work hours because of parents’ need to schedule preventive care appointments when offices are open which is still primarily during the daytime, and since most offices still set up appointments by phone (and not e-mail or other mode of communication that could be accessed in the evening or night). We also examine parents’ scheduling flexibility using 2 measures, the ability to change the time one starts or ends a workday and the ability to set one’s regular schedule, which have been examined as supports for meeting employee health needs6-9 but could similarly facilitate meeting the health needs of employees’ children. Finally, because studies of working parents have demonstrated that the ability to use formal flexibility policies (regardless of reason for use) is often determined by the preferences of one’s supervisor,10-12 we also examine the role of having an accommodating and supportive supervisor.
Methods
Participants
We analyze responses from a sample of 917 currently employed parents of a child younger than 18 years living in their household from the Work, Family, and Community Nexus survey, a random-digit dial, nationally representative survey designed to assess the impacts of working conditions on family and community well-being. The Work, Family, and Community Nexus survey was administered in English and Spanish to 4200 US adults aged 18 to 69 years in 2006 and had a response rate of 60.1%. The data were weighted by gender, race, region, and educational attainment using data from the US Census’ Current Population Survey. See Table 1 for descriptive statistics for the sample.
Sample Description.

Outcome
The outcome examined was the inability to respond to children’s preventive health care needs based on responses to the following question, “How often have you been unable to meet children’s preventive health care needs such as immunizations, annual check-ups, or help with daily treatments?” which had 4 response categories: never, sometimes, frequently and always unable. We also examine a simplified 2-category version which collapses sometimes, frequently, and always unable into a single unable to meet preventive health needs category.
Working Conditions
In this study, we examine a series of workplace policies hypothesized to be important to working parents’ ability to meet their children’s routine care needs using the following question:
For each of the following policies can you tell us whether it is available to people at your workplace to use: (1) without any penalty or cost at work, (2) with a small penalty or cost at work, (3) with a large penalty or cost at work, or (4) not available at all? (Note: A small penalty or cost, for example, means a person’s supervisor being unhappy with you and a large penalty or cost means, for example, a person might risk sacrificing future promotions.).
This question was asked for: (1) “Ability to set your regular work schedule,” (2) “You are allowed to change your starting and quitting times if the need arises,” (3) “While at work, you are allowed to make personal calls without consequences,” and (4) “Your supervisor accommodates you when you have family or personal business to take care of.” Because of survey length constraints, some workplace conditions were asked of only a random half of the sample, including the question regarding the ability to make a phone call.
Analysis
We analyzed the relationship between parents’ work conditions and their ability to care for children’s preventive health needs first using a χ2 test of association and then using multivariate logistic and ordered logistic regression analysis. The regression models include: respondent’s marital status, education level, and gender, spouse’s education level, household income, and number of children in the household, as well an indicator for whether there was an adult or caregiver in the home who is not working or in school full-time who could potentially meet the child’s preventive health care needs. Information about the pediatrician’s office hours was not available. To confirm that all 4 working conditions could be included in the same model without risk of mis-estimation of their effects due to correlations, Pearson correlation coefficients were calculated; none exceeded 0.38. Of the 917 working parents, 781 had complete data on all variables in the regression models. Eighty-seven cases were excluded because of missing income data, and 49 for other missing data. This represents a relatively low nonresponse rate on income compared to other national household surveys.
Multivariate logistic models were first run using the dichotomous dependent variable for being unable to meet children’s preventive health needs (constructed from the original 4 response categories as described above). The full model was also run using an ordered logit regression analysis where the dependent variable was the original 4-option variable to test the robustness of the findings. In each case, 2 models were estimated. The first model was run on the full sample of working parents and included 3 of the 4 workplace policies that are the focus of this article while the second model was run on approximately half of the sample of employed parents because it also includes an indicator for access to a fourth working condition, ability to make personal phone calls during work time, which was asked of a random half of the sample (because of survey length constraints). Finally, to examine the hypothesis that workplace flexibility policies are more important when children are definitively reliant on an adult to get them to the doctor, we estimated a model on a sample of working parents whose children were younger than 12 years, an age below the youngest legal driving age in the United States, and when taking public transportation or walking alone to see a doctor would be less common.
Results
In the sample of working parents, 13% reported that they were unable to meet their children’s preventive health care needs often, some or all the time. Bivariate analyses of the association between workplace conditions and inability to meet children’s preventive health care needs are reported in Table 2. All 4 of the schedule flexibility and workplace supports were significantly associated with less inability to meet children’s preventive health care needs (all Ps ≤ .002).
Bivariate Analysis of Whether Parents With Access to Workplace Flexibility Policies at Little or No Cost Are Less Likely to Report Being Unable to Meet Child’s Preventive Health Needs.

