
Abstract
Bereavement is common among older adults and may result in major depression or complicated grief (CG). Little is known about the effectiveness of physician care for these conditions. We examined whether, among older adults with CG and/or major depression, using physician support was associated with reductions in grief, depression, or anxiety severity. Outcomes were compared to group and religious support. We analyzed data from the Changing Lives of Older Couples (CLOC) Study, a prospective cohort study of married couples in the Detroit area. Spousal death was tracked over 5 years, and follow-up interviews conducted with widowed participants at 6 months (wave 1) and 18 months (wave 2) post loss. Analyses were limited to those with CG or depression with support-seeking data (weighted n = 89). Yes/no items asked whether participants had seen each provider for help with grief up until wave 1. A 19-item grief severity measure was developed by CLOC researchers. The 20-item Center for Epidemiologic Studies Depression scale measured depression severity. The Symptom Checklist 90–Revised assessed anxiety severity. Regressions indicated that seeking support from a family doctor at wave 1 was not associated with changes in anxiety, depression, or grief severity at wave 2 (P > .05). However, support group use was associated with reductions in grief severity (β = −8.46, P < .05), and religious leader support-seeking associated with reductions in depression severity (β = −10.12, P < .01). Findings imply that physician care for grief may not be effective, and support group referral may be helpful. Physicians may benefit from training in recognizing and appropriate referring for bereavement-related distress.
About 2.5 million people die in the United States each year 1 and bereavement (especially spousal loss) is disproportionately experienced by older adults. 2 Most bereaved individuals experience grief that gradually decreases in intensity over time. 3 However, bereavement can also be a major stressor that triggers the onset of physical or mental health problems, including major depression 4 and complicated grief (CG). 5 Though CG is not included as a mental disorder in the current psychiatric Diagnostic and Statistical Manual (DSM-IV-TR), a workgroup has proposed the inclusion of CG as “Persistent Complex Bereavement-Related Disorder” in Section III (conditions requiring further research) of the forthcoming DSM-5. 6 There is substantial evidence that the syndrome of CG exists, 5 and a recent representative population-based survey in Germany found that 60% experienced the death of a significant person and about 7% of these developed CG. 7 Studies have estimated that about 30% of bereaved spouses develop depression in the first months postbereavement, 8 -11 with depression persisting for about 15% at 13 months 8,11 and 25 months. 10
Bereaved older adults often seek help from physicians for emotional distress. 12,13 Yet physicians receive little training in bereavement care, 14 and it is unclear whether they are equipped to be optimally helpful. Bereaved people also commonly seek help from support groups and religious leaders, 12,13 and results of these interventions are similarly unclear. Research on efficacy of support groups is mixed, with some studies showing positive outcomes 14 -17 and others finding no clear effect. 18 -21 No research could be identified on outcomes of bereaved older adults’ support from physicians or religious leaders.
More data are needed to clarify the effectiveness of supports used by bereaved individuals in community settings, as it is these services that most bereaved individuals have access to. We sought to examine bereavement support outcomes in older adults with major depression or CG who participated in a naturalistic longitudinal study. Using secondary analyses from the Changing Lives of Older Couples (CLOC) Study, a representative community sample of older adults, which includes a widowed subset, surveyed longitudinally after their spouse died, this study examines whether utilization of family doctors was associated with reductions in grief, depression, or anxiety among those with CG and/or depression. We also considered how outcomes with family doctor care compared with that of religious leaders and support groups.
Methods
The CLOC Study surveyed 1532 married individuals from the Detroit Standard Metropolitan Statistical Area, using 2-stage area probability sampling. Face-to-face baseline interviews were conducted from June 1987 to April 1988. To be eligible, husbands in all enrolled couples were required to be 65 years or older. A total of 335 respondents lost a spouse during the 5 years of the study, of whom 263 participated in at least one follow-up interview conducted at 6 months (wave 1), 18 months (wave 2), and 48 months (wave 3) after their spouse’s death. As we were interested in outcomes among those with the greatest bereavement-related distress, analyses were limited only to those who had either CG or depression at wave 1 and who also had data available on support seeking (weighted n = 89). High attrition between the 18- and 48-month interviews prevented examination of outcomes at 48 months. The Columbia University Morningside Institutional Review Board reviewed these proposed analysis and concluded that they were exempt from further review.
