
Abstract
Introduction
The all-terrain vehicle (ATV) was introduced in America in the 1970s and has gained in popularity with an estimated 5.6 million ATVs in the United States and 2364 million driving hours in 2001. 1 ATVs are designed with large, low-pressure tires to be used on rugged, irregular terrain. The rider straddles atop the engine using a handlebar configuration to steer a vehicle with most engine sizes greater than 400 cm3, vehicle weights up to 600 pounds, and vehicle speeds up to 75 miles per hour.2-4 Studies using US Consumer Product Safety Commission data have shown that young ATV riders are at higher risk for injury and death. Among ATV users, riders who are younger than 16 years encompass only 18% of users but represent 28% of ATV-related injuries and 18% of ATV-related deaths. 5 ATV drivers younger than 16 years have almost 4 times the risk for injury compared with riders older than 16 years. When compared with ATV riders older than 45 years, riders younger than 16 years have 12 times the risk of injury. 3 Some authors posit that this risk is because of children’s lack of physical strength, higher order cognitive abilities, and the potential speed achievable by ATVs; this latter factor can make ATV operation more difficult than the operation of automobiles.2,6 These factors make ATV operation inherently dangerous, and many researchers have advocated for increased education programs and legislation to decrease the national ATV injury epidemic affecting this young population.
This study begins the process of determining if educational activities are effective in decreasing this injury risk. A collaborative, pilot project was developed between the Children’s Hospital of Illinois/OSF Saint Francis Medical Center and the Peoria County Sheriff’s Office to provide an ATV education and safety demonstration to rural students of Central Illinois, known as the Rural Youth ATV Safety Education Program. We sought to determine the effectiveness of this program for improving users’ ATV knowledge and safety practices.
Methods
The study used a descriptive research strategy with a one group pretest/posttest design. Pretest and posttest questionnaires surveyed participants’ knowledge about ATV safety, personal safety practices, ATV use patterns, and descriptions of ATV-related crashes and injuries. Rural middle and high schools throughout 3 counties of West-Central Illinois were approached for participation in the program. Administrators from 1 rural middle school and 2 rural high schools agreed to participate. The convenient sample consisted of the students present on the pretest/intervention day and then the posttest day. The institutional review board would not allow personal identifiers to match the students who were present on both days.
The intervention consisted of a standardized Microsoft PowerPoint lecture highlighting ATV usage and mechanics, injury risk factors, and recommended safety practices, coupled with a “hands-on” safety demonstration of relevant safety gear and ATV operation using full-sized ATVs and equipment. The intervention was conducted on school property, during scheduled class time. Prior to the intervention, pretest surveys were completed during homeroom class periods. Postintervention surveys were mailed to the school at least 12 weeks after the presentation and distributed by teachers to the same students who had previously participated.
Questions on the survey included student demographic information, ATV use patterns, ATV safety knowledge, protective equipment use, and history of ATV-related injuries and crashes. Community was defined as a rural area/not a farm, farm, small town (<10 000 people), or a city (>10 000 people). ATV safety knowledge questions were based on Illinois ATV regulations and adapted from several sources. ATV safety knowledge questions included identifying the appropriate locations to ride ATVs (trails and nonpaved surfaces), affirming that ATVs were not designed to carry passengers, identifying the correct type of helmet, identifying the recommended ATV size for participant’s age group, and identifying adolescent developmental characteristics that lead to higher injury rates (insufficient strength, cognitive abilities, and motor skills for adult-sized machines). Participants were queried about routine helmet and safety gear use (5-category, ordinal scale, using “always” to “never” as anchor points) and were asked if they had ever participated in an ATV safety course. Participants were asked to report any ATV crashes that occurred during the previous 6 months. If a participant indicated that they had been involved in a crash, a follow-up query asked if they had required medical attention.
