
Abstract
Introduction
Polypharmacy is frequently defined as the excessive or unnecessary use of prescription or nonprescription medications and is associated with drug therapy problems and adverse side effects. 1,2 Drug therapy problems are defined as undesirable events or risks experienced by the patient secondary to drug therapy that inhibit or delay the patient from achieving the desired goals of therapy. Classification of specific drug therapy problems includes problems with drug indication, effectiveness, safety, and patient adherence and has been described in detail previously. 3 Drug therapy problems have been estimated to account for more than $76 billion in annual health care expenditures. 4
Most published research describes polypharmacy in geriatric populations; however, information on medication use in the general population is limited. 5 -8 Identifying risk factors for polypharmacy will help physicians and pharmacists in primary care practices identify patients who would benefit from medication therapy management, improve quality of care, decrease adverse consequences, and decrease the costs of care. To our knowledge, there have been no studies using electronic medical record data to evaluate medication use in a general population of patients receiving care in primary care clinics. Our aim in conducting this study was to characterize the level of medication use by age-groups, demographics, and diagnoses for a large group of patients receiving services in a network of primary care clinics through evaluation of electronic medical record information.
Methods
Sample and Study Population
The study sample consisted of patient demographic and medical data drawn from the University of Wisconsin Department of Family Medicine clinical data warehouse (CDW), a database of electronic medical record information from 22 primary care clinics across the state of Wisconsin. The CDW has been in use since 2005 and provides comprehensive information regarding patients seen at these clinics including: medication use, medical diagnoses, demographic information, and biometric data. We analyzed a sample of de-identified data for all adult patients listed in the database on November 15, 2011. The study received exemption from the Health Sciences Institutional Review Board. To ensure that medication records were accurate, the sample was limited to adult patients who had medication records documented as reviewed by clinic staff within the past 6 months. Patient comorbidities were chosen for analysis based on aggregate data, generated by the CDW, of the most common conditions in the patient population and conditions shown to be associated with greater use of medications in previous studies. 2,8 -11
Outcome Measure
Similar to previous population studies of polypharmacy, medication use was categorized into three groups: level 1 medication use was defined as 0 to 4 medications, level 2 as 5 to 9 medications, and level 3 as ≥10 medications. 10,12 We adopted a broad definition of medication, including all prescription drugs, over-the-counter drugs, vitamins and supplements, and herbal preparations, similar to prior epidemiological studies of medication use. 12 A complete listing of all medications taken by patients in our sample was reviewed to exclude nonmedication items such as testing supplies. Topical preparations, both prescription and over-the-counter, with low likelihood of systemic effects were also excluded.
Independent Variables
Several demographics and comorbidities were analyzed for association with level of medication use. Information on patient age, gender, smoking status, marital status, employment status, race, number of patient encounters within the past year, and body mass index (BMI) were obtained from the clinical database as documented in the patient’s chart on November 15, 2011. Major comorbidities data were obtained based on the International Classification of Diseases, Ninth Revision diagnostic codes shown in Table 1.
Major Comorbidities.

Statistical Analysis
Statistical analyses were performed using SPSS Version 19. Missing data for BMI, marital status, race, and smoking status were imputed. A multinomial logistic model was fit to the imputed data using forced entry for known predictors of multiple medication use based on previous literature and backward stepwise method for the remaining independent variables. Age categories were based on standard US Census cut-points. Insurance status was broken down into subcategories with the employer-provided insurance as the reference category. Models were fit for a single Medicare variable and with separate classifications for patients older than 65 years receiving coverage as an entitlement versus those younger than 65 years because of disability. Odds ratios for age categories changed significantly between models. Because our database does not allow for identification of disabled individuals beyond insurance status, separate Medicare classifications were used in the final model.
Results
Sample demographics, major comorbidities, and health metrics of the population studied are shown in Tables 2 and 3. Patient records analyzed in this study totaled 114 012.
Study Population, by Age-Group and Gender.

Study Population: Demographics and Comorbidities.
