
Abstract
Since the mid-1980s, the prevalence of obesity among adults in the United States has more than doubled.1,2 Obesity is now implicated in approximately 15% of deaths, making it the second leading actual cause of mortality in the United States after tobacco. 3
A landmark 2007 study found that social networks may play an important role in obesity. 4 Using 31 years of data from the Framingham Heart Study, Christakis and Fowler 4 found that an individual’s likelihood of becoming obese was highly influenced by whether or not someone in their social network became obese. The impact was stronger when a closer friend or a friend of the same sex became obese. The authors argue that if social networks could contribute to the obesity epidemic, networks should also be able to be used to spread positive health behaviors and curb the obesity epidemic.
Research on the health and behavioral impacts of social networks was published just as online social networks (OSNs) exploded in popularity. OSNs allow people to construct an online profile within a bounded system, connect with or “friend” other users, communicate via the website with other members, post announcements to one’s network or all viewers, and view information about their network. 5 The technology also enables uploads of data from devices such as accelerometers and scales. In 2011, a Pew Internet survey reported that 65% of US adults who are online (78% of all adults are online) use OSNs like Facebook or Twitter, up from 16% in 2006.6,7 There have been calls for public health interventions to take advantage of OSNs to influence behavior through support, information transfer, social influence, modeling, and transmission of social norms.8,9
Research into the public health uses of OSNs is just starting to be published and is still primarily descriptive. Studies have demonstrated that an existing smoking cessation OSN has the characteristics required for sustainability of social support and social influence, and that using Facebook for a wellness intervention is possible but requires allowing users to limit which members of their network can view their participation.10-12 Studies are only beginning to examine the impacts of social networks and few have yet taken advantage of the abundance of data collected by OSNs. A recent study by Graham et al 13 found no additional benefit of OSN compared to an online smoking cessation program.
This study is a randomized trial of a health-oriented OSN, iWell. 14 The iWell OSN combined an online platform for social networking with an accelerometer and a weight scale that both wirelessly uploaded data for tracking over time. The goal of this study was to examine whether the intervention group had greater increases in physical activity, weight loss, and improvements in clinical indicators over 6 months compared with those in the control group, who did not use the iWell OSN. Furthermore, the study examined the extent to which use of the social network was associated with weight loss and physical activity among those in the intervention group.
Methods
This 6-month randomized trial of the iWell OSN was conducted in 2010-2011. Following enrollment, participants were randomly assigned to the intervention or control group and followed over 6 months. Participation included providing laboratory samples at baseline, 3 months, and 6 months (at no cost to the participant). The study was approved by the Human Subjects’ Committees of PeaceHealth and the University of Oregon and was registered on http://clinicaltrials.gov in October 2010.
All participants received printed lifestyle guidelines on diet and exercise during their first study visit. These materials included a sample daily meal plan with recommended serving sizes, a handout about recommended daily levels of exercise, and a number of articles about the benefits of exercise and healthy eating.15-17
Intervention participants were provided access to the iWell OSN and were given an accelerometer that allowed them to capture their physical activity or “steps” for upload to the iWell OSN and a wireless weight scale for uploading weight data. With the iWell OSN, participants could connect (“friend”) others in the network, send individual messages to their friends, make public postings, view their contact’s postings, view their physical activity or “steps,” view their weight, and compete against others in the network on the number of “steps” walked or run. The iWell OSN also allowed participants to set individual health-related goals and to receive motivational messages.
Study Sample
Participants were recruited from PeaceHealth Oregon employees and their family. Participants were between 18 and 79 years old, had stable medication for 3 months, and had expressed concern about their weight or health in an online screener survey. People with prior bariatric surgery, 20 or more pounds of weight loss in the prior 3 months, or serious health issues (eg, recent cardiovascular event, cancer, or bipolar disorder) were excluded. All participants were compensated with a cookbook at their 3-month follow-up and a $25 Amazon.com gift card at the 6-month follow-up.
At baseline, 513 people enrolled in the study. A total of 349 people, or 68%, participated for the full 6 months and are included in the analysis. Equal percentages of intervention and control group participants dropped out of the study (32%). Those who stopped participating were not significantly different from those who continued in terms of baseline physical activity levels, clinical indicators, or gender. They did, on average, have higher baseline body mass index than those who participated for the full 6 months (33 vs 31 kg/m2) and they were younger.