A pilot study, performed in the previous year, allowed the questions to be evaluated and modified for clarity and responses to be grouped in categories. The pre and post responses were primarily analyzed using those respondents who reported having driven or ridden on an ATV over the past 6 months (riders). For the purposes of analysis, ordinal scale responses were grouped into representative dichotomous categories (“always” and “mostly” were grouped as positive responses; “neutral,” “not often” and “never” were grouped as negative responses). Chi-square tests or Fischer’s exact tests were used to examine differences between groups for nominal variables and t tests were used for interval variables. A significance level was accepted at P < .05. Student responses were combined into aggregate preintervention and postintervention categories because our institutional review board approval did not allow for individual respondent matching. The primary outcome for the study was collective ATV safety knowledge improvement (percentage change in the aggregate correct responses of the 5 ATV safety knowledge questions).
Results
The educational intervention was presented to rural Central Illinois adolescent youths at 3 sites that consisted of 2 high schools and 1 middle school. Of the participants, 207 responded to the preintervention survey (51.2% male, mean age 13.1 years), whereas 165 (55.5% male, mean age 13.2 years) completed the postintervention survey. Table 1 gives the characteristics of riders (drivers and passengers) and nonriders. Riders and nonriders were similar in age and school grade. Whereas the largest proportion of riders (55.8%) resided in small towns, of the 116 that reported living on a farm, 92.2% were riders. This contrasted with 74.6% of the 213 respondents living in a small town and 54.3% of the 35 respondents living in a city being riders. A larger percentage of riders (56.6%) compared with nonrider families (3.8%) owned an ATV. Of the riders, 82.8% reported riding an ATV within the past 6 months.
Characteristics of Survey Responders

Abbreviation: ATV, all-terrain vehicle.
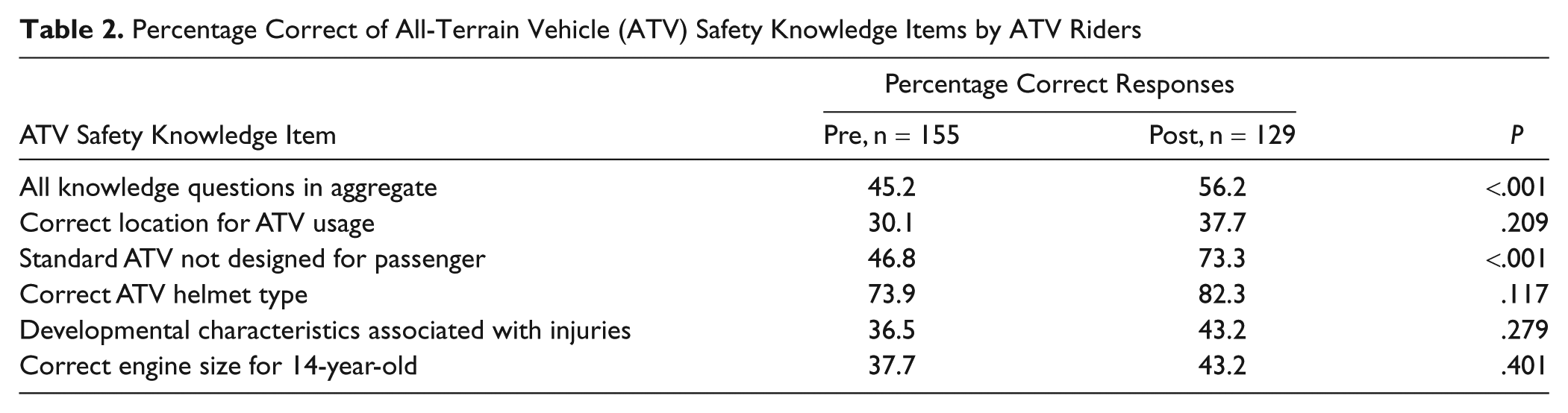
Among all riders students increased significantly in their overall knowledge from the preintervention survey to postintervention survey (45.2% vs 56.2% correct; P < .001) on the 5-knowledge-item test. The individual components of the test are listed in Table 2. Students gained significant improvement in recognizing that an ATV is not designed to carry passengers (P < .001). Although the remaining 4 items were more frequently answered affirmatively in the posttest compared with the pretest, there was no significant difference for the correct location for ATV usage, correct helmet type, risk of injury compared with adult rider and correct engine size.