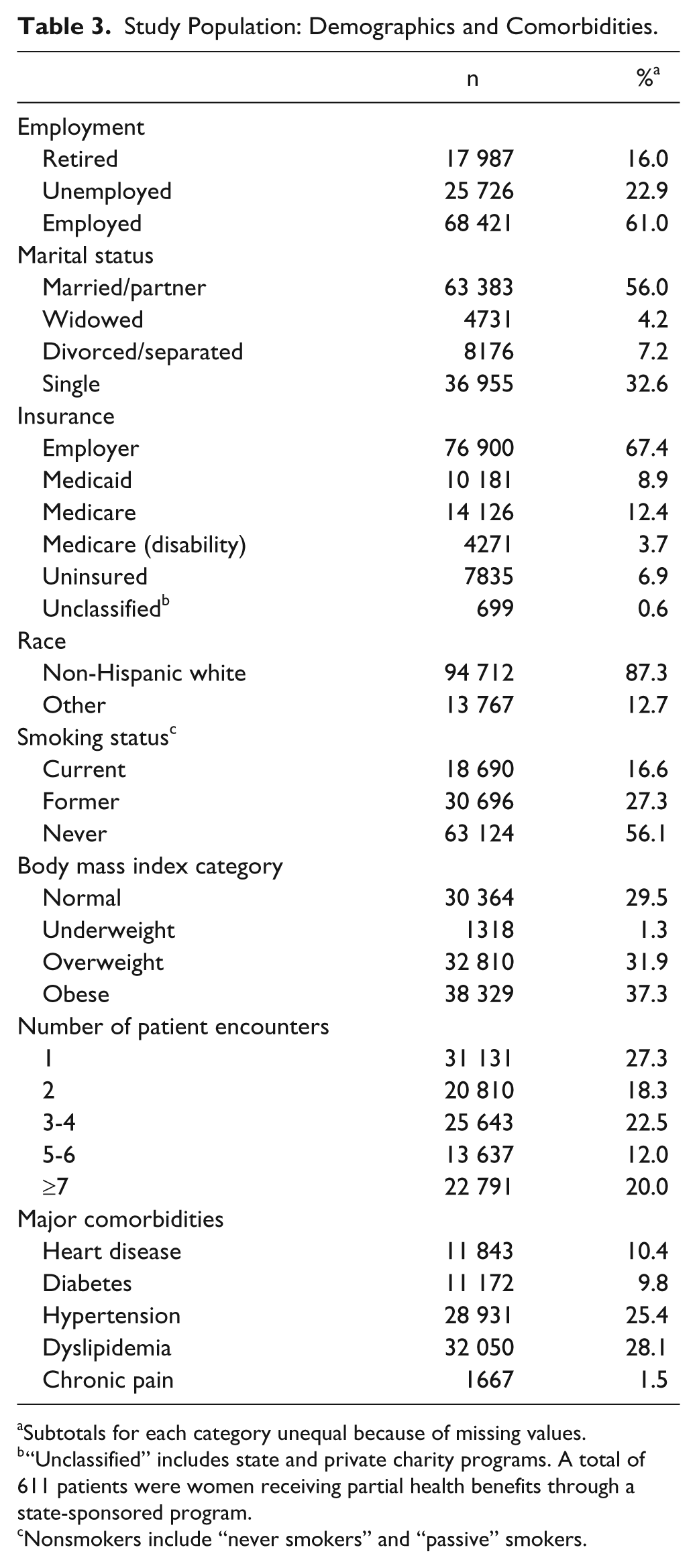
Subtotals for each category unequal because of missing values.
“Unclassified” includes state and private charity programs. A total of 611 patients were women receiving partial health benefits through a state-sponsored program.
Nonsmokers include “never smokers” and “passive” smokers.
Table 4 shows the patient characteristics at each level of medication use. Figures 1 and 2 provide the level 1, 2, and 3 medication use in different age-groups and reveal that the amount of medication used increased with age for both men and women. In the 18- to 24-year-old group, 15% (male) to 23% (female) used more than 5 medications per day; this increased to 85% to 89% in the 75- to 84-year-old cohort.
Number (n) and Percentage of Patients With Various Levels of Medication Use According to Demographic Variables, Body Mass Index, Number of Patient Encounters, and Major Comorbidities.
