
Abstract
Introduction
In general, older adults are safe drivers, 1 but crash and fatality rates rise with age, as medications and conditions common in old age can affect driving ability. 1 Driving reduction or cessation decisions are difficult because of the sense of personal independence linked to driving,2,3 transportation considerations, and the negative health and emotional consequences associated with driving cessation.4,5
Various guides exist to help physicians 6 and family members or friends7-9 talk with older drivers; prior work suggests that older drivers are open to these conversations10,11 and believe that physicians and family members should help make driving decisions.3,12 Recommendations from personal physicians and family members are 2 of the most common reasons for driving cessation by older adults, 13 but many physicians are uncomfortable with these conversations. 14
“Advance driving directives” (ADDs) 10 may facilitate these difficult discussions, especially if used by physicians well before there are specific driving concerns. Similar to advance directives for end-of-life care, ADDs allow a driver to identify a person to help them decide about driving cessation. An ADD would not be legally binding; rather, its intent is to facilitate discussions and decisions about driving in the future.
Our preliminary work in a sample of outpatients suggested that older adults might support ADDs. 10 We conducted this study in a community setting to examine further the perspectives of older drivers concerning ADDs and to identify variables associated with willingness to complete an ADD.
Methods
We conducted an anonymous, voluntary survey of local older drivers at 2 independent living facilities and 2 senior community centers; adults 55 years or older who self-identified as current drivers were eligible. We recruited participants on a single day in group settings (living facilities) and from those passing through a common area (community centers, where surveys were also available at the front desk). Participants self-completed the 24-item surveys on paper and did not receive compensation. Completed surveys were entered into Research Electronic Data Capture for data management. 15 The institutional review board deemed this project exempt from review.
Survey questions from existing questionnaires16-18 and those newly created were pilot-tested in a convenience sample of 10 community-dwelling older adults at an outpatient clinic for clarity and content (see the appendix). Driving variables included the following: driving frequency, ability, and stressfulness; motor vehicle crashes and police stops as a driver in the past 12 months; driving avoidance under certain conditions; and whether, in the past 12 months, someone had spoken with the participant about driving safety, restricted the participant from driving with passengers, or recommended driving cessation.
We assessed opinions about mandatory age-based testing with the statement: “Above a certain age, drivers should be required to have a driver’s test before they can renew their license.” Those who “agreed” or “strongly agreed” were asked the age at which testing should be required. Participants were asked to identify who should determine license revocation when a driver is no longer safe, with multiple responses allowed (driver, family member, physician, state driver’s license office, police or court system, other). We asked whether participants had talked with someone about their wishes if their driving skills decline; if they responded “yes,” we asked “with whom?” We also asked the following: whose advice the driver would follow concerning driving; who the driver would want to “take away the keys” if unable to drive safely; and what kind of driver testing the driver would want. Finally, we asked drivers if they would complete an ADD if recommended by a doctor, friend or family member; for those who responded yes, we asked the likelihood of following the directive in the future.
We described participants’ responses using medians and interquartile ranges (IQRs) or proportions and 95% confidence intervals (95% CIs). We used logistic regression (and calculated odds ratios [OR] with 95% CIs) to test for associations between the driver opinion of greatest interest (willingness to complete an ADD) and driver characteristics; we decided a priori to adjust each regression for age and gender.
Results
Of 173 surveys collected, participant ages were missing on 5 (3%), and these surveys were excluded from further analysis. Of the 168 included, the median age was 76.5 years (range = 56-93 years) and 79% were female. Most participants drove everyday or almost every day (74%) and described their overall driving ability as “good” (72%). Almost a third (29%) described driving as very or somewhat stressful and 86% reported restricting their driving in at least one adverse condition, and 7% reported a crash as a driver in the past 12 months. Very few said that, during the past 12 months, someone had restricted them from driving with passengers, recommended driving cessation, or talked about driving safety (Table 1).
Participant Characteristics, Opinions, and Experiences (N = 168)

Multiple responses allowed; numbers may not add to 100% total because of rounding or missing data (not reported if <5% of total).
Almost three fourths “agreed” or “strongly agreed” that drivers above a certain age should be required to have a driving test before license renewal; the median recommended age was 80 years (IQR = 75-80). Despite their support for age-based testing, fewer drivers felt that the driver’s licensing bureau (32%) or police or court system (26%) should determine license revocation for an unsafe driver, preferring to leave this decision to the driver (71%), a family member (61%) or a physician (59%).
