
Abstract
Many adults continue driving into old age, 1 and there will be over 50 million older drivers by 2020. 2 There are clear benefits to seniors who drive, because driving enhances independence, 3 facilitates involvement in community activities 4 and possibly prevents mental5,6 and physical health problems.7-9 There are also risks to continued driving, as numerous age-related changes affect driving ability,7,10,11 although “smart chips” and other new automobile technologies may help older drivers compensate. Older drivers tend to drive shorter distances and less frequently, 9 thus limiting motor vehicle crash exposure and the risk they pose to the community, 12 but their rates of crash involvement per mile of travel remain high.12,13
It appears important to balance the risks and benefits of continued driving, but it remains unclear how to identify at-risk elderly drivers, and state regulations vary widely. 14 Mandatory age-based testing alone does not appear to prevent crashes or save lives,9,15 and it may result in drivers giving up their licenses rather than taking a test they may actually pass. 9
Older drivers’ opinions concerning mandatory testing have varied in prior work.16-18 Also, little is known about older drivers’ opinions regarding who should advise them when it is time to stop driving. We conducted this survey of older adults to measure (1) support for mandatory age-based testing and (2) willingness to follow driving recommendations from physicians or family members. A better understanding of older drivers’ expectations and attitudes may inform driver safety program development and clinical care.
Methods
We surveyed a cross-sectional sample of patients visiting the emergency department (ED; 7
Survey questions came from existing questionnaires,21,22 and additional new questions were pilot-tested in an older adult population for clarity and content. We reviewed participant charts for current medications and medical diagnoses in categories defined a priori based on conditions previously identified as increasing driving risk.7,11
Current drivers were those who reported driving a motor vehicle everyday or almost every day or occasionally. Current drivers were asked about motor vehicle crash involvement during the past 12 months while driving, whether at fault or not. Additional questions assessed opinions about mandatory age-based testing and decisions about license revocation and willingness to follow driving recommendations.
For analysis, we described participants’ responses, medication use, and diagnoses using proportions and 95% confidence intervals (CIs). We used χ2 analyses to test for associations between the driver opinions of interest (willingness to stop driving if recommended by physician, family, or friends) and driver characteristics. To measure the strength of these relationships, we calculated odds ratios (OR) with 95% CIs.
Results
During enrollment periods, 694 adults aged ≥ 65 visited the clinic or ED. Of these, 304 (43.8%) were ineligible, and another 50 (7.2%) were not approached, because research staff were busy. Of the 340 approached, 171 (50.4%) enrolled; 2 later withdrew and were excluded from analysis. Approximately half (59.3%) were enrolled in the ED. Clinic participants were older (mean age, 79.5 vs 73.8 years) and were taking more medications (9.2 vs 6.0) than ED participants but were otherwise similar.
Half the participants were women, and the majority rated their overall health as good or better and lived independently (Table 1). Among current drivers, 84.1% (95% CI, 77.8-90.4) had at least 1 medical diagnosis previously linked to increased driving risk, and nearly one-third (31.1%; 95% CI, 23.1-39.1) were taking 10 or more medications.