Measures
The CLOC data were collected prior to the recognition of CG as a clinical entity. Therefore, to identify a CG-positive subsample, we selected items on the CLOC questionnaire that roughly corresponded to our proposed CG criteria set. 5 The identification of the CG-positive group is described elsewhere (A. Ghesquiere, N. Duan, and M. K. Shear, “Prevalence and correlates of Complicated Grief in the Changing Lives of Older Couples (CLOC) Study,” unpublished data). The CLOC data set already contained a variable for whether depression was present or absent at each wave, based on items assessing DSM-III criteria.
Outcome measures were symptom severity for grief, depression, and anxiety 18 months after the loss. A continuous grief severity measure was developed by CLOC researchers and described elsewhere (α = .88). 22 In its structure and much of its content, this measure resembles the Inventory of Complicated Grief, often used to assess CG. 23 Depression severity was measured using a subset of 9 items from the 20-item Center for Epidemiologic Studies–Depression (CES-D) scale (α = .75). 24 Anxiety severity was assessed using the anxiety subscale of the Symptom Checklist 90–Revised (α = .86). 25,26
The independent variables were family doctor, support group, and religious leader bereavement support seeking. Three yes/no items asked whether participants had seen each of these provider types for help with feelings of grief, loneliness, or missing their spouse. This item captured any use between the death and the wave 1 interview.
We controlled for variables found in previous analyses to be associated with grief, depression, or anxiety outcomes postloss. 27,28 Control variables included race, gender, education, income (because income distribution was skewed, the natural log of income was used), and single items on religious participation and importance of religious beliefs. Additionally, as there is reason to expect that social network characteristics can influence help seeking, 29 -31 we estimated and controlled for several social network variables (a single close network size item, positive emotional support from friends and relatives (2 items; α = .71), positive emotional support from children (2 items; α = .70), and instrumental support (3 items; α = .64)). Anxious attachment style 32,33 has been associated with increased likelihood of mental health support seeking 34 ; an attachment anxiety composite made up of 4 items was included (α = .80). Finally, we controlled for wave 1 (6 months postloss) anxiety, depression, and grief severity.
Statistical Analyses
All analyses were conducted using Stata statistical software, version 12. Descriptive analyses examined the range and central tendency of all variables. Independent-samples t tests compared the average change in depression severity, anxiety severity, and grief severity between waves by each type of support sought. Separate multiple regression analyses were conducted using the svy regress procedure in Stata. Because many participants reported using more than one service, regression analyses controlled for the effects of each service type.
Results
Eighty-nine of the 263 widowed CLOC participants (35.0%) met criteria for depression and/or CG at wave 1 and also had data on wave 1 service use. Of this group, 65 participants completed interviews at wave 2. Table 1 provides demographic data on this distressed sample and descriptive statistics for all independent, control, and confounding variables. The majority of the sample was female (73.0%) and white (84.7%), with an average age of 69.9 years. Of the 89 participants, 77 met our criteria for CG at wave 1, of whom 27 had co-occurring depression, and 12 met criteria for depression without CG. At wave 2, 22 met criteria for CG, of whom 5 had co-occurring depression and 9 had depression without CG. A sizable minority (40.4%) of symptomatic participants with CG and/or depression did not seek support for their grief from any source. Of those who sought support (n = 53), 76% (n = 40) did so from family doctors, whereas 45% turned to religious leaders and 25% to support groups.
Changing Lives of Older Couples Study Widowed Sample Descriptives (Weighted N = 89).

Seven sought religious leader support alone and 17 sought religious leader support in combination with support group and/or family doctor support.
Five sought support group support alone and 8 sought support group support in combination with religious leader and/or family doctor support.
Twenty-one sought family doctor support alone and 19 sought family doctor support in combination with religious leader and/or support group support.
