
Abstract
Introduction
Obesity among adolescents has become a public health priority due to the dramatic increase in its prevalence.1-5 In 1970, only 5% of adolescents 12 to 19 years old were obese. 3 However, by 2008 the prevalence increased to 18.1%. 1-5 As a result of this epidemic, millions of American adolescents are at risk of developing serious health consequences, and the country is at risk of ballooning health care costs as this generation of adolescents becomes adults and suffers from an earlier onset of comorbidities such as type 2 diabetes, heart disease, and many types of cancer. 6-15
Due to the health and financial costs, it is essential to find effective treatments for obesity. Physicians are well positioned to help families facing the challenge of having an obese child. However, previous studies have outlined numerous barriers encountered by primary care physicians attempting to treat obesity. Primary care physicians cite problems such as limited time, poor reimbursement, lack of self-confidence in their ability to treat obesity, and low patient/parent motivation as impediments to treating obesity.16,17
In recognition of the need for more intensive interventions than are generally available in a primary care office, the American Academy of Pediatrics and American Medical Association Expert Committee on the Prevention and Treatment of Childhood Obesity recommends referral to a pediatric multidisciplinary weight management program (PMWMP) when primary care efforts have failed to achieve satisfactory results. 18 Primary care physician encouragement to make lifestyle changes has been shown in previous studies to be associated with improved weight-related efforts. 19 In adults, a physician raising the topic of weight loss is associated with a greater likelihood of obese patients attempting weight loss. 19 However, it is unknown how a physician’s recommendation to join a weight management program affects actual weight loss among adolescents. Therefore, our objective was to explore the reasons for enrollment in a multidisciplinary weight management program for adolescents and to determine whether enrollment due to a physician’s recommendation, versus other reasons for enrollment, is associated with greater weight loss.
Method
Study design
We performed a retrospective analysis of obese adolescents (12-18 years old, body mass index [BMI] ≥ 95th percentile) enrolled in the Michigan Pediatric Outpatient Weight Evaluation and Reduction (MPOWER) program.
Program overview
The MPOWER program is an intensive, family-focused multidisciplinary weight management program for adolescents 12 to 18 years old. This program incorporates medical evaluation and monitoring along with nutrition and physical activity components. In addition, it incorporates an intense behavioral protocol built on evidenced-based obesity interventions to optimize the likelihood of improved outcomes.20-22
Sample and recruitment
In order to participate in the MPOWER program, adolescents must have a BMI at or above the 95th percentile for their age and sex. BMI was calculated using the formula Weight (kg)/Height (m)2, and percentiles were determined using Centers for Disease Control age-specific and gender-specific growth charts. Adolescents were included in this analysis if they enrolled in the MPOWER program between April 2007 and March 2009 and if initial and 12-week measurements were obtained. MPOWER participants using obesogenic medications (i.e., steroids), and those with severe mental illness (e.g., uncontrolled bipolar disorder) were excluded from this analysis.
Measurements
Weight was measured at each visit to two decimal places via electronic scale with patients in light clothing and without shoes. Height was measured at the initial and 12-week visit via portable stadiometer. Reasons for enrollment in the MPOWER program were obtained from responses to a menu of options listed in the enrollment questionnaire. For each participant, this questionnaire was completed prior to their first visit, by their parent or their guardian. The reasons for enrollment listed were (1) concern about child’s physical health, (2) concern about child’s mental health, (3) concern about child’s physical appearance, (4) concern about people’s reactions to my child’s weight, (5) child’s desire to participate in program, (6) recommendation by child’s doctor, (7) family member recently diagnosed with an obesity-related illness, (8) family member has recently lost weight, (9) suggestion of family member, and (10) other. Parents were instructed to indicate using check boxes all the reasons that influenced their decision to enroll.
Data Analysis
Dependent variable
The dependent variable for this analysis was change in BMI over the course of 12 weeks in the MPOWER program.
Independent variables
The independent variables considered for this analysis were each of the reasons for enrollment, along with age, initial BMI, Medicaid status, race, and gender.
For each reason for enrollment, we computed the percentage of respondents endorsing that option. We then rank ordered the percentages to determine the most common response.
Bivariate analysis of change in BMI versus each independent variable was performed using simple linear regression. The predictors that were significantly associated with change in BMI at a P value < .05 were included in the multiple linear regression analysis.
All analyses were conducted using STATA 10 (Stata Corporation; College Station, TX). This study was approved by the Institutional Review Board of the University of Michigan Medical School.
