
Abstract
The status of the primary care workforce is a major health policy concern. It is affected not only by the specialty choices of young physicians but also by decisions of physicians to leave their practices. This study examines factors that may contribute to such decisions. We analyzed data from a 2009 Commonwealth Fund mail survey of American physicians in internal medicine, family or general practice, or pediatrics to examine characteristics associated with their plans to retire or leave their practice for other reasons in the next 5 years. Just over half (53%) of the physicians age 50 years or older and 30% of physicians between age 35 and 49 years may leave their practices for these reasons. Having such plans was associated with many factors, but the strongest predictor concerned problems regarding time spent coordinating care for their patients, possibly reflecting dissatisfaction with tasks that do not require medical expertise and are not generally paid for in fee-for-service medicine. Factors that predict plans to retire differ from those associated with plans to leave practices for other reasons. Provisions of the Patient Protection and Affordable Care Act that reduce the number of uninsured patients as well as innovations such as medical homes and accountable care organizations may reduce pressures that lead to attrition in the primary care workforce. Reasons why primary care physicians’ decide to leave their practices deserve more attention from researchers and policy makers.
Keywords
Assessments of the state of primary care in the United States generally point to both its importance and its poor condition.1-3 Primary care physicians make up less than 40% of the physician workforce, 4 and the small number of new physicians who choose to go into primary care fields is a serious policy concern. Primary care physicians’ continuation in practice has received less attention, with a primary research focus on psychological factors such as stress and job satisfaction. 5 However, when asked in the Commonwealth Fund’s 2009 Survey of Primary Care Doctors in 11 countries if they plan to leave their medical practice in the next 5 years, some 42% of American primary care physicians indicated that they might. In only one country (Sweden) was the percentage higher. In this article, we examine practice characteristics associated with American primary care physicians’ plans to retire or leave their practice for other reasons in the next 5 years.
Methods
We used data from a 2009 Commonwealth Fund mail survey of 1442 American physicians practicing internal medicine, family or general practice, or pediatrics. The response rate was 39%, and the sample was weighted to reflect the characteristics of the physician population. 6 We focused on physicians who, when asked if they planned to leave their practice in the next 5 years, indicated that they planned to retire, planned to leave for “other reasons,” or were uncertain about leaving or continuing. (The exact question was “Do you plan to leave your medical practice within the next 5 years? Yes, retiring; Yes, leaving for other reasons; No; Not sure.” Given the wording of the survey question, we are unable to distinguish between physicians planning to leave practice altogether, to leave a primary care specialty, or to move in some other way. It should also be understood that planning to retire or leave one’s practice is not the same as doing so, but it seems to be a reasonable indicator of such intents.) In our analyses, we combined these latter 2 responses to identify physicians who “might leave” their practice for reasons other than retirement. We excluded physicians under age 35 years from the analysis because planning to leave their practice might reflect transitions typical of early stages of a medical career.
Reasons for planning retirement may differ from other reasons for leaving one’s practice, so we examined 3 groupings of physicians: (1) those above age 50 years who plan to retire, (2) those above age 50 years who might leave their practice for other reasons, and (3) those aged 35 to 49 years (referred to as “younger physicians”) who might leave their practices.
We examined factors that could increase or decrease the probability of planning to leave one’s practice, including 3 sets of policy-relevant variables that might, we hypothesized, affect quality of a physician’s work life:
having patients who experience problems obtaining needed care;
practice-related problems; and
use of information technology.
We hypothesized that the first 2 of these would increase physicians’ plans to leave their practices and that the latter would reduce such plans.
We performed a bivariate analysis of our control and hypothesis variables’ relationship to physicians’ leaving plans and a multiple regression analysis of the 3 sets of variables mentioned above, controlling for
physician gender and specialty;
practice characteristics: location, payer mix, and type and size of practice; and
work characteristics: hours worked, number of patients seen per week, and percentage of time spent with patients.