Table 2 shows mean wave 1 and wave 2 scores, and mean change, for depression severity, anxiety severity, and grief severity by each type of support, compared to those who sought no support. There were no significant differences among physicians, religious leaders, or support groups in any of these outcome measures, except that those who used groups had a reduction in grief severity about 3 times greater than those who did not seek any support. Though this difference did not reach statistical significance, it was also more than twice the magnitude of the change seen with physician care.
Change in Anxiety, Depression, and Grief Severity From Wave 1 (6 Months) to Wave 2 (18 Months) Postbereavement: Comparison by Support Sought up to Wave 1.

Compared with those who did not seek any support for grief.
P < .05.
There were some differences found in independent- samples t tests and χ2 tests across control variables between those sought each kinds of support and those who did not seek any support. Those with high religious participation were marginally significantly more likely to seek support from religious leaders (χ2 = 4.666, P = .031) and were also significantly more likely to go to family doctors (χ2 = 4.840, P = .028). Moreover, non-whites were significantly more likely to seek support from religious leaders (χ2 = 6.267, P = .012). There was also a difference in use of support groups across education levels, with use more likely among those with a high school education or greater (χ2 = 4.770, P = .029). Women were significantly more likely to go to religious leaders (χ2 = 4.105, P = .043) and marginally more likely to go to support groups (χ2 = 3.780; P = .052). Likelihood of attending support groups decreased marginally significantly with age (t = 1.902, P = .63). There were no significant differences in any other control variables. We controlled for all variables that showed significant differences in regression analyses.
Weighted least squares regressions, which included all control variables, indicated that seeking support from a family doctor at wave 1 was not associated with changes in anxiety, depression, or grief severity at wave 2. However, using a support group at wave 1 was associated with reductions in grief severity, and support seeking from a religious leader at wave 1 was associated with reductions in depression severity. The effect of using any other support type was controlled for in the analyses. None of the support types were associated with changes in anxiety severity. A sizable proportion of variance was explained by the models, with R 2 values of .52 for grief as the outcome, .47 for anxiety, and .53 for depression (Table 3).
Weighted Least Squares Regressions Predicting the Effect of Bereavement Service Use Reported at 6 Month Follow-up on Depressive, Anxiety, and Grief Symptoms at 18-Month Follow-Up.
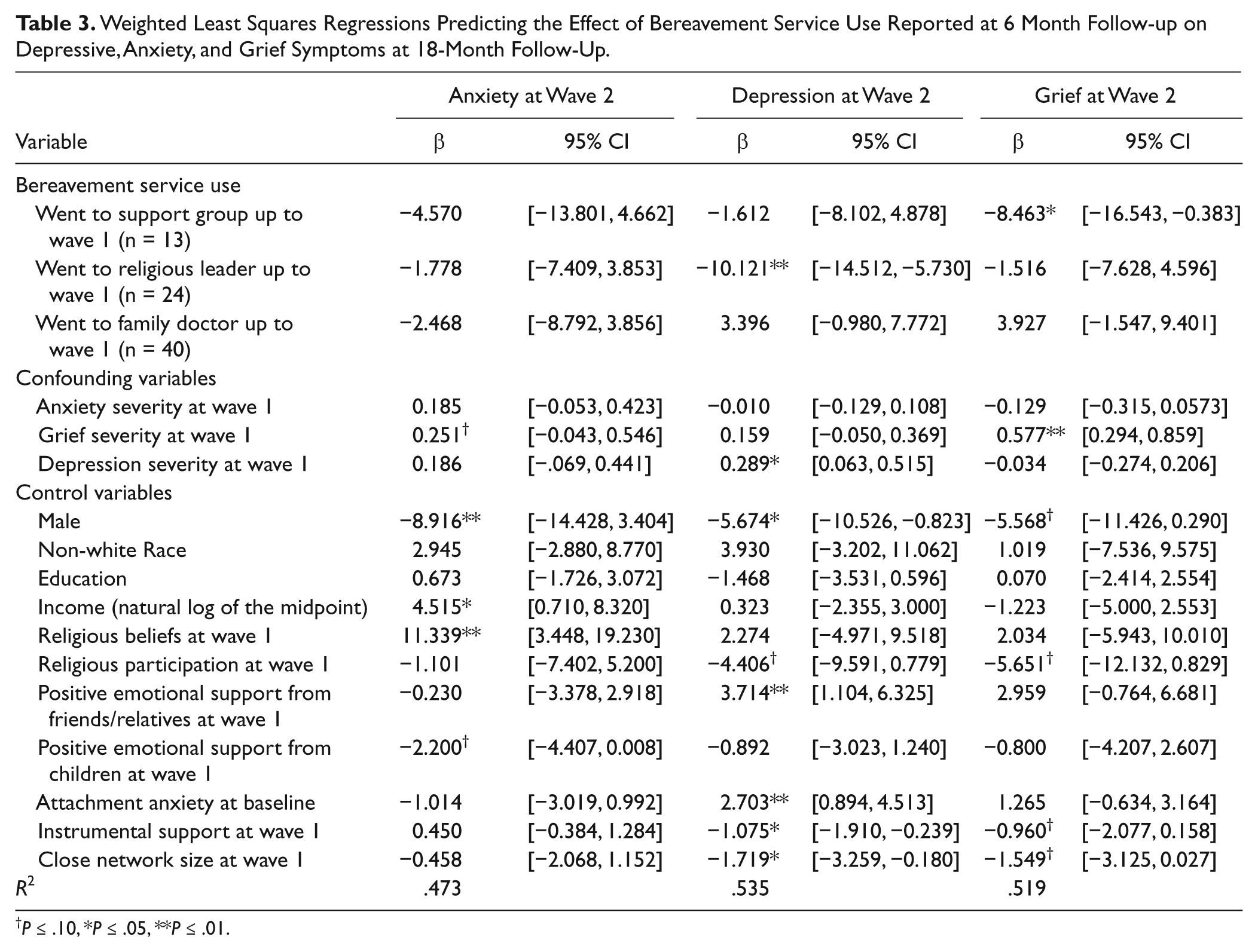
P ≤ .10, *P ≤ .05, **P ≤ .01.
Discussion
