
Abstract
Studies that assess health care use in older adults with and without dementia face several major challenges. These include ascertaining dementia status, measuring health care use, and adjusting for comorbidities. Most studies rely either on patient and informant reports or on medical claims data. Claims-based studies show that older adults with dementia use more medical care and incur higher medical costs than older adults without dementia.1-3 In these studies, the use of medical claims data to establish dementia cases creates at least two methodological issues. First, use of claims data likely underestimates true dementia-related utilization, as such data cannot capture undiagnosed dementia or the prodromal states preceding frank dementia. Second, because the same data are used to capture dementia cases and to measure outcomes, persons with higher costs may be preferentially ascertained, resulting in ascertainment bias. 4 Studies using claims-based data are therefore vulnerable to the twin problems of underestimating total utilization and cost, while overestimating the health care costs per person.
Studies that rely on patient and informant reports often use research quality evaluations to determine dementia status, which generally provide more consistent ascertainment of dementia status.5,6 However, these studies may need to rely on informants to obtain medical history and determine patterns of health care use. Abundant evidence suggests that such informant-based reporting is subject to bias, often failing to report utilization.7,8
Assessing the role of comorbidities is a third challenge. Serious medical conditions that are common in people with dementia increase the use and cost of health care services. 9 If comorbidites increase utilization independent of dementia status, any estimate of dementia burden should adjust for them. On the other hand, if comorbid disease is mediated by dementia status, then adjusting may lead to underestimates of dementia-attributable utilization.
To address these challenges, we systematically screened and diagnosed dementia in older adults participating in a longitudinal cohort study of dementia screening strategies in an urban geriatrics practice. To capture the range in severity of comorbidities, we then used the Cumulative Illness Rating Scale-Geriatrics (CIRS-G) a well validated measure of chronic medical burden for geriatric patients that indicates number and severity of comorbid disease.10,11 We avoided reliance on informant reports by reviewing medical charts to compile the CIRS-G. Finally, we used hospital-based claims data to assess utilization, focusing on emergency department (ED) visits and hospital admissions for 5 years following our initial assessment.
We expected that patients with very mild dementia would have more ED visits and hospitalizations than patients without dementia. This is because very mild dementia, which often goes unrecognized in primary care,12-14 may lead to poor adherence to medication and lifestyle management and a failure to optimally manage medical comorbidities. 15 This, in turn, may increase the use of acute care services and exacerbate cognitive impairment.1,5,16 Medical burden was expected to be a powerful predictor of both ED visits and hospital admissions as it is in most studies of dementia. 9 Finally, we sought to determine whether dementia status and medical burden were independent predictors of ED visits and hospitalizations.
Methods
Clinical Setting
The cohort consisted of 300 African American and Caucasian participants from the dementia screening project conducted in the Geriatric Ambulatory Practice (GAP), an urban academic primary care practice staffed by geriatricians in the Bronx, New York. Building on the Einstein Aging Study’s success in developing dementia screening tools, we developed and validated efficient two stage strategies for identifying early dementia and Alzheimer’s disease in primary care patients with comorbid medical conditions.17-19 Using clinical diagnosis as a gold standard, the strategies had high sensitivity and specificity for identifying early stage dementia. Sensitivity and specificity did not differ by race or education. Thus, these strategies provide an efficient approach to screening for very mild dementia in primary care. Recruitment began in January, 2003 and clinical follow-up was completed in July, 2007. The methods have been described in detail elsewhere. 17 All study procedures were approved by Montefiore Medical Center’s Institutional Review Board. Clinical Looking Glass, Montefiore’s clinical information system 20 was used to retrieve number of ED visits and hospitalizations provided by Montefiore Medical Center’s network through December, 2009.
Diagnostic Determination
The cognitive status of the 300 patients was established at baseline and follow-up according to the Diagnostic and Statistical Manual of Mental Disorders, 4th edition (DSM IV) criteria for dementia 21 using a comprehensive battery of neuropsychological tests and informant interviews. Patients were classified as having no dementia, prevalent dementia, or incident dementia by consensus of a neuropsychologist (EG), geriatrician (AE), and geriatric psychiatrist who also rated their functional capacity with the Clinical Dementia Rating (CDR) Scale. 22 The pattern of box scores determined the consensus CDR score and the sum of boxes indexed functional capacity.
Participants
Table 1 displays demographic information, medical burden scores, and screening test scores at baseline as a function of dementia status, which was determined independently of the screening tests. As usual, patients with dementia were older, had lower scores on tests of memory and cognition, and reported more depressive symptoms than patients without dementia. Though patients with dementia had less education than nondemented patients, the difference was not statistically significant. Neither sex nor race was associated with dementia status. Three-fourths of the prevalent dementia patients (35 of 46) had very mild dementia (CDR = 0.5); the other 11 had mild dementia (CDR = 1.0). Independent confirmation of early stage dementia was the absence of a dementia diagnosis in the chart notes for 59% of the patients diagnosed with dementia.