Within each age group, we used t tests to analyze differences between physicians within a category and all other physicians regarding having plans to leave. Descriptive statistics for these variables are presented in the 2 Appendix tables.
The multivariate regression models for physicians 50 years and older are estimated as multinomial logit models, with “not planning to leave” as the base outcome. The multivariate regression models for physicians 35 to 49 years are estimated as standard logit models, with “not planning to leave” as the base outcome.
Results
Table 1 shows that just over half (53%) of the physicians aged 50 years or older plan to retire or leave their practice for other reasons and that 30% of physicians aged 35 to 49 years indicated that they might leave their practices.
Percentage of American Primary Care Physicians Aged 35 Years and Older Planning to Leave Their Practice Within the Next 5 Years (by Age Group)

Note: Authors’ analysis of data from the 2009 Commonwealth Fund international health policy survey of primary care physicians.
Table 2 shows how such plans vary by physician, practice, and work characteristics. Table 3 presents comparable estimates of the share of physicians who might leave among those reporting patient difficulties, practice problems, and use of health information technologies (HIT). Table 3 also shows which predictors were statistically significant in a multivariate analysis, controlling for the physician, practice, and work characteristics in Table 2.
Percentage Planning to Leave Among Physicians Reporting Selected Characteristics
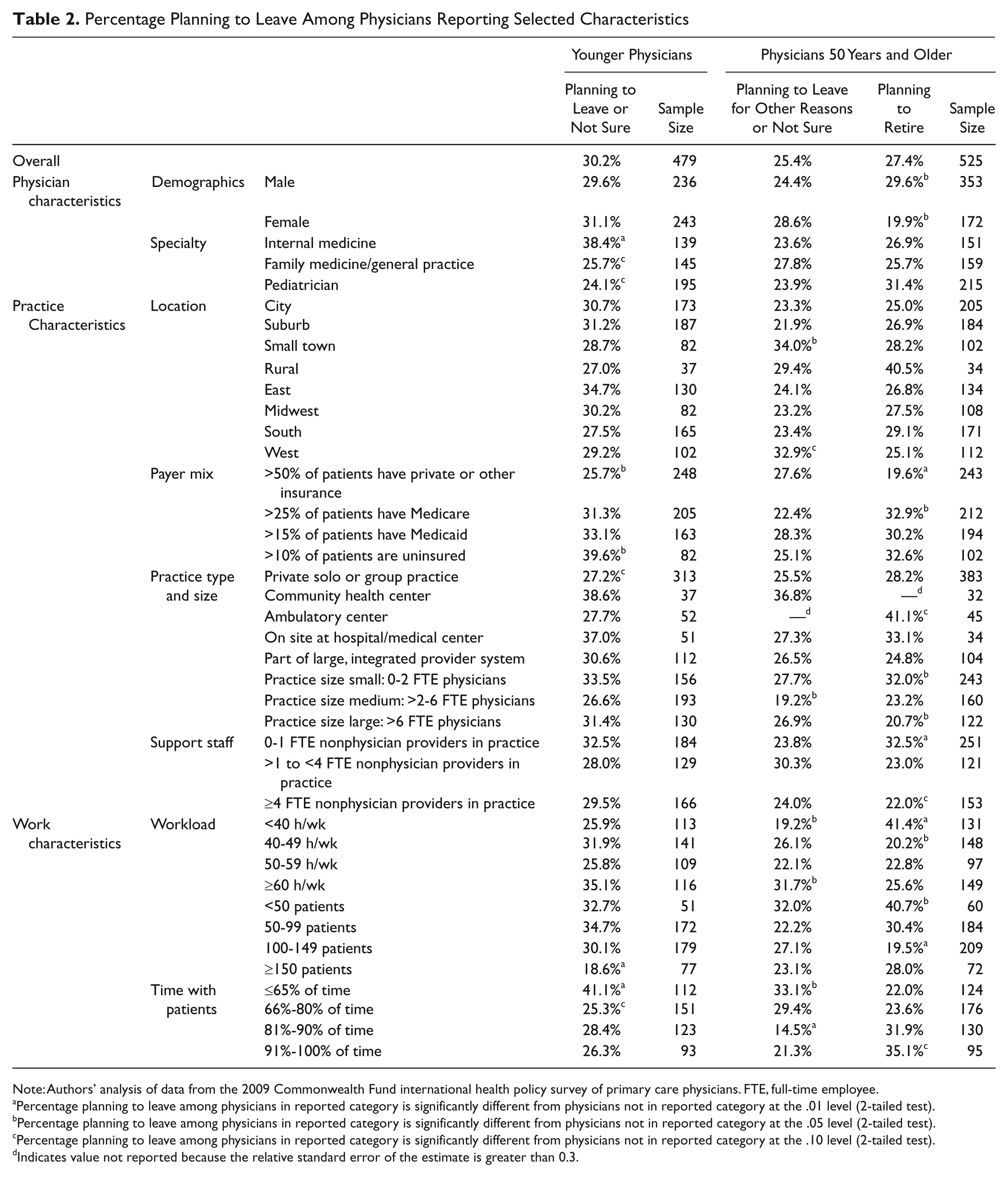
Note: Authors’ analysis of data from the 2009 Commonwealth Fund international health policy survey of primary care physicians. FTE, full-time employee.