Only 21% of drivers said they had talked with someone about their wishes if their driving skills should decline, more commonly with an adult child (56%), spouse or partner (31%), or friend (28%) than with a primary care physician (11%). However, approximately two thirds of drivers said that if a physician, family member, or friend spoke with them about making a plan for when their driving abilities decline, they would “be open to talking about it” or would “listen to suggestions” by a physician (Figure 1). Small numbers of subjects said they would “be worried about losing my license” or would “be offended, insulted or angry” (Table 1).
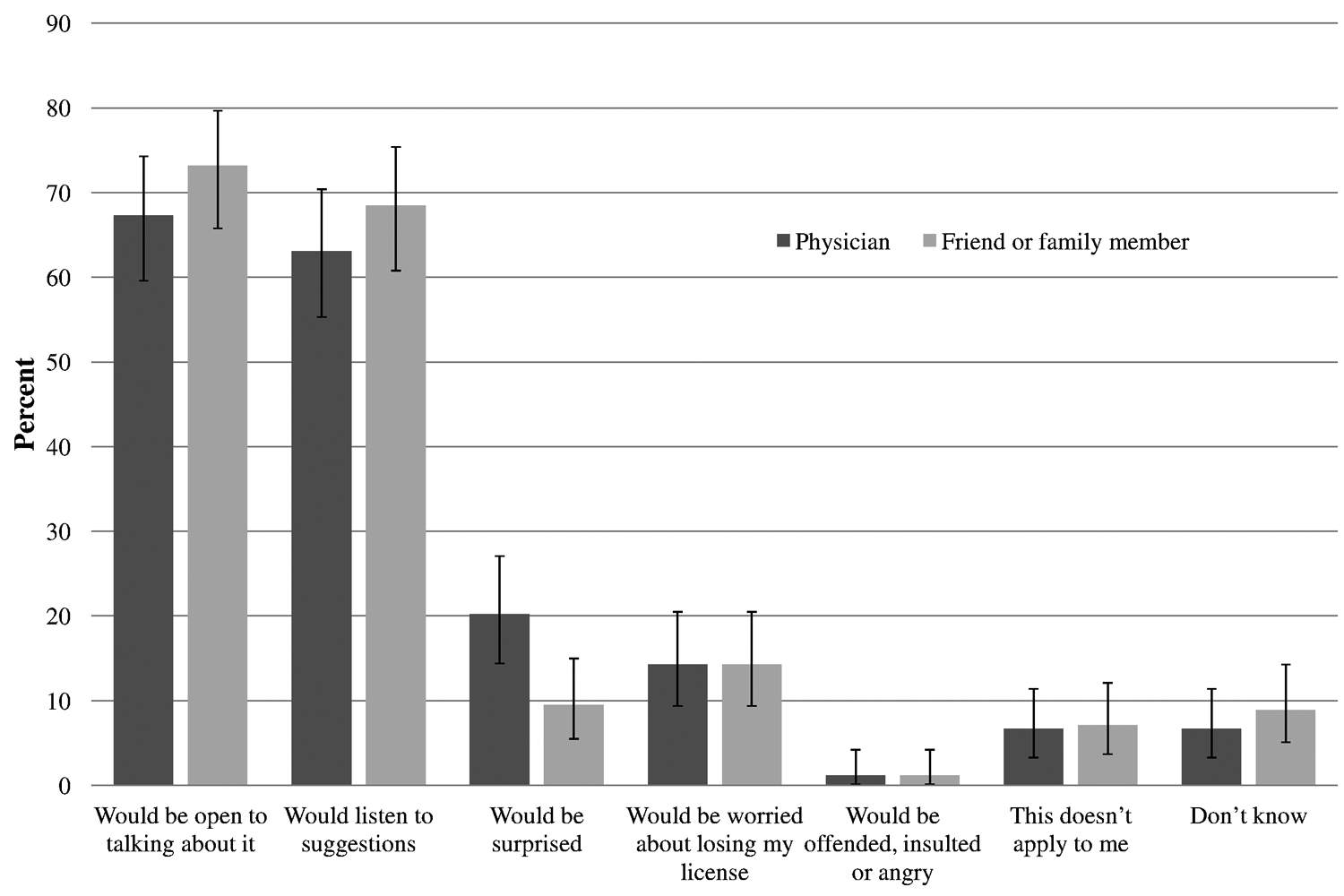
Likely response if a doctor or family member/friend talked with you about setting a plan for when your driving abilities decline in the future (N = 168)
When asked about ADDs, 86% of drivers said they “would” or “maybe would” complete an ADD if recommended by a doctor, friend or family member. Of the drivers who said they “would” complete an ADD, 79% said they were “likely” or “very likely” to follow the ADD in the future. In bivariate analysis, the only factors significantly associated with willingness to complete an ADD if recommended were agreeing or strongly agreeing with age-based driver retesting (OR = 2.21, 95% CI = 1.05-4.68) and being open to talking about a future driving plan if brought up by a physician (OR = 2.10, 95% CI = 1.09-4.05) or by a friend or family member (OR = 2.49, 95% CI = 1.23-5.02; Table 2). These estimates did not change significantly when adjusted for gender and age.