Characteristics of Participants (N = 169) a
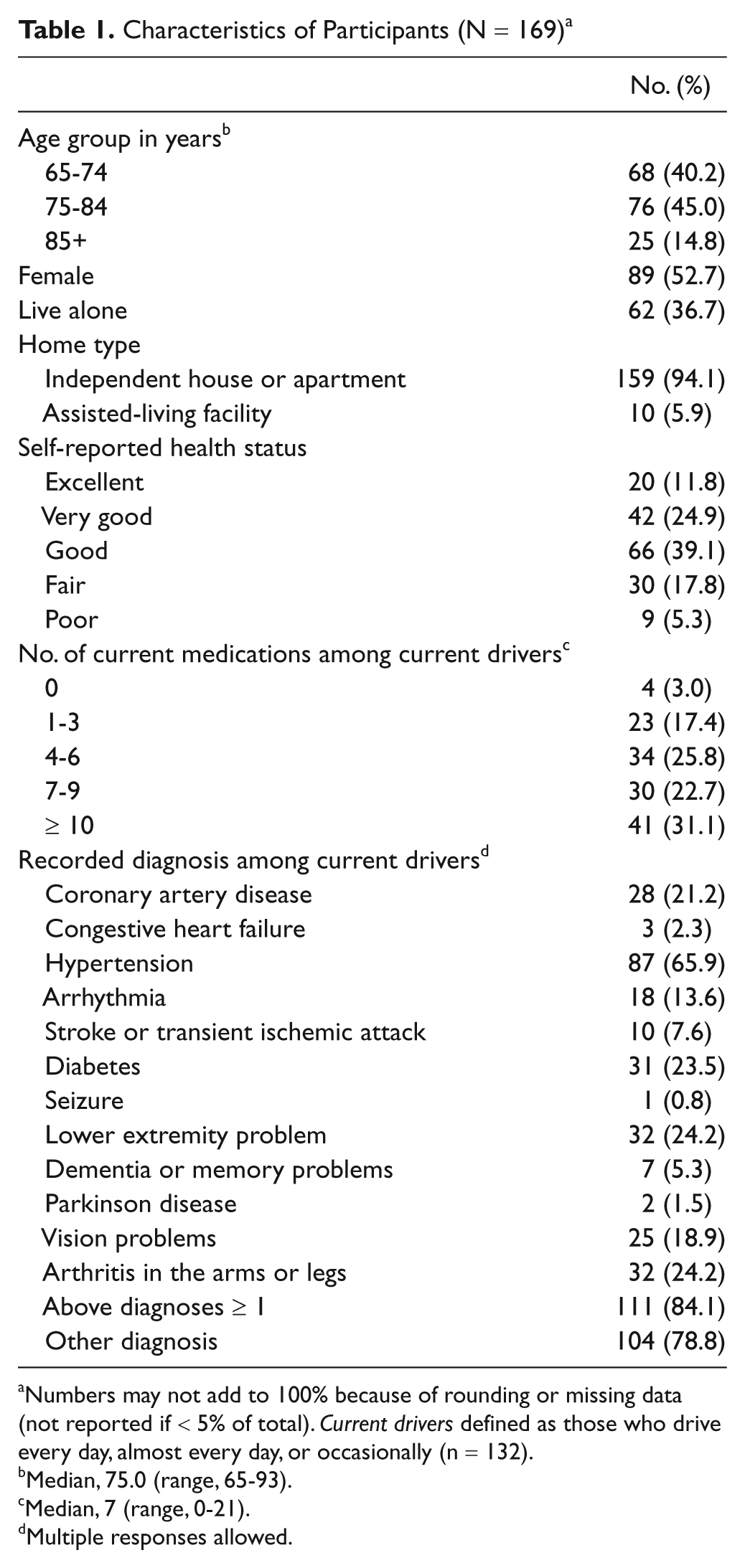
Numbers may not add to 100% because of rounding or missing data (not reported if < 5% of total). Current drivers defined as those who drive every day, almost every day, or occasionally (n = 132).
Median, 75.0 (range, 65-93).
Median, 7 (range, 0-21).
Multiple responses allowed.
Over three-fourths (78.1%; 95% CI, 71.8-84.4) of older adults were current drivers, and 11.4% (95% CI, 5.9-16.8) of drivers reported motor vehicle crash involvement as a driver in the past 12 months, without significant differences by age (Table 2). Just 3.8% (95% CI, 0.5-7.1) had been asked to stop driving in the past year.
Experiences and Opinions of Participants (N = 169) a

Numbers may not add to 100% because of rounding or missing data (not reported if < 5% of total). Current drivers defined as those who drive every day, almost every day, or occasionally (n = 132).
Multiple responses allowed.
A majority (74.0%; 95% CI, 67.3-80.6) agreed or strongly agreed with mandatory age-based testing for driver’s license renewal. Fewer thought that the state driver’s license office (34.2%; 95% CI, 27.6-42.2) or the police or court system (29.6%; 95% CI, 23.2-37.4) should determine license revocation for unsafe drivers. Far more stated that family members (73.4%; 95% CI, 68.0-81.4) or physicians (60.4%; 95% CI, 54.0-68.9) should make the license revocation decisions.