Independent Variables
The main independent variable was whether or not the participant was randomized to the intervention or control group. For the supplementary analyses among the intervention group—which examined how use of the iWell OSN was related with weight loss and physical activity—the number of number of messages participants sent to individuals in the iWell OSN and the number of uploads of accelerometer data were examined.
Dependent Variables
Dependent measures included study participants’ physical activity, weight, cholesterol, and triglycerides. Weight, cholesterol, and triglycerides were measured by staff at the PeaceHealth Laboratory.
A comprehensive, validated self-report measure called the Short Questionnaire to Assess Health-Enhancing Physical Activity (SQUASH) was used to measure physical activity. 18 Respondents completed the SQUASH online, separate from the laboratory data collection, and unfortunately 25% of participants failed to complete the SQUASH surveys.
Analytic Approach
Initially, the intervention and control groups’ demographic characteristics and baseline dependent variables were compared to assess the similarity of the 2 groups.
To test the impact of the intervention, the dependent variables were examined at baseline, at 3 months, and at 6 months. Independent sample t tests were used to assess whether there was greater change for the intervention group compared with the control group. The principal analysis included the sample of 349 study participants, who participated in the study for the full 6 months. Supplementary intention-to-treat analyses were consistent with what is presented in the primary analyses and are available on request from the authors.
Regression models were developed to examine the relationship between use of the iWell OSN and accelerometer, and increases in leisure time walking and weight loss over the study period among the intervention participants. Two independent variables were used. One measure of OSN use was selected because of the high correlation between potential measures, which would result in problems with multicollinearity. The number of private messages participants sent to others in the iWell OSN (as recorded by the OSN) was selected because it exhibited a strong relationship with change in physical activity and weight change in bivariate analyses. The second measure was the number of uploads of accelerometer data. Control variables in the regression models included gender, age-group, and whether or not the participant had a body mass index ≥30 kg/m2 at baseline.
Results
Table 1 shows the characteristics of the study sample, who were overwhelmingly female (79%), non-Hispanic white (93%), and 50 years or older (60%). There were no statistically significant baseline differences between the intervention and control groups in terms of demographics or physical activity, weight, or clinical indicators.
Description of Study Sample. a

No differences between intervention and control groups were statistically significant.
Table 2 shows that the intervention group significantly increased weekly leisure walking from 129 to 341 minutes, on average, a 164% increase over the 6-month study period, compared with a 47% increase for the control group. The intervention group had larger increases in 9 other areas of physical activity compared to the control group; however, none of those differences were statistically significant (see the appendix).
Average Values of Clinical and Physical Activity Indicators Over the Study Period, for Intervention and Control Participants. a

Sample sizes for weight and clinical indicators: intervention (n = 180) and control (n = 169). Sample sizes for physical activity and walking: intervention (n = 137) and control (n = 125). Change from baseline was significantly different for intervention and control groups at P < .05.
Change from baseline was significantly different for intervention and control groups at P < .01.
The intervention group also lost more weight over the 6-month study period than did the control group (mean 5.2 vs 1.6 pounds). There were, however, no significant differences between the intervention and control groups in terms of change in low-density lipoprotein and high-density lipoprotein values. Although the intervention group had a significant reduction in triglycerides at 3 months compared with the control group, it was not sustained at 6 months.