Demographic Information, Neuropsychological Test Scores, and Medical Burden Scores as a Function of Dementia Status at Baseline a

Abbreviations: CIRS, Cumulative Illness Rating Scale; FCSRT-IR, Free And Cued Selective Reminding Test With Immediate Recall; GDS, Geriatric Depression Scale; IQCODE, Informant Questionnaire On Cognitive Decline In The Elderly; MMSE, Mini Mental Status Exam score;
Minimum and maximum scores based on the 254 patients without dementia at baseline shown in parenthesis in notes b-h. T-test comparisons were performed except where noted.
Pearson chi square test.
MMSE (13, 30). 23
Sum of three trials of free recall from the FCSRT-IR (8, 44). 19
Number of animals, fruits, and vegetables generated in 60 seconds (9, 68). 25
Sum of two trials of clock drawing scored for numbers, hands, and center (4, 27). 26
Number of depressive symptoms endorsed (0, 12). 27
Average score (3 = no change in five years; and 4 = a bit worse) (2.5, 4.3). 28
Medical Comorbidity Index
The CIRS-G was used to evaluate conditions comorbid with dementia.10,11 The severity of comorbid conditions in 14 organ systems is individually rated on a scale from 0 to 4 (0 = no problem, 4 = extremely severe problem). The geriatric neurologist (AS) reviewed everything in the patient’s chart up to the date of the baseline assessment including problem lists, results of laboratory and diagnostic tests, current and past medications, and clinical notes from physicians and social workers. CIRS-G ratings were made in a manner consistent with published guidelines except for the psychiatric organ system that was recalculated to exclude dementia and Mini Mental State Exam (MMSE) scores 23 to avoid duplication of variance with clinical diagnosis. Our medical burden measure was the sum of severity ratings across all illnesses. Mortality was ascertained from the Clinical Looking Glass system, which records in-hospital deaths and deaths indicated in the National Death Registry
Statistical Methods
A series of paired comparisons examined differences in demography, neuropsychological test scores, and medical burden between patients with and without dementia at baseline. A series of nested models examined the effect of dementia status on number of ED visits and hospital admissions before and after adjustments for medical burden and functional capacity. Rates of acute care utilization were examined using marginal Poisson regression models fit with generalized estimating equations with exchangeable correlation structure; the robust “sandwich” variance estimator was used to calculate confidence intervals. Outcomes were the number of ED visits and hospital admissions, offset by follow-up time. Predictors were dementia status treated as a potentially time dependent variable, age at dementia assessment, medical burden indexed by the CIRS-G total score, and functional capacity indexed by the sum of CDR box scores. A secondary analysis used Cox proportional hazards models with age as the time scale to examine overall mortality as a function of these predictors, including dementia status as a potentially time dependent predictor. Utilization and mortality of patients with incident dementia were included with the data for patients without dementia until the date of their conversion to dementia. Analyses were performed using Stata SE, version 11.0 (Statcorp, LP, College Station, TX) and S-Plus, version 8.1 (TIBCO Spotfire software, Seattle, WA).
Results
Median follow-up time was 5.5 years (interquartile range, 4.3-6.1 years). The unadjusted medical burden score on the CIRS-G was no different for patients with and without dementia (Table 1).
ED Visits
Persons with dementia made 261 ED visits over 269 person-years of follow-up, for an unadjusted rate of 0.97 ED visits/year. Persons not diagnosed with dementia visited the ED 779 times over 1255.3 person-years of follow-up, for an unadjusted rate of 0.62 ED visits/year. Table 2 shows the incidence rate ratios for ED visits for persons with dementia versus persons with no dementia adjusted for age. Persons with dementia had a 49% higher rate of ED visits than persons without dementia (incidence rate ratio [IRR] = 1.49; 95% confidence interval [CI] = 1.06, 2.09; P = .023). The effect of dementia status was unchanged when medical burden (CIRS-G total score) was added to the model (Table 3). For each point increase of medical burden, there was an 11% higher risk of an ED visit (IRR = 1.11; 95% CI = 1.06, 1.16; P = .000). In the full model (not shown), functional capacity did not predict ED visits (P = .95), presumably because of its shared variance with dementia status. Age was not a significant predictor of ED visits in any model (P > .30).