Percentage Correct of All-Terrain Vehicle (ATV) Safety Knowledge Items by ATV Riders
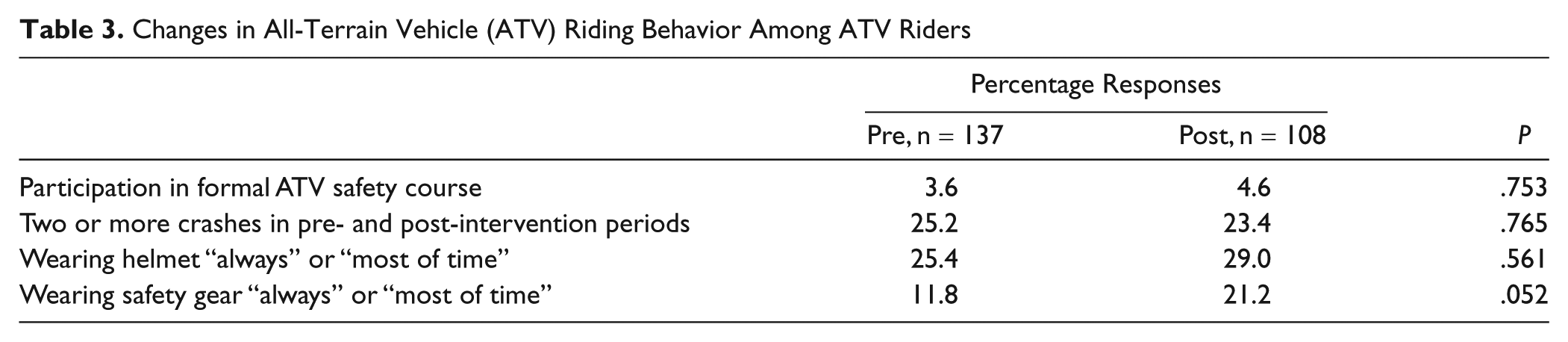
None of the changes in the 4 ATV riding behaviors among those reporting to have ridden in the last 6 months were significant for the pretest–posttest differences (see Table 3). A slightly larger proportion reported 2 or more crashes in the preperiod than in the postperiod. The participation in other ATV safety courses, always or most of the time wearing a helmet or safety gear increased slightly from the pretest to the posttest.
Changes in All-Terrain Vehicle (ATV) Riding Behavior Among ATV Riders
Discussion
Investigations of ATV-related injuries have shown the risk of injury is higher for young ATV riders. One study has demonstrated children have 4.7 times the risk compared with adults for involvement in a right-sided rollover, even when excluding collision crashes. 7 The high risk of injury for ATV riders younger than 16 years is also shown through ATV-related hospitalizations and the associated cost impact. From 2000 to 2004 there were an estimated 58 254 hospitalizations related to ATVs and of these admissions, 30% were younger than 18 years. The highest rate of ATV-associated hospitalization per 100 000 population was in the younger than 18 years age-group. 8 In a study comparing the years 1997 to 2000, an estimated $70 million in hospital charges accrued related to ATV injuries, with 20% of the charges being paid by public insurance. 9
These injury risks to adolescent ATV riders and their subsequent public health impact have led to advocacy efforts to decrease ATV-related injuries. The American Academy of Orthopaedic Surgeons, the American Academy of Pediatricians, and the Canadian Association of Pediatric Surgeons have issued policy statements that include limiting the operation of ATVs to a minimum age of 16 years.10-12 However, several studies have pointed out that similar enacted legislation has not been effective. For example, a study examining pediatric ATV incidents in Utah, another examining the short-term legislative impact in North Carolina, another describing injury patterns in Florida; as well as studies that compare states with the greatest and least ATV-related pediatric mortality with established state legislation, have all demonstrated that legislation in isolation is ineffective at preventing ATV-related injuries and mortality.13-17 Winfield et al 17 have advocated for legislation that promotes safety education and certification through knowledge and skill testing as an alternative to restrictive use legislation.