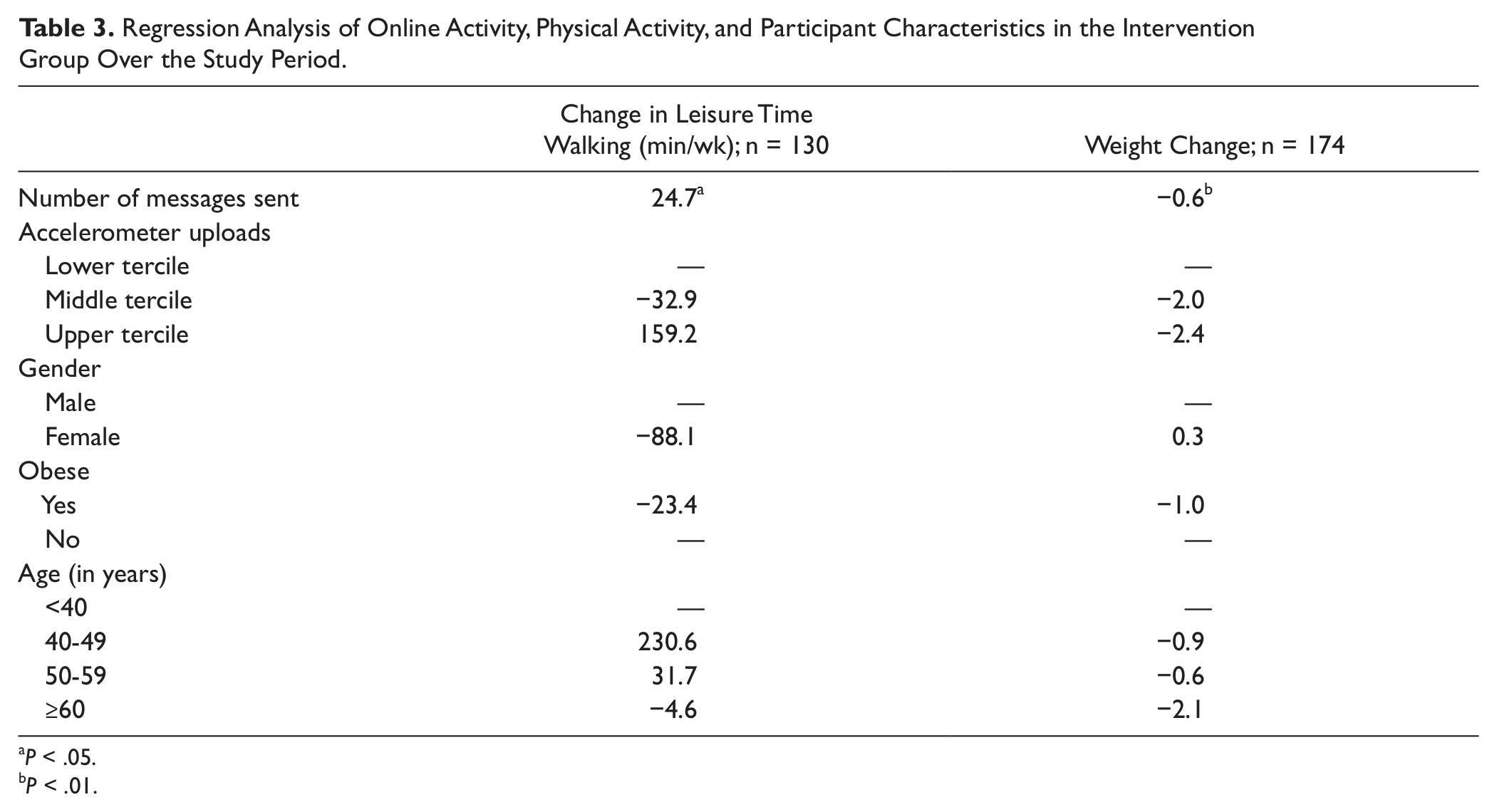
In multivariate regressions, the number of messages sent by participants was positively related to increases in leisure time walking minutes and it was negatively related to weight change (Table 3). In other words, the more messages a participant sent on the iWell OSN, the more likely he or she increased the number of minutes walked, and reduced his or her weight. None of the factors—the number of accelerometer uploads, obesity, age, or gender—was related to change in leisure time walking or weight.
Regression Analysis of Online Activity, Physical Activity, and Participant Characteristics in the Intervention Group Over the Study Period.
P < .05.
P < .01.
Discussion
This study found that people randomized to a health-oriented online social network with an accelerometer and wireless scale increased the amount of leisure-time walking from approximately 6.5 miles a week to 17.1 miles a week over 6 months. This was a significantly greater increase than that observed within the control group, which increased walking from approximately 7.1 miles weekly to 10.4 miles. Furthermore, those randomized to the iWell OSN shed 3 times as many pounds as the control group (5.2 vs 1.6). The intervention, however, neither significantly improved vigorous physical activity, such as running or high-intensity housework, nor did it improve their triglycerides or cholesterol levels relative to the control group.