IRRs for ED Visits as a Function of Age at Study Entry and Dementia Status
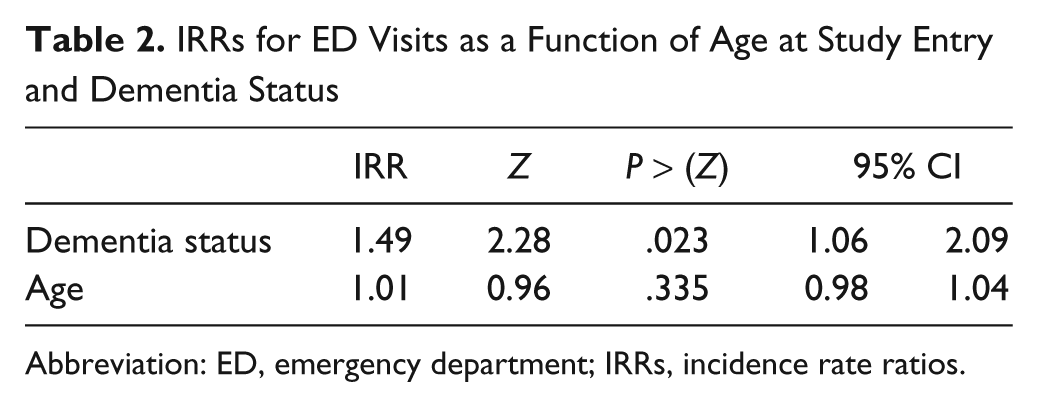
Abbreviation: ED, emergency department; IRRs, incidence rate ratios.
IRRs for ED Visits as a Function of Age at Study Entry, Dementia Status, and Medical Burden

Abbreviation: ED, emergency department; IRRs, incidence rate ratios.
Hospital Admissions
Persons diagnosed with dementia accounted for 173 inpatient hospital admissions over 269 person-years of follow-up, for an unadjusted rate of 0.64 admissions/year. In comparison, persons not diagnosed with dementia had 561 admissions over 1255 person-years of follow-up, for an unadjusted rate of 0.45 admissions/year. Table 4 shows the incidence rate ratios for hospital admissions for persons with dementia versus persons with no dementia. In the model adjusted for age only, dementia status did not predict hospitalizations (P = .08) though persons with dementia had a 37% higher rate than persons without dementia. Additional adjustment for medical burden (Table 5) strengthened the effect of dementia status (IRR = 1.37; 95% CI = 0.99, 1.89; P = .055). For each point increase of medical burden, there was a 13% higher risk of a hospital admission (IRR = 1.13; 95% CI = 1.09, 1.17; P = .000). As in ED visits, age and functional capacity did not predict hospitalizations (P >.45).
IRRs for Hospitalizations as a Function of Age at Study Entry and Dementia Status
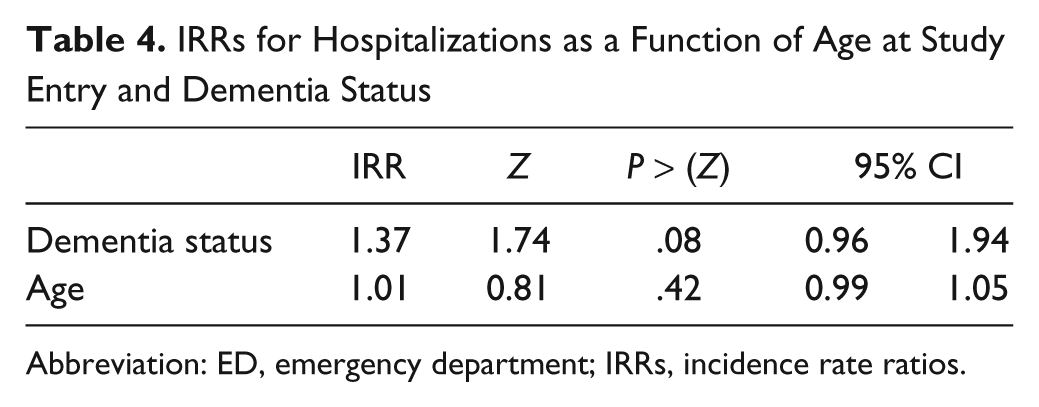
Abbreviation: ED, emergency department; IRRs, incidence rate ratios.