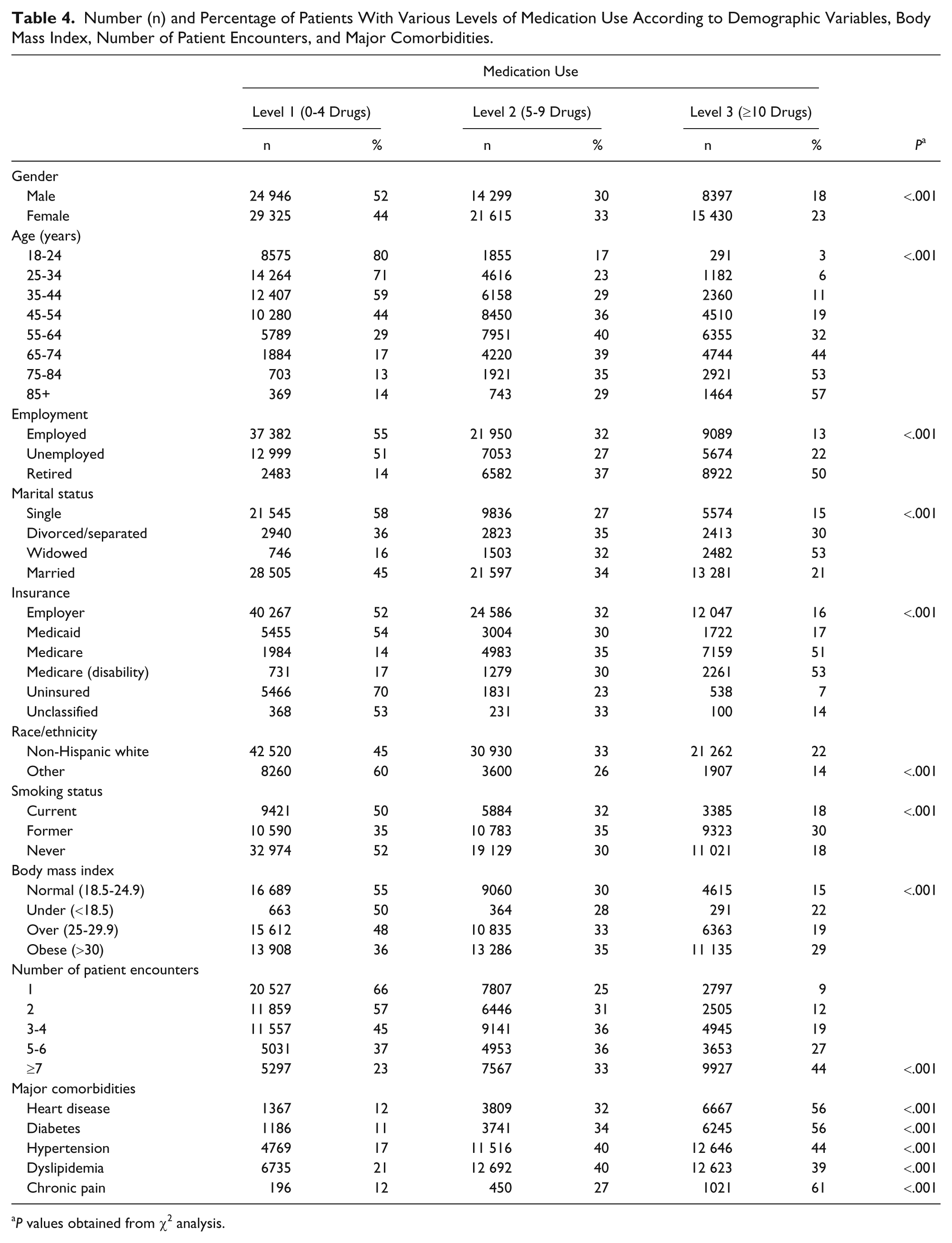
P values obtained from χ2 analysis.

Medication use for men, by age category.