Determining the best strategy for implementing ATV educational programs has been investigated previously. Research using several focus groups investigated what type of education programs adults and teenagers view positively. Inclusion of ATV safety education in youth forums at school or as part of driver education programs was viewed most positively by these focus groups. 18 Of interest, findings from this research suggest that restricting age limit to those 16 years old and older was viewed negatively and would fail to affect the reality of ATV use. A study at the national convention for the Future Farmers of America found that nearly half the participants did not have ATV training available to them and suggested frequent dangerous behaviors that should be the focus of educational interventions. 19 It also has been shown that community-based prevention programs effectively increase safety knowledge and decrease injuries associated with various injury mechanisms, including drowning, traffic injuries, residential fires, bicycle accidents, tap water burns, and car accidents.20-26
Our ATV safety program was modestly effective at increasing ATV-related safety knowledge collectively. Several of the topics covered in the current intervention have been shown to be important safety topics to address with adolescent ATV riders. 19 However, individual safety issues, such as riding in the correct location, appropriate helmet type and usage, and adolescent developmental characteristics addressed in this ATV education intervention did not show significant knowledge improvement amongst adolescent ATV riders. Although addressed in the educational intervention, there were no knowledge changes noted for riders younger than 16 years using a recommended youth-sized ATV. This issue should be strongly addressed in any future interventions as nearly 90% of injuries to young ATV riders occur while using an adult-sized ATV.27,28 One possible way to address this safety issue is by focusing educational interventions on parents, as they represent the group actually purchasing the ATVs.
Even with an overall increase in safety knowledge, our nonsignificant changes in riding practices and crash rates demonstrate that youth behavior is more difficult to impact than knowledge. The results from this study indicate that the Rural Youth ATV Safety Education Program may be an effective first step to a much broader, community-based intervention that is needed to affect the safety knowledge and riding behavior of rural Central Illinois youths. A common element of successful adolescent bicycle helmet promotion programs is the use of multiple strategies targeted at different audiences to address the pivotal barriers.29,30 ATV safety educational interventions should not only target rural youths but also aim to influence the knowledge and behavior of the parents of these young operators, as well as community leaders and organizations. Although many injury prevention programs have included education and the distribution of discounted or free safety equipment, implementation of similar strategies for an ATV safety campaigns will be more difficult, given the use of the vehicles on private property, the diversity of vehicle types, the relatively high costs of recommended motorcycle helmets, and the low use of safety equipment at baseline. 18 In addition, effective safety knowledge transfer is not likely a linear process, but rather that it is an interactive, multidirectional process, that benefits from multiple interconnected interventions. 31 Therefore, using a wide variety of interventions and techniques (ie, hands-on training, safety courses, social marketing, safety regulation) may yield the best effect on adolescent ATV injury prevention.
Limitations of this study include the convenience sample and the inability to match preintervention and postintervention surveys to individual participants. Given the lack of previously published ATV safety programs in this population, we felt this enrollment model would provide basic data and trends regarding the intervention. As the present study was limited because of the convenient sample, a larger, randomized trial based on a power analysis needs to be conducted. As we were seeking self-reported information regarding risky behavior, it was felt that self-identification might have deterred individuals from truthfully completing the survey. This limited tracking those participants that dropped out of the study and prevented the matching of individual results on pretests and posttests. Although absences and students not returning the postintervention surveys account for the differences in numbers of surveys, the similarities in sample demographics from the preintervention to the postintervention surveys suggests that the population of students who received the educational intervention and completed the preinterventional and postinterventional survey were similar. The study participants were all from rural Central Illinois and regional differences in ATV operation and legislation may limit the generalizability of the results. We inquired into ATV crashes and related injuries; however, this study was underpowered to determine if the intervention caused any change in ATV-related injuries or fatalities. The sporadic nature of ATV-related injuries requires a much larger population base beyond the scope of this investigation.
Conclusions
In conclusion, our Rural Youth ATV Safety Education Program was effective at increasing ATV safety knowledge in rural Central Illinois youths. However, affecting the behavior of young ATV operators was not successful and represents a much more challenging initiative. In the future, the design and implementation of a community-based, multi-agency ATV injury prevention intervention might benefit by targeting not only youths but also their parents to improve its impact.
Footnotes
Authors’ Note
This study was presented as a poster at the 138th American Public Health Association Annual Meeting and Exposition, Injury Control and Emergency Services Section, Denver, Colorado, November 2010.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for this study was provided through a Robert Wood Johnson Grant for the Injury Free Coalition for Kids of Peoria.