Bivariate and Multivariate Logistic Regression Analysis of Factors Associated With Willingness to complete an “Advanced Driving Directive” if Recommended by a Doctor, Friend, or Family Member (N = 168)

Abbreviations: 95% CI, 95% confidence interval; MVC, motor vehicle crash.
Separate analyses, each adjusted for age and gender.
Multiple responses allowed per participant; “—” indicates no observations.
Discussion
In this sample of community-dwelling older drivers, most were open to driving conversations with physicians and would consider filling out an ADD if recommended. Consistent with our prior work, 10 most drivers supported retesting above a certain age but felt drivers, family members, or physicians, rather than licensing bureaus or other state authorities, should make decisions about license revocation. These results support both the physician’s traditional role in counseling older drivers and also the newer idea of ADDs to facilitate driving conversations at the time of completion and in the future.
Older drivers, family members, and legal authorities expect physicians to take a leading and active role in discussions and decisions about safe driving,6,19,20 and prior work suggests that physicians accept this role.21,22 However, physicians may be reluctant to have these conversations with individual patients 23 because of issues such as fear of damaging the physician–patient relationship,20,24 inadequate training, 24 time constraints,19,25 and uncertainty about their ability to assess a driver’s ability. 26 We found that most older drivers would be open to discussing future driving plans and would listen to physician recommendations, and very few said they would be offended, insulted, or angry if a physician brought up the topic of planning for what to do in the case of decreased driving ability.
Given that most drivers will eventually experience some decline in driving abilities, early and regular conversations about driving may make the topic an easier one for drivers, physicians, family members and friends. An ADD could facilitate conversations about future driving decisions and in the future serve as a guide for decision making. Available templates refer only to family involvement,27,28 but modifications could make the forms more usable by physicians and friends. Although in this cross-sectional survey we cannot know how a completed ADD would actually affect future driver behavior, these findings provide support for physicians to begin these conversations with patients. Some patients may not be interested, but for those who are, an ADD might be very useful. Although prior work has shown some differences by gender in driving cessation,4,29 in this small sample we did not find significant differences between men and women; future studies could help identify characteristics of drivers most likely to be influenced by an ADD.
Limitations include our use of a convenience sample from 4 sites, so results may not generalize to other populations. Selection bias may be an issue, since because participants recruited before a free “driving safety seminar” at one facility (hosted by the facility but with external presenters) may have been more open to driving discussions. The survey relied on self-report, and the relatively small sample size limited subgroup analysis.
In conclusion, many older drivers may be open to conversations with their physicians, family members, and friends to make plans for future driving decisions. The findings of this preliminary suggest that ADDs could be a useful way to open these discussions and support the need for future development and testing of ADDs.
Footnotes
Appendix
Acknowledgements
The authors thank Ruth Johnson, Morgan Valley, and Kristen Carpenter for their assistance with patient enrollment.
Authors’ Note
The contents of this article are solely the responsibility of the authors and do not necessarily represent the official views of the Emergency Medicine Foundation or the John A. Hartford University of Colorado Denver Center of Excellence. No sponsor had any direct involvement in study design, methods, subject recruitment, data collection, analysis, or manuscript preparation.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Emergency Medicine Foundation (2009-2011 Research Fellowship) and the John A. Hartford University of Colorado Denver Center of Excellence.