Only about 60% of this distressed sample of widowed older adults reported using any of the 3 common grief supports within 6 months of their loss, suggesting that there may be a gap between the need for services and their use. Results also suggest that older adults seeking bereavement support from their physicians may not get the help they need, and that grief-specific services may be a more effective option. Seeking help from religious leaders also failed to be associated with reduction in grief but was significantly related to the course of postloss depression. Moreover, none of the service types impacted anxiety. Research shows that anxiety in older adults responds best to specialized treatment, including cognitive–behavioral therapy and pharmacotherapy, which is usually delivered by mental health professionals. 35 Such care was likely beyond the expertise of family doctors, religious leaders, or support groups.
Past research on the efficacy of support groups is mixed, with some studies finding positive outcomes 14 and others not. 20,21 Variations in sample and intervention technique may account for these differences. However, when effective, support groups are thought to operate by providing emotional and social support, and may help fill gaps in the bereaved person’s existing social network. 36 In the current study, self-help and support groups were the only service use type that is specifically focused on grief, whereas family doctors and religious leaders would primarily be seen for medical care and general spiritual support, respectively. Though data on the content of support groups are unavailable in this study, it is possible that the emphasis of support groups on grief made them effective. The fact that support groups did not also reduce depression is unsurprising, as support groups are unlikely to provide treatment specific to depression.
The finding that religious leaders reduced depression severity, whereas support groups and family doctors did not, is novel. To our knowledge, no published research has examined the impact of religious leader support on depression postbereavement. Theory offers some possible explanation for this finding. Neimeyer 37 has proposed that that successful coping after a death requires finding a sense of meaning in the loss and has argued for developing clinical interventions to enhance a sense of meaning. Religious beliefs inherently create systems of meaning. 38 Consultation with religious leaders might therefore enhance a sense of meaning and reduce symptoms. Another possibility is that religious help may be implicitly tailored to one’s needs. Presumably bereaved individuals seek help from a religious leader they know, who shares a religious denomination and perhaps views about death, the afterlife, and so on. Therefore, religious support could be particularly appropriate help for some. Possible active ingredients of bereavement support from both religious leaders and support group might be investigated and, if possible, operationalized and tested in randomized controlled trials. Importantly, although longitudinal data suggest that there may be a causal effect, the lack of systematic information about how much and what kind of help was provided makes it difficult to draw firm conclusions.