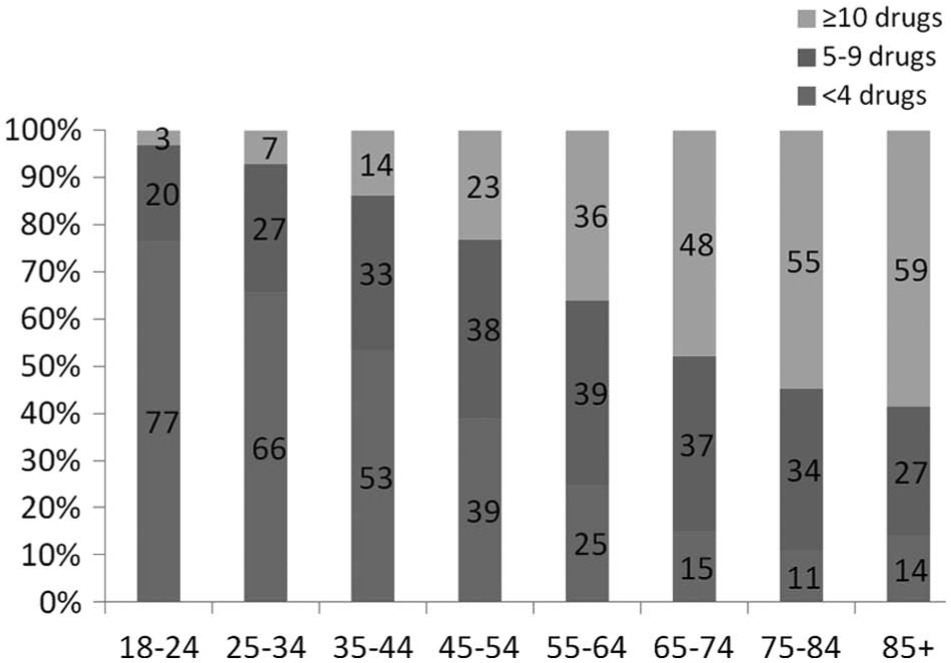
Medication use for women, by age category.
Table 5 shows the results of the regression analysis. Female patients were more likely to have level 2 (odds ratio [OR] = 1.76) and level 3 medication usage (OR = 2.73) compared with men. ORs began to decline after age 75 years for level 2 use and after age 85 years for level 3 use (Table 5). All comorbidities increased the odds of level 2 and level 3 medication use. Of those evaluated, a diagnosis of chronic pain had the highest odds of both levels 2 and 3 use compared with other comorbidities (level 2 OR = 2.56; level 3 OR = 6.40). Level 2 and level 3 medication use increased with the number of patient encounters. Lack of insurance was associated with lower medication use (level 2 OR = 0.74; level 3 OR = 0.47) compared with patients with employer-provided insurance. Patients with Medicaid were more likely to use medications compared to employer-provided insurance (level 2 OR = 1.09; level 3 OR = 1.20) as were patients with Medicare either as entitlement by age or through disability (Medicare, level 2 OR = 1.12, level 3 OR = 1.32; Medicare via disability, level 2 OR = 2.22, level 3 OR = 4.91).
Determinates of Medication Usage in Multinomial Logistic Regression.
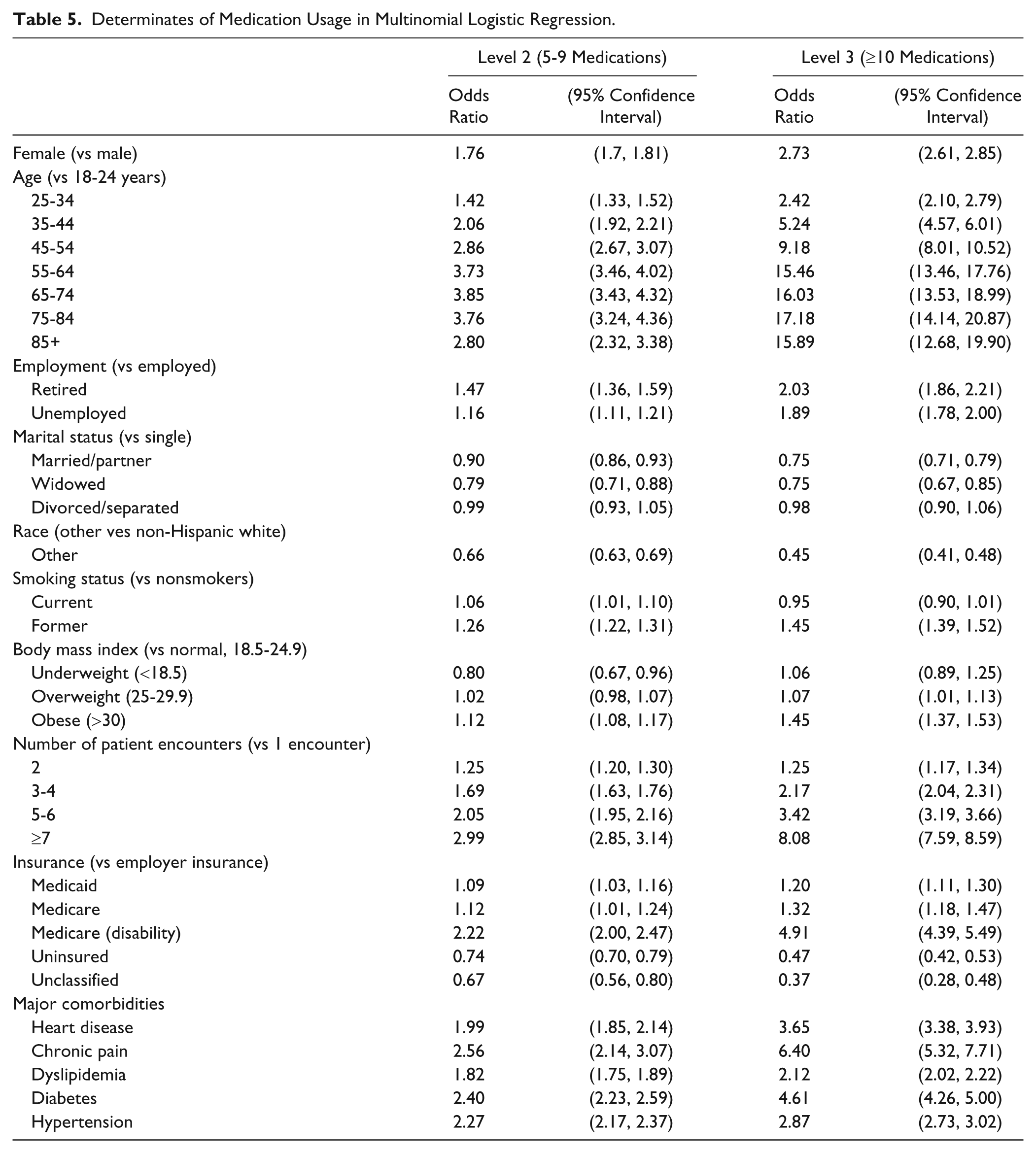
Underweight individuals (BMI < 18.5) had lower likelihood of level 2 use (OR = 0.80) and no statistically significant increase for level 3 use compared with patients with a normal weight (BMI = 18.5-24.9). Overweight patients had no statistically significant increase in level 2 use but were more likely to have level 3 (OR = 1.06) usage, whereas patients with BMI > 30 had increased for both (level 2 OR = 1.12; level 3 OR = 1.45) compared with patients with normal BMI.
Unemployed and retired patients showed higher level 2 and level 3 use compared with working individuals. There were no statistically significant findings for separated or divorced patients compared with single individuals, but married and widowed patients had lower use of medications overall compared with single patients. Non-Hispanic white patients had higher rates of level 2 and level 3 medication use than patients from other racial and ethnic groups. Former smokers were at more likely to use greater amounts of medications compared with never-smokers (level 2 OR = 1.26; level 3 OR = 1.45) and current smokers showed increased rates for level 2 (OR = 1.06) use, but no statistically significant increased risk for level 3 use.
Discussion