Results
Study population
Of the 92 patients who enrolled in the MPOWER program during the study period and had measurement at weeks 1 and 12, 90 adolescents met the inclusion criteria. All 90 charts were reviewed and revealed the following demographic characteristics: 70% were female, and racial/ethnic breakdown was 57% white, 35% black, and 8% other (Hispanic, Asian, Native American Indian, and Middle Eastern). Of participants, 41% came from families with an income of less than $25,000 per year and were Medicaid enrollees. Mean age was 14.5 years old (range 12-18 years). All participants had a BMI at or above the 95th percentile at program entry; the mean initial BMI was 42 kg/m2 (range 29-70).
Reasons for enrollment
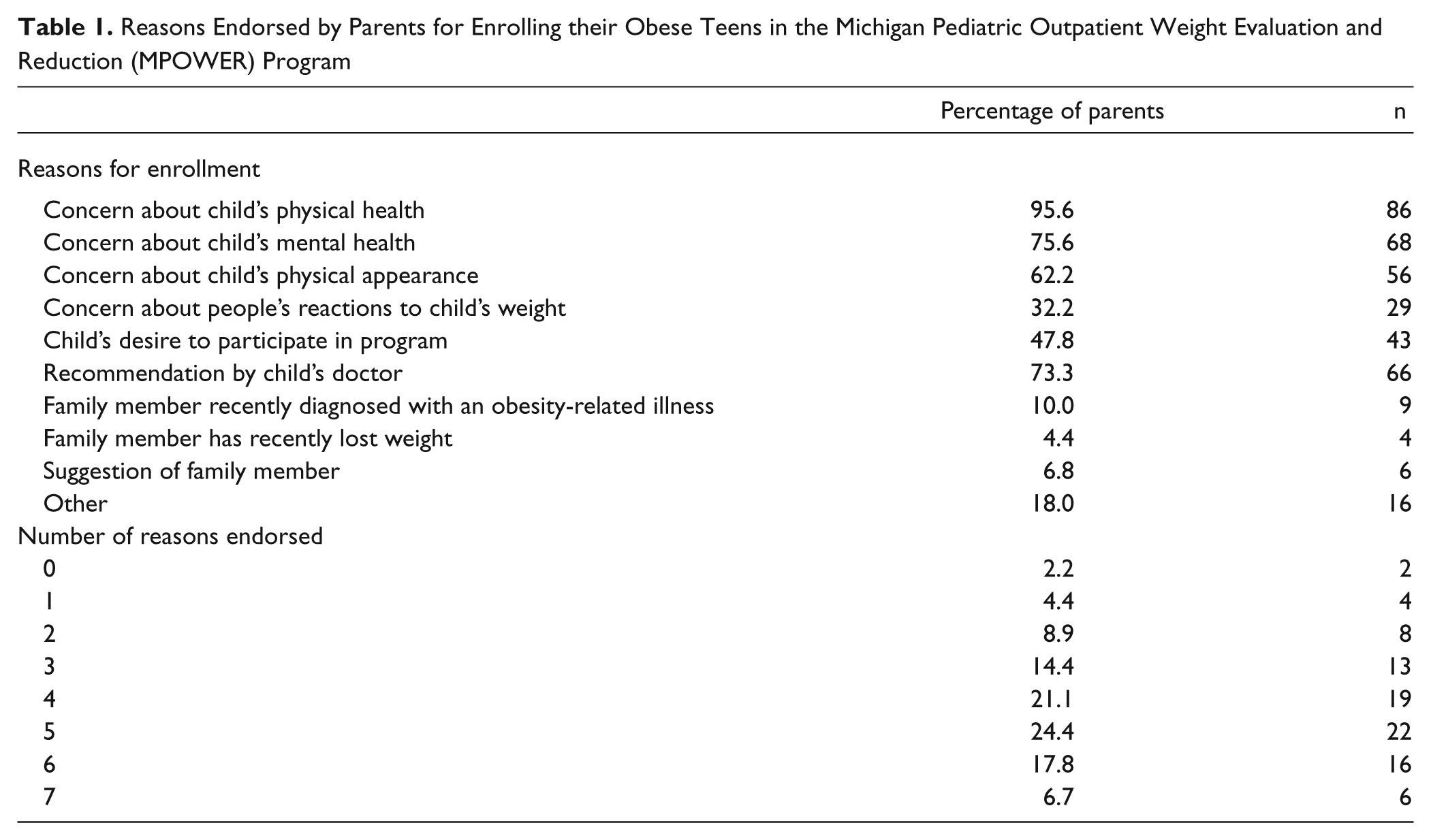
According to surveys completed at baseline, the most common reasons for enrolling in the MPOWER program were to improve the obese adolescent’s physical health (96%), to improve his or her mental health (76%), and because they were referred by their physician (73%) (Table 1). Only 48% enrolled because of the obese adolescent’s desire to participate.