Results from our multivariate logistic regression models are presented in Table 3. Model 1 includes the 3 flexibility measures asked of the full sample. Model 2 was run on approximately half of the sample of employed parents and includes the ability to make personal phone calls during work time, which was asked of a random half of the sample. Results from model 1 show that being able to set one’s own schedule was associated with a reduction of nearly half of the odds of a parent’s being unable to respond to their child’s preventive health care needs (odds ratio [OR] = 0.59, P < .05). In model 2, which also includes the ability to make personal phone calls during work time, schedule control remained statistically significant and the association was even larger in magnitude (OR = 0.399, P < .05). Being able to make personal calls while at work cut the odds of being unable to meet a child’s preventive care needs by half (relative to the odds for working parents without access to these policies at work; OR = 0.44, P < .05). In model 1, the odds of being unable to meet a child’s preventive care needs for working parents who have an accommodating supervisor (OR = 0.587, P < .05) were nearly identical in magnitude to the odds for parents who are able to set their schedule (OR = 0.596, P = .067). Other significant variables include marital status variables and household income. Parents who are divorced or never married have more than twice the odds of saying they are unable to meet the preventive health care needs of their children (OR = 2.27 and 3.72, respectively, P < .05 in both cases). Though small in magnitude, higher annual income reduces the odds of being unable to respond to their children’s preventive health care needs. For every $1000 increase in annual income, the odds being unable to ensure a child’s preventive health needs are reduced by 1%, and by extension for each $10 000, the odds are predicted to fall by 10% (P < .001).
Logistic Regression Model Predicting Whether Working Parents Are Unable to Meet Children’s Preventive Health Care Needs.
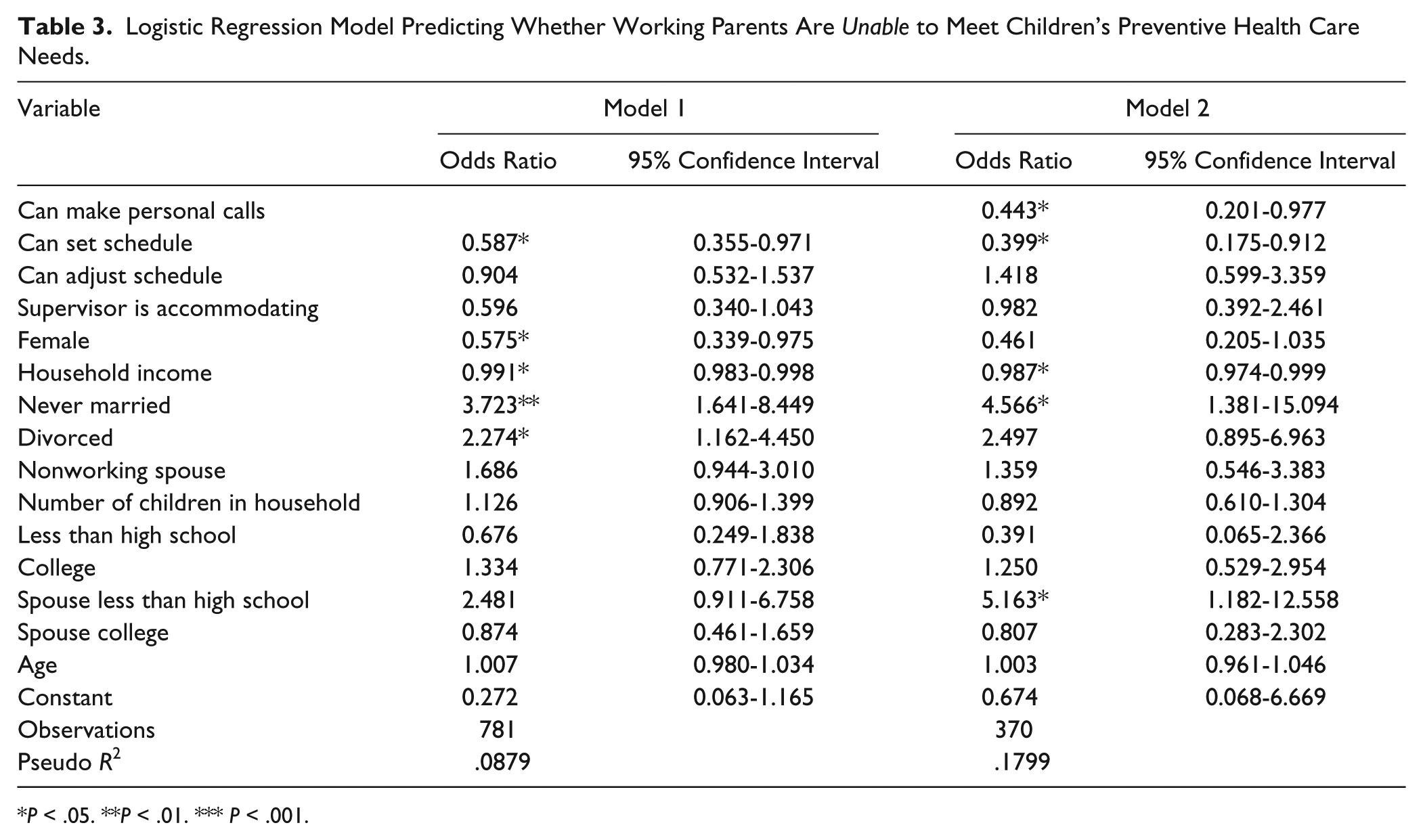
P < .05. **P < .01. *** P < .001.