Percentage planning to leave among physicians in reported category is significantly different from physicians not in reported category at the .01 level (2-tailed test).
Percentage planning to leave among physicians in reported category is significantly different from physicians not in reported category at the .05 level (2-tailed test).
Percentage planning to leave among physicians in reported category is significantly different from physicians not in reported category at the .10 level (2-tailed test).
Indicates value not reported because the relative standard error of the estimate is greater than 0.3.
Percentage Planning to Leave Among Physicians Reporting Explanatory Variables of Interest and Significance of Explanatory Variables in Multivariate Analysis
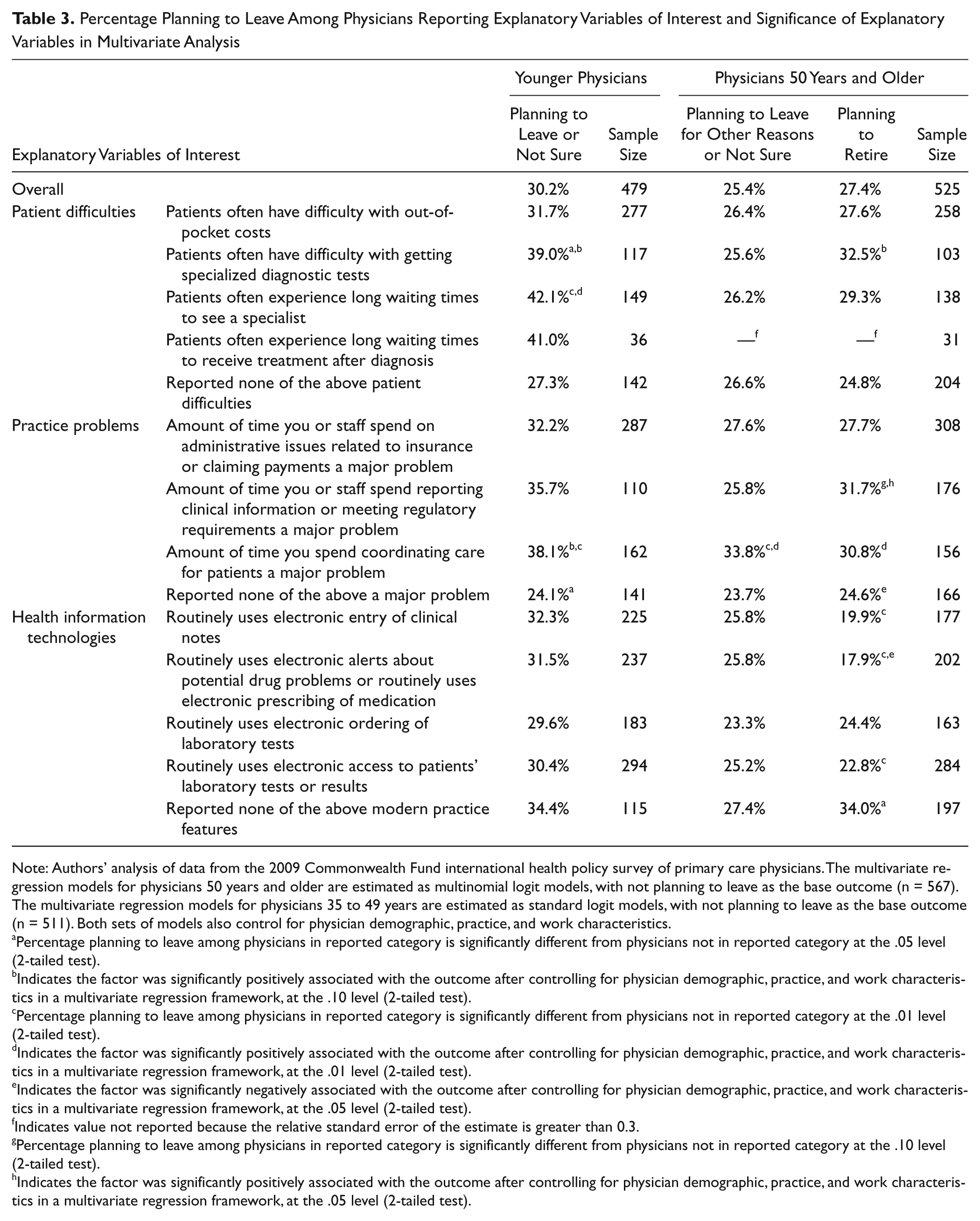
Note: Authors’ analysis of data from the 2009 Commonwealth Fund international health policy survey of primary care physicians. The multivariate regression models for physicians 50 years and older are estimated as multinomial logit models, with not planning to leave as the base outcome (n = 567). The multivariate regression models for physicians 35 to 49 years are estimated as standard logit models, with not planning to leave as the base outcome (n = 511). Both sets of models also control for physician demographic, practice, and work characteristics.
Percentage planning to leave among physicians in reported category is significantly different from physicians not in reported category at the .05 level (2-tailed test).
Indicates the factor was significantly positively associated with the outcome after controlling for physician demographic, practice, and work characteristics in a multivariate regression framework, at the .10 level (2-tailed test).
Percentage planning to leave among physicians in reported category is significantly different from physicians not in reported category at the .01 level (2-tailed test).
Indicates the factor was significantly positively associated with the outcome after controlling for physician demographic, practice, and work characteristics in a multivariate regression framework, at the .01 level (2-tailed test).
Indicates the factor was significantly negatively associated with the outcome after controlling for physician demographic, practice, and work characteristics in a multivariate regression framework, at the .05 level (2-tailed test).
Indicates value not reported because the relative standard error of the estimate is greater than 0.3.
Percentage planning to leave among physicians in reported category is significantly different from physicians not in reported category at the .10 level (2-tailed test).
Indicates the factor was significantly positively associated with the outcome after controlling for physician demographic, practice, and work characteristics in a multivariate regression framework, at the .05 level (2-tailed test).
Leaving Plans of Younger Physicians
Table 2 shows that plans for or uncertainty about leaving their practice in the next 5 years were more common among internists (38%) than among pediatricians or family/general practitioners. Geographic factors made little difference. Similarly, practice size was not associated with plans regarding leaving, nor was being in a large, integrated provider system such as Kaiser or the Veterans Health Administration (VHA). Physicians in private solo or group practice or a hospital-affiliated clinic were the most unlikely to plan to leave.