Reasons Endorsed by Parents for Enrolling their Obese Teens in the Michigan Pediatric Outpatient Weight Evaluation and Reduction (MPOWER) Program
Association between reasons for enrollment and mean change in BMI
The mean 12-week change in BMI for adolescents whose parents indicated that they enrolled due to a recommendation from their child’s physician showed significantly greater decreases than those who did not indicate they enrolled due to a recommendation from their doctor (−1.5 vs −0.5 kg/m2: P < .05). This finding remained significant when, using multivariate analysis, we controlled for initial BMI and race (Table 2). Age, gender, and Medicaid status were not significant in bivariate analysis and therefore were not included in the final model. No statistically significant differences in mean BMI change were noted for the other reasons for enrollment.
Mulitvariate Regression for Change in Body Mass Index (BMI) by Physician Recommendation, Controlling for Initial BMI and Race

Number of observations = 90; F(3, 86) = 5.88; P = 0.0011; R2 = 0.17; adjusted R2 = 0.14.
Discussion
In this retrospective review of a clinical multidisciplinary program, we found that the most common reasons cited by parents for bringing their obese adolescents to the multidisciplinary weight management program were due to their concerns for their adolescent’s physical health, concern for his or her mental health, and due to a recommendation from their physician. In addition, adolescent’s appearance was an important factor for the majority of parents. Of note, adolescent’s desire to participate in the program was the reason for joining in less than half of cases. This may suggest that many adolescents may have had low motivation to engage in the weight management program. However, the fact that no statistically significant difference in change in BMI was noted for those who endorsed this as a reason for enrollment versus those who did not endorse this reason may reflect the importance of the parents’ role in weight loss efforts.
Few clinical weight management programs for adolescents have published outcomes, with most available data coming from randomized trials.23-25 These trials, such as the 2007 study by Savoye, often recruit patients for the purposes of research, compared to clinical programs where the participants seek treatment. 23 This likely explains why previous studies have not explored reasons for enrollment. Thus, this is the first study to our knowledge to find that adolescents who enroll in a weight management program due to their physician’s recommendation have greater decreases in their BMI than those who enroll for other reasons. This finding underscores the significance of primary care physicians in the battle against childhood obesity. The treatment of obesity among adolescents, as with adults, is challenging, and behavioral weight loss interventions in childhood have shown only modest success.23-25 The finding that a physician’s recommendation only accounted for 14% of the variance highlights the fact that a myriad of factors come into play when considering the results of weight loss efforts. However, if a physician’s recommendation might help, it presents a modifiable factor and potentially a feasible intervention that could be implemented in the primary care setting to improve outcomes for obese patients.
In the face of time constraints, reimbursement limitations, and low self-efficacy in the treatment of obesity, many physicians have difficulty following the guidelines even for the initial steps of screening for obesity (i.e., measuring and monitoring BMI), and many struggle with how to treat obesity once it is identified.26,27 From previous work we found that most will refer if the patient/family asks for a referral, 28 but this study suggests that it might be more effective if the physician raises the topic rather than waiting for the family to express concern.
Further work is required to explore the factors associated with a physician’s recommendation that are related to improved weight loss outcomes. It may be that the recommendation is enough, or possibly the discussion physicians have with families regarding the recommendation is the factor that increases their sense of the severity of the situation and increases their motivation to attempt change. This type of discussion may lengthen visits; however, particularly with the subpopulations of patients who are at greatest risk, the time taken to make a recommendation may be time well spent.
Limitations
This study was conducted among patients enrolled in one multidisciplinary weight management program. Results may differ by program. This was a retrospective analysis of cross-sectional data, therefore causation cannot be inferred. For this study we explored the change in BMI over a 12-week period; it is unknown whether the results would hold true over a longer period of time.
Conclusions
Physicians’ recommendation to a pediatric multidisciplinary weight management program for adolescents is associated with greater decreases in BMI than other reasons for enrollment. Physician recognition of obesity and discussions of this issue with patients may impact motivation to make lifestyle changes. Physicians should be encouraged to recommend lifestyle changes and participation in structured weight management efforts as this may lead to improved patient outcomes. Further work should explore how physician recommendation impacts long-term weight loss among obese adolescents.
Footnotes
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author(s) received no financial support for the research, authorship, and/or publication of this article.