This study provides evidence that use of 5 or medications is prevalent across all adult age-groups, including the younger cohorts receiving care in primary care clinics. We found that in female patients aged 18 to 24 years, 25 to 34 years, and 35 to 44 years, the percentage using 5 or more medications was 23%, 34%, and 57%, respectively. In contrast, survey data collected by the Centers for Disease Control and Prevention 13 reported 4.0% of 18- to 44-year old women used 5 or more prescription drugs in the past 30 days, similar to 3% reported (survey data) for prescription drug use in the same age-group by the Slone Epidemiology Center. 14 Similarly, for male patients in our study, the percentage using 5 or medications was 15% for 18- to 24-year-olds, 20% for 25- to 34-year-olds, and 33% for 35- to 44-year-olds. Again, these numbers are much higher than prescription data from the Centers for Disease Control and Prevention (2.1%) 13 and from the Slone Epidemiology Center (4%). 14 Because we did not evaluate the medication lists or health problem lists for each of these age cohorts, it is difficult to speculate about the large difference between our results and that of the other sources. Our patients may use a large number of nonprescription or alternative/complementary products, documented in the electronic medical record, or have a larger number of comorbid conditions requiring prescription medications. Our information regarding medication use was reported directly from patients during clinic visits, including all patients seen during the study time frame, whereas surveys conducted by other means (eg, telephone) may omit patients in specific demographic groups. Another possible explanation for the difference is that our sample is biased toward heavy health care utilizers. Because we limited the population to patients who had an appointment with their primary care provider in the previous 6 months, we may have excluded some healthier patients who did not visit their primary care provider. It is also possible that our electronic medical records may include inaccurate information, such as medications no longer used, thereby inflating the number of medications used. However, a recent electronic medical record medication reconciliation study revealed that comprehensive medication histories taken by pharmacists were likely to reveal greater medication use (primarily nonprescription drugs) than the electronic medical record had listed, suggesting that electronic medical records are more likely to underestimate, rather than overestimate, actual medication use. 15 The fact that our inclusion criteria require patients for whom medications were recently reviewed by clinic staff likely reduced the risk that our medical records contain medications no longer used.