IRRs for Hospitalizations as a Function of Age at Study Entry, Dementia Status, and Medical Burden
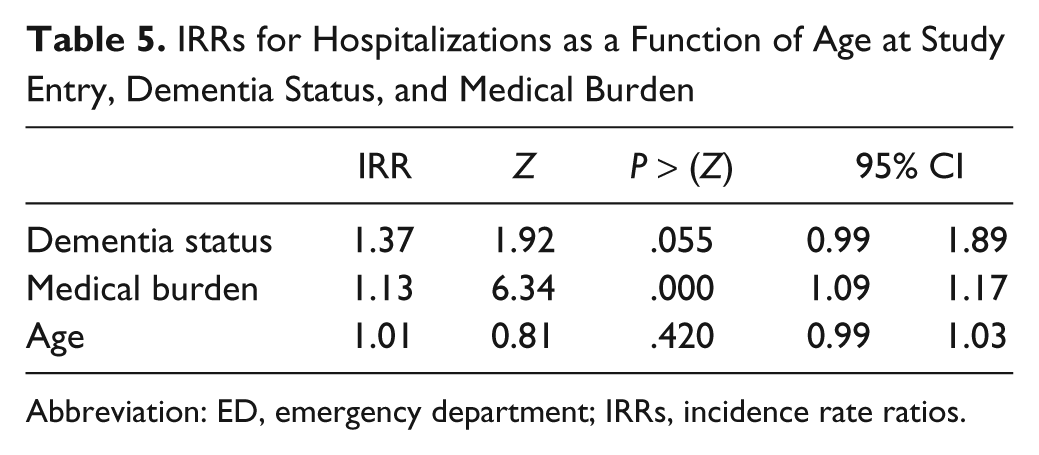
Abbreviation: ED, emergency department; IRRs, incidence rate ratios.
Mortality
Patients with dementia had an 83% higher risk of death than patients without dementia (hazard ratio (HR) = 1.83; 95% CI = 1.05, 3.07). For each 1-point increase of medical burden, the risk of death was 11% higher (HR = 1.11; 95% CI = 1.04-1.17). Functional capacity did not predict death in the full model (not shown).
Discussion
This study differed from most claims based studies because we diagnosed dementia directly by a consensus committee using neuropsychological tests and informant interviews circumventing the problem of under-ascertainment by medical record, assessed comorbidity by comprehensive chart review, and used a medical burden index that takes severity of disease into account. Though the number of dementia cases was small relative to large claims based studies, there was sufficient power to demonstrate that dementia status and medical burden were independent predictors of ED visits and death in this longitudinal cohort of patients from an urban geriatrics clinic. The picture that emerged for hospital admissions was somewhat different. Dementia status by itself did not predict number of admissions, but when adjusted for medical burden, the effect of dementia status was stronger and nearly reached significance (P = .055) in this relatively small sample. Importantly, adjusting for medical burden did not attenuate the association between dementia status, ED visits, and hospitalizations, making it unlikely that measured comorbidities contributed to dementia-related utilization. Functional capacity indexed by the sum of CDR boxes did not predict utilization presumably because of its association with dementia status. Age was not a predictor of utilization.
Our results are consistent with two studies that examined health care costs in the very earliest stages of Alzheimer’s disease. One study of a population-based sample of Medicare enrollees examined the cost of care in the prodromal phase, 1 to 2 years before Alzheimer’s disease was clinically diagnosed. 1 Individuals with incident Alzheimer’s disease were more likely to use outpatient and ambulatory care services during the prodromal phase than adults who did not develop Alzheimer’s disease. The greater use of these services was not due to greater medical burden indexed by the number of comorbidities, suggesting that prodromal Alzheimer’s disease itself may increase the need for medical care. The second study examined the total cost of care (direct medical care, direct nonmedical care, unpaid caregiving) for a large, multicenter cohort of Alzheimer’s disease patients followed from the early stages of the disease. 5 Total cost was higher for patients with dementia and increased with each point of decline in measured activities of daily living.
Our study has several limitations. First, compared to claims based studies, the number of patients with dementia was modest, thus creating a greater possibility that results were due to chance. Second, we cannot be sure that we obtained all comorbidity data though missed comorbidity and missed care would account for our findings only if they were differentially captured by cognitive status, which seems most unlikely. Third, there was insufficient power to examine utilization differences as a function of specific medical comorbidities. Finally, the setting was an urban academic primary care practice staffed by geriatricians who care for many elderly and frail patients. Clinicians and patients in other primary care settings may be different so that the current findings may not predict their utilization patterns.
The increased rates of ED visits and hospitalizations in persons with early stage dementia provide both clinical challenges and opportunities. As the population ages, dementia will become an ever greater challenge and the effects will reverberate throughout the health care delivery system. Opportunity arises from the fact that, at least in part, increased utilization in persons with dementia may be attributable to poor adherence to medical therapy. Strategies to improve medication adherence and disease management have been proposed for elderly patients with and without dementia. 15 Combining them with early detection of cognitive impairment and dementia may provide opportunities to drive down the cost of care. 24
Footnotes
The authors declared no potential conflicts of interests with respect to the authorship and/or publication of this article.
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported in part by grants AG017854 and AG03949 from the National Institutes of Health.