Although we do not have data on what family doctors in this sample actually did with widowed participants, or what exactly participants asked them to do, it is unlikely that participants were receiving evidence-based treatment for grief, depression, or anxiety from their family doctors. Other studies have found that the quality of mental health care in the primary care sector is lower than in the specialty mental health sector. 39,40 Unfortunately, the CLOC study did not gather data on family doctors’ detection of depression, CG, or anxiety, or on how many family doctors prescribed medication. It is also possible that those who sought help from family doctors were more ill than those who attended support groups or sought out religious leaders for their grief. However, mean scores on the symptom rating scales at 6 months postloss were not significantly greater for those who sought out physicians compared to those who sought no support. Although no data are available on grief support in primary care, studies have shown that primary care physicians often do not detect depression or anxiety in older adults, 41,42 that the quality of depression care provided in the primary care sector is lower than in the specialty mental health sector, 39,40 and that primary care physicians may not effectively treat anxiety. 43
The finding that religious leader support reduced depression severity, whereas support groups reduced grief severity, also supports the observation that these conditions respond to care differently. Indeed, previous studies have found that CG and depression have distinct symptoms 44,45 and each require unique treatments. 46 -48 Our results provide additional evidence for the distinctiveness of CG and depression. Our results should be considered preliminary for a number of reasons. First, the sample size is small; it is possible that there was not sufficient power to detect meaningful changes in some symptoms. It is also possible that unmeasured confounders, such as talking with friends, may have affected outcomes. In addition, the use of bereavement services was assessed only via participant self-report and there is no information on the content, duration, frequency, or timing or services received. Participants who sought help once are grouped with those who did so repeatedly over the first 6 months of bereavement. Nor do we have data on patient adherence to any treatments provided. It is possible, for example, that some family doctors appropriately prescribed antidepressants to participants, but the participants did not take them regularly. In general, older adults are less likely than younger adults to complete 30- or 60-day courses of antidepressants at a therapeutic dose. 49 We were also unable to examine whether doctors had any preventative effect on the evolution of normal acute grief into complicated grief, as we did not have data on physician support for grief symptoms immediately after widowhood. Future studies could explore whether physician support might prevent CG. Moreover, suicidality is common among older adults with both depression and CG. 50,51 We did not examine suicidal ideation as a separate outcome because only 6 participants endorsed items on suicidality at wave 2. And though the algorithms for identifying CG and depression included items on suicidal ideation, we did not have data on physicians’ detection or treatment of suicidality. Future research should also examine the physicians’ role in detecting and addressing suicidal ideation in bereaved older adults. Also, though a CG-positive group was identified in the CLOC sample, this measure was created by the authors and was not a component of the initial study design. Finally, bereavement is restricted to spousal loss, and data were collected in one area of the United States starting in the 1980s. Therefore, results may not generalize to other types of loss or to other regions of the country, or to the present day. Antidepressants are much more widely prescribed to older adults now than they were in the 1980s, for example. 48,52 Finally, as analyses lack both a control group and random or matched assignment to treatment conditions, causal inference is limited. Findings should be replicated.
Despite these limitations, our results have potentially useful implications. The study provides evidence that older adults are likely to seek bereavement support from family doctors and that they may not receive the help they need. Primary care physicians may benefit from training on how to recognize grief symptoms and provide effective support for subgroups of highly distressed bereaved people, including referrals to grief support groups. Recently, researchers have begun integrating specialty care for depression into primary care clinics 53 ; these efforts could be expanded to reach bereaved older adults with CG.
Footnotes
Acknowledgements
We acknowledge the original Changing Lives of Older Couples (CLOC) Study research team, which conducted the surveys that are analyzed in this report.
Authors’ Note
The Hartford Doctoral Fellows Program in Geriatric Social Work had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; and preparation, review, or approval of the article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The CLOC study was funded by the National Institute on Aging. These secondary data analyses were supported by the Hartford Doctoral Fellows Program in Geriatric Social Work.
Author Biographies