The odds ratio and statistical significance of the policy variables in the ordered logit analysis are similar to the binary logit (results not shown).
Results from a model run on a sample of working parents whose children were younger than 12 years and would be dependent on an adult to obtain preventive care also supported the importance of working conditions. There were no substantive differences between the magnitude of the coefficients in this model and in the model run on all working parents although because of the smaller sample in this model, standard errors were larger and statistical significance was reduced.
Discussion
Despite a wealth of evidence showing the importance of preventive care to child and youth health status13,14 and the benefits of parental participation in children’s care,15-21 prevention of illness22,23 and injury,24,25 millions of children each year do not attend preventive care visits and many parents face constraints to ensuring their children receive preventive health services because of their work schedules. This study demonstrates that when working parents are allowed accommodations by their supervisor including being able to make personal phone calls while at work and having schedule flexibility, they are significantly less likely to report being unable to meet their children’s preventive health needs.
The hours when physicians see patients often coincide with parents’ work schedules making it necessary for parents to take time off when their children need to see a provider. The only federal policy addressing family health needs in the United States, the Family and Medical Leave Act, does not cover care for preventive or routine health needs despite the benefits of making it more feasible for parents to ensure their children avoid getting potentially serious diseases and receive timely care for routine, minor illnesses. Three states now have paid family leave policies but none would facilitate parents’ ability to obtain preventive care for their children. Paid family leave in New Jersey provides 6 weeks of paid leave for a serious health condition or bonding with a new baby but preventive care (outside of that which is obtained during the time immediately following the birth or adoption) is not covered. The paid leave program in California has a 7-day waiting period before benefits begin so indeed, routine and preventive care could not be covered. The recently passed paid leave legislation in Rhode Island provides 66% of pay (up to a ceiling) for up to 4 weeks to care for an “ailing” family member but as written (detailed regulations have not been written) would not cover preventive care such as annual physicals, screenings, immunizations, and so forth.
Legislation guaranteeing access to paid sick days, short-term leave to address and recover from an illness or to care for a family member with an illness, now in place in the state of Connecticut and the cities of San Francisco, Washington, DC, Seattle and Portland, Oregon, is likely to be a better vehicle for covering preventive care needs. Connecticut’s law specifically allows workers to use accrued days for “preventative care”, and the San Francisco law enables workers to use short-term leave for “medical appointments” and “health issues” in addition to injuries and illnesses. once sick days are accrued (90 days after hire date), there is no statutory waiting time before the sick days can be used making the time off potentially available for addressing preventive, routine health needs. Earlier research finds that having paid leave is one of the most important predictors of whether working parents can stay home to care for their child when he or she is sick. 26 It is likely that this leave would also help with preventive and routine care.
Having the ability to make work schedule adjustments provides important flexibility to many working parents, and is associated with lower odds of being unable to meet children’s preventive health care needs. However, from the standpoint of assisting workers balance work and family needs, it is not as beneficial as paid sick days because it either requires making up work hours or taking unpaid leave, each of which can present problems to parents working long hours for little pay.
Also valuable would be changes in pediatric care practice. A growing number of pediatric offices have begun to offer evening office hours, which would reduce the conflict for those parents who work a daytime schedule. Health care providers, clinics, and private practice managers could also consider accommodations such as taking patient questions by e-mail, for example. Pediatric primary care professionals play an essential role in promoting children’s and adolescents’ health by providing important preventive care including well-child exams, advice on disease and injury prevention measures, immunizations and screenings. Primary care providers need to be concerned with whether parents can fully utilize this care and information. If workplace policies or the lack thereof make it difficult to get to or speak with doctors, children’s health and well-being will suffer. Pediatric primary care providers can make a large difference by supporting workplace policies that allow parents to make adjustments to their schedule and contact health care providers during the work day.
Footnotes
Acknowledgements
We are grateful for the support from the Alfred P. Sloan Foundation and the American Association of Retired People. We are indebted to Jeff Hayes for his assistance with data management.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The development of the Work, Family, Community Nexus Survey was supported by the Alfred P. Sloan Foundation and the American Association of Retired People.