Intervention participants who used the iWell OSN more, specifically sending more private messages, increased the amount of time spent walking and lost more weight than participants who used the OSN less. These findings suggest a dose–response relationship, in which greater use of the iWell OSN was associated with more minutes walking and greater weight loss. OSNs may be an important way to support people in following through on their desires to increase physical activity and become healthier.
Given the study design, the findings are generalizable only to those who want to improve their health, which was a requirement for study participation. The findings are also generalizable only to similar OSNs with wireless devices that enable uploading of physical activity and weight data. Future studies may want to examine the impact of the OSN separately from the wireless devices. Additionally, future work should include more diverse study participants.
Other study limitations include the use of a self-report measure of physical activity, which was used because the control group did not have accelerometers and also because accelerometers might have affected measurement of baseline physical activity. The SQUASH, however, is a reliable measure, and in this sample, increases in reported walking were positively correlated with weight loss. Another limitation was the relatively high attrition rate, though our intention-to-treat analysis resulted in substantively similar findings. Future work should examine the extent to which OSNs can promote long-term behavior change and sustained weight loss. Research is also needed to examine whether OSNs can promote diet change in addition to increased physical activity. This may result in more evident changes in cholesterol and triglyceride levels, which may be observed relatively quickly in dietary interventions. 19
In summary, this study provides promising evidence that OSN participation when paired with monitoring tools can promote greater levels of physical activity and weight loss. The development of strong, OSNs may be a relatively low-cost and scalable way to positively influence health-related behavior.
Footnotes
Appendix
Frequency of Physical Activity (SQUASH) Over the Study Period for Intervention and Control Groups. a
| Baseline (min/wk) | 3 Months (min/wk) | 6 Months (min/wk) | |
|---|---|---|---|
| All physical activity | |||
| Intervention | 2055.9 | 2479.3 | 2686.9 |
| Control | 1950.5 | 2102.4 | 2248.2 |
| Commuting | |||
| Walking | |||
| Intervention | 2.4 | 3.3 | 3.1 |
| Control | 0.0 | 1.6 | 6.2 |
| Cycling | |||
| Intervention | 3.9 | 4.3 | 7.0 |
| Control | 4.2 | 4.8 | 6.7 |
| Activities at work | |||
| Light | |||
| Intervention | 1260.9 | 1362.9 | 1392.7 |
| Control | 1180.1 | 1242.0 | 1235.5 |
| Intense | |||
| Intervention | 146.3 | 193.5 | 248.1 |
| Control | 150.0 | 143.4 | 160.0 |
| Household activities | |||
| Light | |||
| Intervention | 306.2 | 285.9 | 309.7 |
| Control | 231.6 | 310.4 | 319.7 |
| Intense | |||
| Intervention | 60.9 | 63.1 | 85.1 |
| Control | 65.1 | 67.3 | 69.8 |
| Leisure time | |||
| Walking | |||
| Intervention | 129.2 | 354.1 b | 341.0 b |
| Control | 141.7 | 160.4 | 208.6 |
| Cycling | |||
| Intervention | 7.1 | 9.6 | 17.5 |
| Control | 9.8 | 10.2 | 13.9 |
| Gardening | |||
| Intervention | 25.8 | 26.4 | 94.6 |
| Control | 25.1 | 25.0 | 73.2 |
| Odd jobs | |||
| Intervention | 40.2 | 73.6 | 88.1 |
| Control | 52.1 | 46.8 | 67.0 |
| Sports | |||
| Intervention | 73.0 | 83.8 | 99.9 |
| Control | 90.8 | 90.5 | 87.5 |

Abbreviation: SQUASH, Short Questionnaire to Assess Health-Enhancing Physical Activity.
Sample sizes: intervention (n = 137) and control: (n = 125). Change from baseline was significantly different for intervention and control groups at P < .05.
Change was significantly different at P < .01.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article:
Financial support for conducting the clinical trial was provided by SK Telecom Americas.