Payer mix was related to younger physicians’ plans to leave their practice. Among those who had more than 10% uninsured patients, 40% had leaving plans, while only 26% of physicians having more than 50% privately insured patients had such plans. High percentages of Medicare or Medicaid patients were not associated with leaving plans.
Regarding work characteristics, leaving plans were elevated (35%) among physicians who worked long hours (60 or more per week), but only 19% of the physicians who saw 150 or more patients in an average week had such plans. Two interpretations are possible. Perhaps these physicians value seeing many patients, an interpretation that is supported by the finding (Table 2) that those who spent the least time seeing patients were particularly likely (41%) to plan to leave. Alternatively, seeing larger numbers of patients may produce higher incomes, which could lessen physicians’ interest in leaving their practices. Unfortunately, satisfaction with income was not included in the survey.
Leaving plans were particularly common among younger physicians whose patients often experienced difficulty obtaining needed specialty services (Table 3). This relationship was also significant in the multivariate analysis. Similarly, those who said that the amount of time they spent coordinating patients’ care was a major problem were particularly likely to have leaving plans (also significant in the multivariate analysis). Physicians who had none of the practice problems included in the survey were significantly less likely to have leaving plans, although not in the multivariate analysis.
Contrary to expectations, younger physicians whose practices used HIT were no less likely to have leaving plans than were physicians whose practices did not.
Plans of Older Physicians
Primary care physicians age 50 years and older were more likely than younger physicians to plan to leave their practices but were slightly less likely than younger physicians (25% vs 30%) to consider leaving their practices for reasons other than retirement. The predictors of older physicians’ plans to retire and to leave their practices for other reasons differ from each other, and both differ somewhat from predictors among younger physicians.
In Table 2, medical specialty was not related to older physicians’ plans to leave their practices, but like younger physicians, older physicians practicing in settings other than private solo or group practice more likely had plans to leave. Practice location was also related to leaving plans among older physicians, with those practicing in rural areas particularly likely to have plans to retire and those in small towns particularly likely to have leaving plans for other reasons. By contrast, older physicians with suburban practices were particularly unlikely to have plans to leave for reasons other than retirement.
Older physicians were similar to the younger in that the likelihood of leaving for nonretirement reasons was relatively high for those working more than 60 hours a week and for those spending less than 66% of their time with patients. Older physicians who worked fewer than 40 hours per week were particularly unlikely to have leaving plans for reasons other than retirement.
Having unusually high numbers of Medicare, Medicaid, and uninsured patients all increased the likelihood of having retirement plans; physicians for whom more than half of their patients were privately insured were unlikely to plan retirement. Retirement plans were most common among physicians who practiced alone or with one other physician, and physicians in groups of 6 or more were particularly unlikely to have such plans. Older physicians who spent the most time with patients were more likely to plan retirement.
In Table 3, older physicians’ plans to leave for nonretirement reasons were less sensitive to patients’ difficulties and to practice problems than were such plans among younger physicians. However, in both age groupings, planning to leave practice was particularly common among physicians for whom time spent coordinating patients’ care was a major problem.
Having patients who had difficulty getting specialized diagnostic tests increased chances that older physicians would plan retirement, and time spent meeting regulatory requirements and coordinating patients’ care was associated with higher rates of retirement planning among older physicians in the multivariate analyses. Consistent with this, having support staff to perform functions like executing standing orders for patients lowered the likelihood of older physicians’ plans to retire (data not shown).
As with the younger physicians, use of HIT in their practices had no relationship to older physicians’ plans to leave for nonretirement reasons. However, HIT was associated with significantly lower rates of retirement plans.
Discussion
Although our cross-sectional data do not support causal connections, we have identified factors associated with elevated or depressed interest among primary care physicians in leaving their practices for retirement or other reasons. As such, our results complement earlier research that has focused on psychological measures such as stress and satisfaction.
Our survey data did not include information about income, but it contains hints that income may be affecting plans to retire or leave practice for other reasons. Having a particularly large share of privately insured patients is associated with lower rates of such plans. Treating large numbers of uninsured patients is associated with high rates of plans to leave among younger physicians, and treating large numbers of Medicare patients is associated with retirement plans among older physicians. Younger physicians who see an unusually large number of patients per week (>150) are particularly unlikely to plan to leave their practices.
Regarding the much expressed concern about the ability of the nation’s primary care workforce to meet the increased demand resulting from the Affordable Care Act (ACA), it is notable that the busiest older physicians (seeing >150 patients per week) were not more likely than others to have retirement plans, and among both age groups, the busiest physicians were particularly unlikely to plan to leave their practices. This provides a note of optimism regarding how primary care physicians will respond to the increased demand from newly insured patients.
Our data also suggest that 2 recent policy initiatives might reduce attrition from the primary care workforce. First, the coverage expansions resulting from the ACA should reduce the number of uninsured patients faced by primary care physicians. Having 10% or more of such patients in their practices was associated with younger physicians’ plans to leave their practices and with elevated (although not statistically significant) retirement plans among older physicians.
Second, the association between using HIT and lower rates of retirement among older primary care physicians raises the possibility that policy initiatives to increase the use of HIT in health care may reduce attrition due to retirement. Possibly, however, retirement plans reduce the likelihood of acquiring such technology.
The measure most consistently and strongly associated with physicians’ plans to leave their practices for retirement or other reasons concerned the amount of time spent coordinating care for patients. This may reflect dissatisfaction with tasks that do not require their expertise but also the lack of compensation for such work. These possibilities reinforce the need to redesign primary care practice and payment methods. The ACA’s provisions regarding patient-centered medical homes and accountable care organizations may result in such changes, but that is still quite uncertain.
Finally, our data show that attrition from the primary care workforce belongs on the policy agenda alongside physicians’ decisions to go into primary care. Our analysis has identified some practice-related factors that may affect primary care physicians’ decisions to retire or leave their practices for other reasons, but this is a topic that deserves much additional attention from researchers and policy makers.
Footnotes
Appendix
Means of Hypothesis Variables for Samples of American Physicians Aged 35 to 49 Years and 50 Years and Older
| Younger Physicians Aged 35-49 Years | Physicians 50 Years and Older | ||
|---|---|---|---|
| Patient difficulties | Patients often have difficulty with out-of-pocket costs | 60.7% | 52.9% |
| Patients often have difficulty with getting specialized diagnostic tests | 25.9% | 22.5% | |
| Patients often experience long waiting times to see a specialist | 29.1% | 24.8% | |
| Patients often experience long waiting times to receive treatment after diagnosis | 7.5% | 7.0% | |
| Reported none of the above patient difficulties | 28.5% | 37.2% | |
| Practice problems | Amount of time you or staff spend on administrative issues related to insurance or claiming payments a major problem | 63.8% | 60.8% |
| Amount of time you or staff spend reporting clinical information or meeting regulatory requirements a major problem | 24.6% | 35.4% | |
| Amount of time you spend coordinating care for patients a major problem | 36.1% | 31.0% | |
| Reported none of the above a major problem | 27.2% | 30.3% | |
| Health information technologies | Routinely uses electronic entry of clinical notes | 48.7% | 31.7% |
| Routinely uses electronic alerts about potential drug problems or routinely uses electronic prescribing of medication | 51.0% | 38.1% | |
| Routinely uses electronic ordering of laboratory tests | 41.2% | 30.5% | |
| Routinely uses electronic access to patients’ laboratory tests or results | 63.3% | 53.9% | |
| Often or sometimes communicates with patients by email | 5.0% | 2.1% | |
| Reported none of the above modern practice features | 23.7% | 39.3% | |
| Sample size | 479 | 525 | |
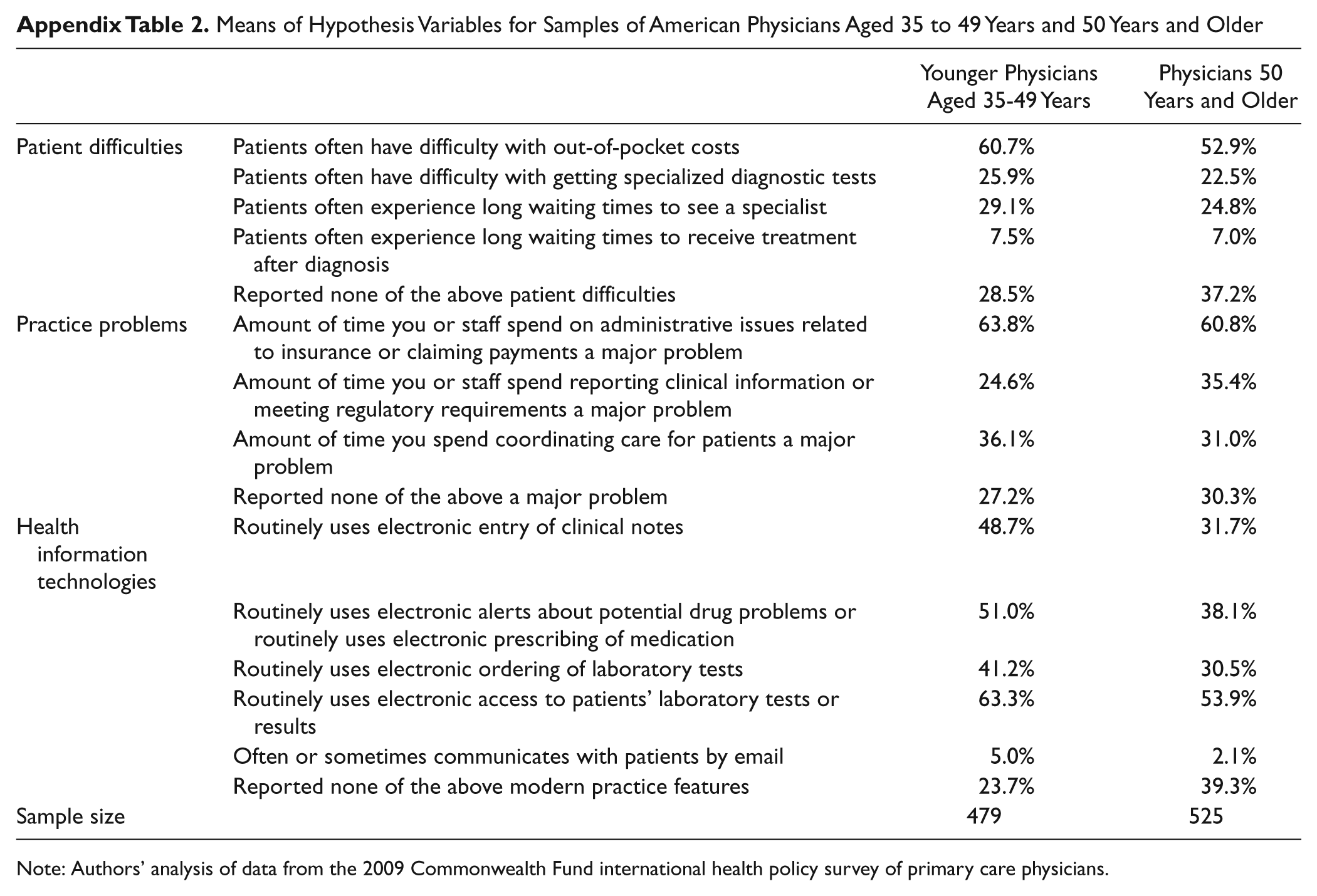
Note: Authors’ analysis of data from the 2009 Commonwealth Fund international health policy survey of primary care physicians.
Acknowledgements
The authors are grateful for the assistance of David Squires and Eva Hruba in the preparation of this article.
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author(s) declared the following financial support for the research, authorship, and/or publication of this article: This research was supported by The Commonwealth Fund.