Almost all (93.2%, 95% CI, 88.9-97.5) drivers said they would or maybe would take a driving evaluation if recommended by a physician. Far more drivers said they would stop driving if recommended by a physician (62.1%) than if recommended by a family member or friend (33.3%; P < .001). Women appeared more likely than men to stop driving if instructed by a physician, although the association was not statistically significant (OR, 2.15; 95% CI, 0.65-7.13; P = .2). Compared with drivers aged ≥ 75, drivers aged 65 to 74 appeared more likely to stop driving if recommended by a family member or friend (OR, 2.39; 95% CI, 0.95-6.04; P = .06) but equally likely if recommended by a physician (OR, 0.91; 95% CI, 0.36-2.31; P = .9). Not surprisingly, drivers who felt that a physician should determine license revocation for unsafe drivers were more likely to say they would stop driving if recommended by a physician (OR, 2.82; 95% CI, 0.86-9.26) than if by a family member or friend (OR, 0.70; 95% CI, 0.14-3.43). However, drivers who felt that a family member should decide were more likely to stop driving if recommended by a family member or friend (OR, 7.37; 95% CI, 2.35-23.10) than if by a physician (OR, 0.91; 95% CI, 0.28-2.95).
Discussion
In this sample of older patients at a geriatric clinic or ED, over three-fourths reported driving at least occasionally, similar to other estimates.23,24 Twelve percent of older drivers reported a crash while driving in the past year; almost all had at least 1 medical diagnosis previously linked to increased driving risk7,11; and most were taking a number of medications. However, just 4% had been asked to stop driving in the past year.
Participants voiced strong support for mandatory, age-based testing for license renewal, but when it comes to driving cessation, more felt that the driver, a physician, or a family member should decide when driving is no longer safe. Most older drivers reported that they would heed the advice of their doctor, family, or friends, and almost all said they would at least consider a driving evaluation if recommended by their physician. These findings support an important role for physicians in counseling patients about driving safety.10,11,16 Prior work has shown some differences by sex in driving behavior and cessation,9,25 and we found that women appeared more likely to follow a physician’s recommendation to stop driving.
Although physicians may be reluctant to begin these difficult conversations, 26 our study demonstrates that older drivers want to have them, and for some it will be especially important to involve family members. Our findings support the idea of “advanced driving directives,” similar to advanced directives for end-of-life care, where drivers identify the physician, family member, or friend whom they would want to help them decide about driving cessation.11,27 Physicians could recommend these forms to their patients long before driving safety is a real concern, thereby facilitating planning by patients and families and mitigating anxiety. Although not legally binding, a written and signed advanced driving directive could make later decisions easier and help physicians tailor care to patient wishes. One model is Hartford’s “Agreement With My Family About Driving” 28 ; however, this form refers only to family members without acknowledging the role of physicians or testing agencies, and it is unclear how it was developed or whether it has been tested. In planned studies, we will explore the idea of advanced driving directives with older drivers, family members, and providers to develop and pilot-test an advanced driving directive template. Additional studies could examine the impact of physician or family recommendations and the completion of an advanced driving directive on future driving behavior.
There are several limitations to consider. The study included 2 outpatient sites at 1 institution, and daytime ED enrollment might have introduced bias if driving characteristics and opinions varied by time of day. However, the prevalence of driving, medication use, and chronic medical problems was similar to that of prior studies, suggesting that our results are representative.29,30 The relatively high nonparticipation rate (50%) might also have introduced bias; while we assured participants of confidentiality, some may have declined out of fear of license loss. The survey relied on self-report without independent verification of driving patterns, motor vehicle crashes, or adherence to driving recommendations. Finally, our relatively small sample sizes limited our ability to compare other subgroups.
In conclusion, many older Americans drive, and many take medications or have conditions that could increase their crash risk. Older drivers’ opinions about driving cessation may influence their likelihood of following recommendations. Older drivers voiced strong support for mandatory age-based testing but were more likely to follow recommendations from physicians or family, thereby supporting a role for physician counseling, evaluations, and advanced directives for driving.
Footnotes
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author(s) declared the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Emergency Medicine Foundation (2009-2011 Research Fellowship); the Centers for Disease Control and Prevention (Grant Number 5 R49 CE001168); and the John A Hartford University of Colorado Denver Center of Excellence. Its contents are solely the responsibility of the authors and do not necessarily represent the official views of the funders. The author(s) received no personal financial support for the research authorship, and/or publication of this article.