Although our study demonstrates significant use of multiple medications across the age span of patients, it is not known what, if any, types of drug therapy problems are experienced by this younger population. From studies in the elderly, we would anticipate drug therapy problems such as drugs lacking indications, drugs used to treat side effects from other drugs, and drug interactions. 16
This study also sought to examine patient characteristics associated with medication use. Previous population studies evaluating medication use in older populations showed results similar to ours with regard to the association of gender with medication use. 8,11,12,17 -20 Three studies found that rates of medication use were higher in women across all age-groups, except for 65 or 70 years and older. 8,11,12 Two studies found that women older than 65 years used more medications than men in the same age-group. 19,20 However, one recent study of polypharmacy in patients >65 years of age being discharged from a hospital showed no association between gender and polypharmacy. 21 In our study population, females were more likely to have level 2 and level 3 medication use, independent of age.
Most studies have shown that increasing age is associated with increased medication use. 11,17,18 Our study agrees with these findings, as the prevalence of level 2 and level 3 use increased with advanced age. However, our analysis indicates that the oldest (85+ years) age-group had lower odds of level 2 and level 3 use compared with the next oldest group. Although we controlled for major comorbidities in our model, there are other variables we did not include. The higher degree of medication use attributable to these excluded variables is likely captured, in part, by the age variable. This finding may suggest that the oldest patients who lack comorbidities may be healthier than slightly younger age cohorts, and hence less likely to use medications. Some studies, in fact, have found decreasing medication use at the extremes of age. This finding has been attributed to the oldest survivors being the healthiest and requiring fewer medications. 11,22
Previous studies have demonstrated increased medication use with chronic conditions, including diabetes, heart disease, chronic pain, dyslipidemia, and hypertension. 2,8 -10,23 -25 Our study found similar results, demonstrating greater level 2 and level 3 medication use in all conditions listed above. Additionally, our study found that chronic pain was the strongest predictor of use of more than 5 medications among the chronic conditions evaluated. A previous study found that 21% of adult patients using chronic opioid therapy were taking more than 10 concurrent medications, putting them at increased risk for drug interactions. 26
The number of patient encounters with health care providers correlated with both level 2 and level 3 medication use, even when controlling for other confounders. Jörgensen et al 19 reported similar results in their study as patients with greater than 5 office visits were 15 times more likely to have multiple medication use. However, their study population was elderly, defined as 65 years or older, whereas our study population included ages 18 to 85+ years. The wider age range of our study suggests that as contact with medical providers increases, the risk of level 3 medication use increases for all age-groups, not solely elderly patients. Several explanations exist for increased medication use associated with increased health care utilization, including an emphasis on providers to see patients more quickly resulting in prescription of a medication rather than spending time exploring nonpharmacologic treatments and patient education. 27 In addition, direct to consumer advertising has given patients more information to request specific medications from their doctors. 28
Limitations
We acknowledge that there are several limitations related to our methods and analysis. Data were taken from electronic medical records, and over-the-counter medication and complementary/alternative medication use was self-reported. Sensitivity of the regression analysis was limited by the need to impute some demographic information and likely accounts for nonsignificant findings related to BMI, smoking, and marital status. As discussed above, our sample may be biased toward heavy health care utilizers. Although major comorbidities were included in the analysis, there are other indications of health status and drivers of polypharmacy that were not included in the model.
Conclusions
Electronic medical record data has the capacity to provide comprehensive information regarding medication use (prescription and nonprescription). These data can serve as a valuable tool to characterize and evaluate medication use in various demographic groups receiving care in primary care settings. Further investigation of medication use and medication-related problems are warranted in younger patients seen in primary care settings.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies