
Abstract
Perceptions of vaccine safety, importance and effectiveness are at the core of vaccine hesitancy around the world, and Africa has had its own share of vaccine revolts. This study uses the 2018 Wellcome Global Monitor on public perceptions of vaccines in 40 African countries to examine the predictors of vaccine hesitancy. It examines levels of hesitancy from a language perspective, comparing French speakers with others, mostly English speakers. Results show that French speakers were significantly more hesitant about importance and safety, while English speakers and others were more hesitant about effectiveness. This reflects the continuing influence of colonial ties on African countries. Respondents with high levels of trust in social actors (such as national government, journalists, people neighborhood, doctors and nurses) were also more hesitant about the safety and effectiveness of vaccines, indicating the importance of non-scientists in influencing vaccine hesitancy. Those with high levels of education were more likely to be hesitant about vaccines in general, indicating that having more education may have an opposite effect. Perception of science as progress was significant for all three hesitancy types, indicating that Africans with more progressive attitudes were less likely to worry about the importance, safety and effectiveness of vaccines. At the country level, there was no overarching predictor, indicating the strong role of local social and cultural factors. These findings improve our understanding of the drivers of vaccine hesitancy in Africa and provide valuable input for future vaccine policy and health-awareness campaigns.
Keywords
Introduction
Resistance to vaccines and anti-vaccination groups both emerged in the late 18th and early 19th centuries because of safety concerns following the introduction of the Jennerian inoculation against smallpox using cowpox. The anti-vaccination groups were formed by the religious community, scientists, journalists and politicians (Colgrove, 2005; Durbach, 2000; Potter and Potter, 1988). The scar from the inoculation was described as the ‘mark of the beast’ and vaccination as an ‘invasion of traditional civil liberties’.
Safety concerns re-emerged in 1974 when severe neurological complications in children were linked with the DTP (diphtheria, tetanus and pertussis) vaccine (Kulenkampff et al., 1974). A link between the MMR (measles, mumps and rubella) vaccine and autism in 1998 sparked another wave of safety concerns (Burgess et al., 2006). More recently, safety concerns over the SARS-CoV-2 (COVID-19) vaccine have been associated with its speed of development and have been seen as a continuation of increasing vaccine hesitancy during the past decade (Verger and Dubé, 2020).
Africa has had its own share of anti-vaccine revolts. State governors in northern Nigeria banned the use of the oral polio vaccine in 2003 following safety concerns during a nationwide vaccination exercise. The vials were rumored to have been contaminated with substances capable of sterilizing women (Falade, 2014). In 1990, in Cameroun, Nigeria's neighbor to the east, young girls leapt from school windows to escape tetanus toxoid vaccination teams, again following concerns that the vaccine would sterilize them (Feldman-Savelsberg et al., 2000). Members of the Apostolic Church in Zimbabwe also expressed fears that vaccines could cause death or disease (Machekanyanga et al., 2017).
This study explores the roles of language, trust, knowledge and attitudes to science in vaccine hesitancy on the African continent with a view to expanding the current body of literature. It explores the roles of trust in science, scientists and social actors as well as knowledge of science and health and the performance of activities that show engagement with science.
Unique to this study is the use of colonial language as a predictor variable. Colonial languages are still used as lingua francas in many African countries, splitting the continent into French and English speakers, alongside less common languages such as Portuguese and Spanish. African countries, since independence, have continued to have cultural, linguistic and economic ties with the former colonizing countries, and this study examines the effect that those ties may have on vaccine hesitancy, given the wide difference in safety concerns between France and the United Kingdom (Karafillakis et al., 2022; Larson et al., 2016). This is an area of research that has not yet been explored in Africa and makes valuable contributions to understanding differences in vaccine hesitancy across the continent.
Vaccines and public health
Vaccines have been praised as one of the great public-health achievements of recent decades (MMWR, 2011). The use of vaccines led to the worldwide eradication of smallpox in 1979, and the world is now closer to eradicating wild poliovirus, confirmed cases of which are now limited to Afghanistan and Pakistan (WHO, 2023a, 2023b). Mortality rates from the COVID-19 pandemic have also been reduced worldwide with the use of vaccines (Eyre et al., 2022; Magazzino et al., 2022). The world is not safe from communicable diseases until they are eradicated worldwide, and the success with smallpox has shown the efficacy of vaccines and of international approaches to public health. Vaccine hesitancy, described as a delay in acceptance or refusal of vaccination, or acceptance with doubts about its safety and benefits, remains a threat to global health campaigns (Larson et al., 2014).
There is, however, no ‘perfect’ vaccine that protects everyone who receives it and is entirely safe for everyone (WHO, 2021a). Among other adverse events, the World Health Organization (WHO) lists the risk of anaphylaxis from the anthrax vaccine as 0.76 per 100,000; the risk of immune reconstitution syndrome from the tuberculosis vaccine BCG (Bacillus Calmette-Guérin) as 1 per 640,000; and the risk of vaccine-associated paralysis from the oral polio vaccine as 1 per 2.9 million doses (WHO, 2021b). Following the introduction of the COVID-19 vaccine, vaccine adverse event reporting systems were set up by some countries (CDC, 2022; DHAC, 2022; MHRA, 2021). Some of the adverse events reported after COVID-19 vaccination were categorized by CDC (the Centers for Disease Control and Prevention of the United States) as anaphylaxis, reports of deaths, Guillain-Barré syndrome, myocarditis and pericarditis, and thrombosis with thrombocytopenia syndrome. Others include minor reactions such as headaches, fever, fatigue and joint or muscle pains.
While progress has been made in addressing some of the rare, but serious, side effects, increasing concerns have created an ever-growing number of anti-vaccine groups, further driving media and public anxieties over a range of disorders linked to vaccines (Poland and Jacobson, 2011; Swales, 1992). Vaccine behaviors, however, form a continuum ranging from active demand for vaccines to complete refusal of all vaccines rather than a dichotomous pro- versus anti-vaccination perspective. Between these extremes are those who may accept some vaccines and reject others (Dubé et al., 2015).
Trust in science and vaccines
Trust is based on social relations (Earle et al., 2007; Siegrist, 2010) and is both at the origin and the limit of social knowledge (Moscovici, 2001). A public that cannot understand what science says must trust, as that compensates for deficiencies at a cognitive level (Neidhart, 1993). Reliance on trust in science and scientists is a dominant heuristic in reaching judgements, and it is only where societal leaders effectively redefine an area of science as in conflict with something else that controversy arises (Brossard and Nisbet, 2007; Nisbet and Scheufele, 2009). Anderson et al. (2012) found that deference to scientific authority and specific technological knowledge are important in science, society and trust relationships.
Hendriks et al. (2016) argue that trust is pivotal for scientists just as it is fundamental for public understanding of science. Since laypeople are now able to rapidly access all kinds of scientific knowledge online but still have to trust scientists, that trust relationship also entails a vigilance towards the risk of being misinformed. Weingart and Guenther (2016) argue that science communication, whether among scientists or with the public, depends on trust, both in the source and in the medium of communication. Trust, the authors argue, is endangered by the new ‘ecology of communication’ because science communication by scientists is tainted by special interests, and the channels used to communicate, such as social media, could raise doubts about the credibility of the communication spread through them.
Larson et al. (2018) define trust in health care as a relationship that exists between individuals, as well as between individuals and a system, in which one party accepts a vulnerable position, assuming the benevolent interest and competence of the other, in exchange for a reduction in decision complexity. Vaccine acceptance, the authors argue, involves multiple levels of trust in the product, health-care professionals, policymakers and public-health researchers. Trust in vaccine information, they argue further, also involves multiple levels: the information itself, those who produce it and those who propagate it. Its perception is subjective. When communicating about vaccines specifically, Ozawa and Stack (2013) argue that the public's trust in the information source, the mode of communication and the consistency of messages should be carefully considered as building and sustaining trust, as well as measuring and monitoring levels of trust. These factors, they suggest, could hold the key to bridging the vaccine confidence gap.
Perceptions of the safety, importance and efficiency of vaccines
This study examines African people's perceptions of the importance, safety and effectiveness of vaccines, focusing on the roles of language, trust and other psychosocial and economic predictors. In Nigeria, which is part of anglophone West Africa, party politics and declining trust in Western countries (the donors of the oral polio vaccine) played significant roles in vaccine hesitancy (Falade, 2014). In Cameroun, which is part of francophone West Africa, members of the pro-life Catholic movement were prominent actors, and opposition politicians described the vaccine as a government plot to politically disadvantage some provinces (Feldman-Savelsberg et al., 2000). Safety concerns led to similar revolts in Uganda, Tanzania and Kenya (Clements and Drake, 2002). In Zimbabwe, greater trust in religious teachings that emphasize the power of prayers over science contributed to hesitancy.
The effect of the language of communication has been neglected in past studies of vaccine hesitancy in Africa. While African countries are multilingual, the official language for politics, educational curriculums and books is largely French or English (some countries have adopted two or more official languages). While anglophone countries have developed their own currencies independent of the United Kingdom, the francophone currencies and economy remain tied to France, and, some will argue, so is much of their politics, health-care and other systems. The languages of the media of communication in these blocs also remain French and English, and traditional media are tuned to either the BBC and CNN or AFP for foreign news. People are also more likely to connect to social-media platforms, which are now a major source of health news in languages they understand (Kata, 2012; Witteman and Zikmund-Fisher, 2012). Cultural, linguistic and economic ties may have a role in vaccine hesitancy in Africa, given the wide difference in safety concerns between France and the United Kingdom (Karafillakis et al., 2022; Larson et al., 2016).
In a Dutch study, Harmsen et al. (2013) found that hesitancy was related to multiple factors, including family lifestyle; parental perceptions about the body and the immune system of the child; perceived risks of disease; vaccine efficacy and side effects; perceived advantages of experiencing the disease; prior negative experiences with vaccination; and the social environment. Vaccines may also be resisted because of religion, pain and cost (Lyren and Leonard, 2006). Another major concern is the perception of risk that may arise from the use of preservatives such as mercury and adjuvants such as aluminium. Scientists are, however, divided on this associated risk (Ball et al., 2001; Crespo-López et al., 2009).
Scientific authorities in the medical field also have reservations about the safety and efficacy of vaccines. In a review of research focused on vaccine hesitancy among nurses and physicians, Ahmad et al. (2022) found that hesitancy among them stemmed predominantly from distrust in vaccine efficacy and safety and mistrust of pharmaceutical companies. In a review of attitudes towards vaccination in Europe, Yaqub et al. (2014) found that those attitudes were shaped not just by health-care professionals but also by an array of other information sources, including online and social-media sources.
Perception of risk has also been blamed for vaccine hesitancy among doctors. A French study found that general practitioners (GPs) recommended vaccines when they felt comfortable with explaining their benefits and risks to patients or trusted official sources of information (Verger et al., 2015). Another French study of 1582 GPs by Le Marechal et al. (2018) found that most of GPs’ perceptions of serious adverse effects were not based on scientific evidence. French surveys have reported one of the highest rates of vaccine hesitancy in the world, at between 25% and 70% (Ward et al., 2019). Bocquier et al.'s (2018) analysis of the 2016 Baromètre santé (a random cross-sectional telephone survey of the French general population) showed that 26% of parents were vaccine refusers, 7% were delayers and 13% were acceptors with doubts.
Ozawa and Stack (2013) argue that public trust can be built by helping all stakeholders, including parents, health practitioners, community leaders, policymakers and the media, to recognize the value of vaccines within unique social, cultural and political contexts. They also argue that information should be transparent in presenting both the risks and benefits of vaccines.
Anti-vaccination movements: Same message, new media
While the functions of anti-vaccine movements have remained the same across the decades, their campaign strategies have evolved alongside developments in the media. Before the advent of the internet, campaigns were through pamphlets, books, newspapers, magazines and journals. The internet moved debates online, and social media are now important sources of information; health news is increasingly sought from online news groups and blogs rather than official vaccine information sites (Kata, 2012; Witteman and Zikmund-Fisher, 2012).
Social-media platforms such as Twitter (now X) and Reddit were used by parents in the United States and United Kingdom as top resources during the vaccine‒autism controversy (Jang et al., 2019). An analysis of Twitter during the 2015 measles outbreak in California in the United States found that messages of interest to parents about measles were news updates, personal opinions, personal experiences, susceptibility, cues to action and severity (Meadows et al., 2019). Wilson and Wiysonge (2020) found a significant relationship between organized activities on social media and public doubts about vaccine safety. They also found a substantial relationship between foreign anti-vaccination campaigns and declining vaccine coverage. Osur et al. (2022) found that social media remained an important source of vaccine information in Africa contributing to vaccine hesitancy among Kenyans.
Despite safer and more effective vaccines and enhanced surveillance of adverse effects, vaccine hesitancy remains underpinned by the same reasons as centuries ago: perceptions of vaccines’ safety, effectiveness and relative importance over other treatment options, such as natural immunity. The activities of anti-vaccine movements have, however, expanded to online forums, contributing to vaccine hesitancy and declining vaccine coverage. Unlike the anti-vaccination leagues of the 1880s, however, more recent campaigns have adopted neutral names, such as Vaccination News and The National Vaccine Information Centre (intended to sound authoritative) and have been implicated in lowered vaccine acceptance rates and increases in vaccine-preventable disease outbreaks (Dubé et al., 2015; Kirkland, 2012).
Research objectives
Safety concerns in Cameroun (Feldman-Savelsberg et al., 2000), Nigeria (Falade, 2014), Uganda, Kenya, Tanzania (Clements and Drake, 2002) and Zimbabwe (Machekanyanga et al., 2017) have led to vaccine revolts. Safety and other concerns have also arisen with the introduction of the COVID-19 vaccine in Africa (Ajeigbe et al., 2022; Cooper et al., 2021; Ekwebelem et al., 2021). Anti-vaccination campaigns, spread by social media, have been associated with declining vaccine coverage (Wilson and Wiysonge, 2020) and have contributed to vaccine hesitancy in Kenya (Osur et al., 2022).
The Wellcome Global Monitor 2018 explored public perceptions of the safety, importance and efficacy of vaccines and trust in science and society. The survey predated the COVID-19 pandemic and offered insights into public perceptions before the crisis. No comparable worldwide surveys have been undertaken since this Wellcome Trust report. Research questions in this study have evolved from themes in the 2018 survey and also examined the influence of shared language within Africa and with colonial masters. The aim of this study is to widen the knowledge base and address the need for country-specific and/or regional predictors of hesitancy in Africa. The research questions are:
Data and research methods
This study examines vaccine hesitancy in 40 African countries in the Wellcome Global Monitor 2018. The francophone countries in the sample (22) were Morocco, Benin, Madagascar, Mali, Mauritania, Niger, Rwanda, Senegal, Burkina Faso, Cameroon, Algeria, Burundi, Chad, Comoros, the Democratic Republic of the Congo (DR Congo), Gabon, Guinea, Ivory Coast, Mauritius, The Gambia, Togo and Tunisia. The others, mostly English speaking (18), were Egypt, Nigeria, Kenya, Tanzania, Ghana, Uganda, Malawi, South Africa, Botswana, Ethiopia, Mozambique, Zambia, Sierra Leone, Zimbabwe, Liberia, Libya, Namibia and Eswatini.
Twelve countries (Chad, Morocco, DR Congo, Mali, Algeria, Gabon, Tanzania, Kenya, Ghana, Nigeria, Zambia and South Africa) were selected to compare frequencies and measurement invariance. The first six countries are French-speaking, while the others are English-speaking. They were selected from the North, West, Central and Southern Africa regions.
Response variables
Q24. Vaccines are important. Q25. Vaccines are safe. Q26. Vaccines are effective.
The answer options were recoded to a binary: acceptance (strongly agree and somewhat agree) and hesitancy (neither agree nor disagree, somewhat disagree, strongly disagree and don’t know/refuse). Given the definition of hesitancy as including acceptance with doubts, somewhat agree was considered hesitancy, but the author was of the view that this was too restrictive and opted to categorize it as acceptance.
Predictor variables
Demographics: age, gender, education, income and area type (rural versus urban). A binary variable was created for language: French and others (mostly English).
Trust variables
Q11. How much do you trust each of the following: Q11A. The people in your neighborhood. Q11B. The national government in this country. Q11C. Scientists in this country. Q11D. Journalists in this country. Q11E. Doctors and nurses in this country. Q11F. People who work for charitable organizations/NGOs. Q11G. Traditional healers. Q12. In general, would you say that you trust science? Q13. In general, how much do you trust scientists to find out accurate information about the world? Q14A. How much do you trust scientists working in colleges/universities in this country to do their work with the intention of benefiting the public? Q14B. How much do you trust scientists working in colleges/universities in this country to be open and honest about who is paying for their work? Q15A. How much do you trust scientists working for companies in this country to do their work with the intention of benefiting the public? Q15B. How much do you trust scientists working for companies in this country to be open and honest about who is paying for their work?
Progress, engagement and knowledge
The PREK (progress, reserve, engagement and knowledge) model was adopted from Bauer and Suerdem (2016). Reserve was the response variable and so was not used as an explanatory variable.
The summative scales for progress were:
Q17. Do you think the work that scientists do benefits people like you in this country? Q18. Do you think that science and technology will help improve life for the next generation? Q19. Do you think that science and technology will increase or decrease the number of jobs in your local area in the next five years? Q16(1). Do you think the work that scientists do benefits most, some or very few people in this country?
The summative scales for engagement (information-seeking) were:
Q6. Have you, personally, tried to get any information about science in the past 30 days? Q7. Have you, personally, tried to get any information about medicine, disease or health in the past 30 days? Q8. Would you, personally, like to know more about science? Q9(1). Would you, personally, like to know more about medicine, disease or health?
The summative scales for knowledge were:
Q1. How much do you, personally, know about science? Q2. How much did you understand the meaning of ‘science’ and ‘scientists’ that was just read? Q5A. Have you, personally, ever, learned about science at primary school? Q5B. Have you, personally, ever, learned about science at secondary school? Q5C. Have you, personally, ever, learned about science at college/university? Q23(1). Before today, had you ever heard of a vaccine?
Factor analysis and multigroup confirmatory factor analysis
Factor analysis was used to reduce the responses from the 13 trust questions to latent variables (Bartholomew et al., 2008; Field, 2005). Multigroup confirmatory factor analysis (MGCFA), an extension of confirmatory factor analysis, was used to test measurement invariance—that the same underlying construct was being measured in the data set, using gender as the group variable. Models ensured that increased reliability was not achieved at the expense of construct validity, and goodness-of-fit indexes were in acceptable ranges (Bialosiewicz et al., 2013; Kim et al., 2017).
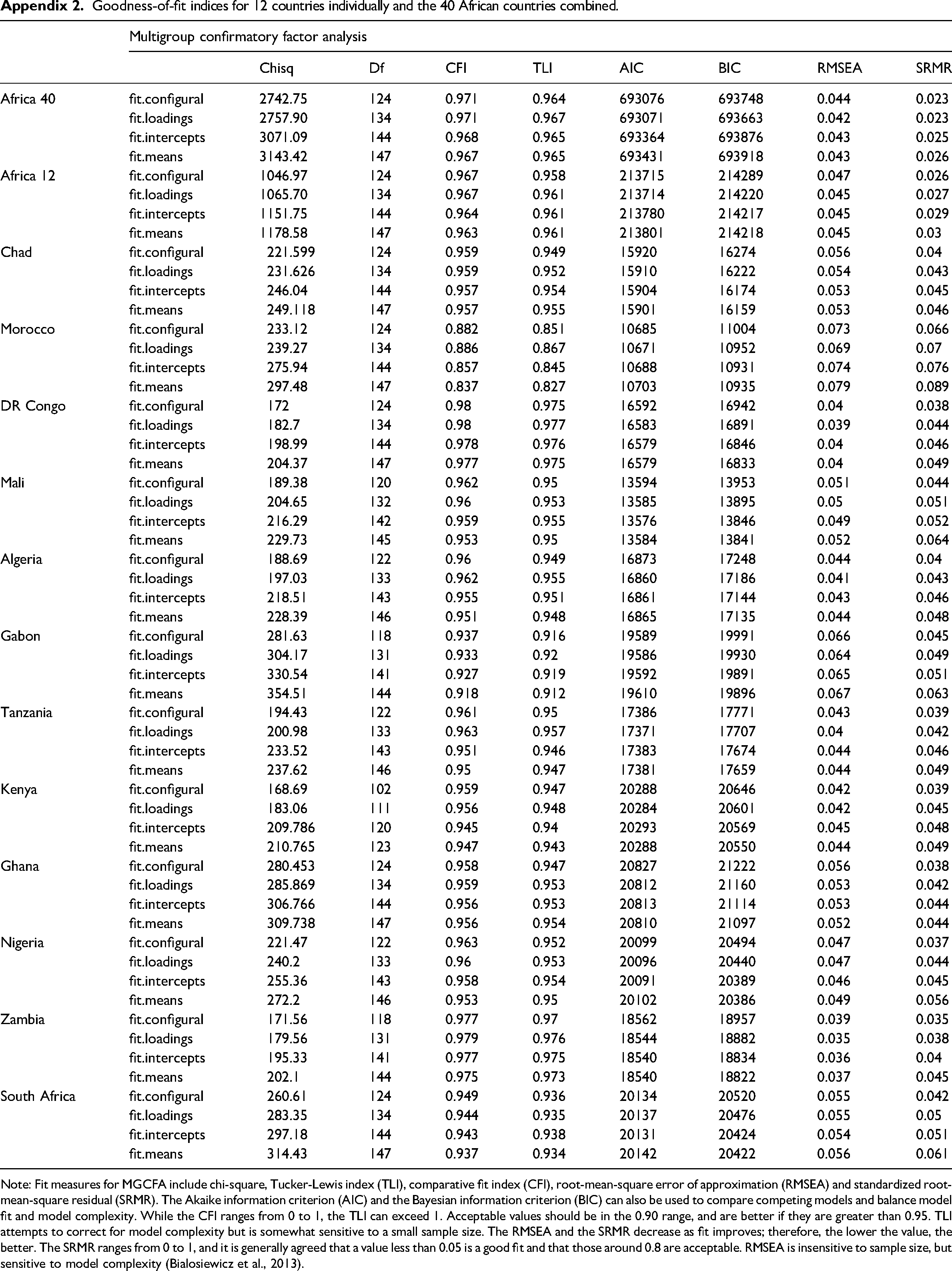
For factor analysis, the author examined and reported Cronbach's alpha, percentage of variance explained, chi-square, the Kaiser-Meyer-Olkin measure of sampling adequacy and Bartlett's test of sphericity (Appendix 1). For MGCFA, the author examined and reported configural, metric and scalar invariance (Appendix 2) using the chi-square statistic, comparative fit index (CFI), the Tucker-Lewis index (TLI), the root-mean-squared error of approximation (RMSEA), the standardized root-mean-squared residual (SRMR), the Akaike information criterion (AIC) and Bayesian information criterion (BIC).
A three-factor solution best described the trust variables across countries, which were named trust in social actors, trust in scientific research and trust in science and scientists (Appendix 1). The percentage of variance explained by factors, factor loadings and factor position varied between countries, and few cross-loadings were observed. Loadings for trust in traditional healers were below 0.2 for South Africa and Tanzania but acceptable for the sample size (Field, 2005: 637)
Analysis and findings
French surveys reported vaccine hesitancy at between 25% and 70% (Ward et al., 2019). The Wellcome Global Monitor 2018 survey showed 49% for hesitancy about safety, 28% for effectiveness and 20% for importance for France compared with 23%, 13% and 10% for the United Kingdom. Figure 1 shows that the francophone countries mirrored France, with higher levels of hesitancy about safety compared with the United Kingdom and the anglophone countries.
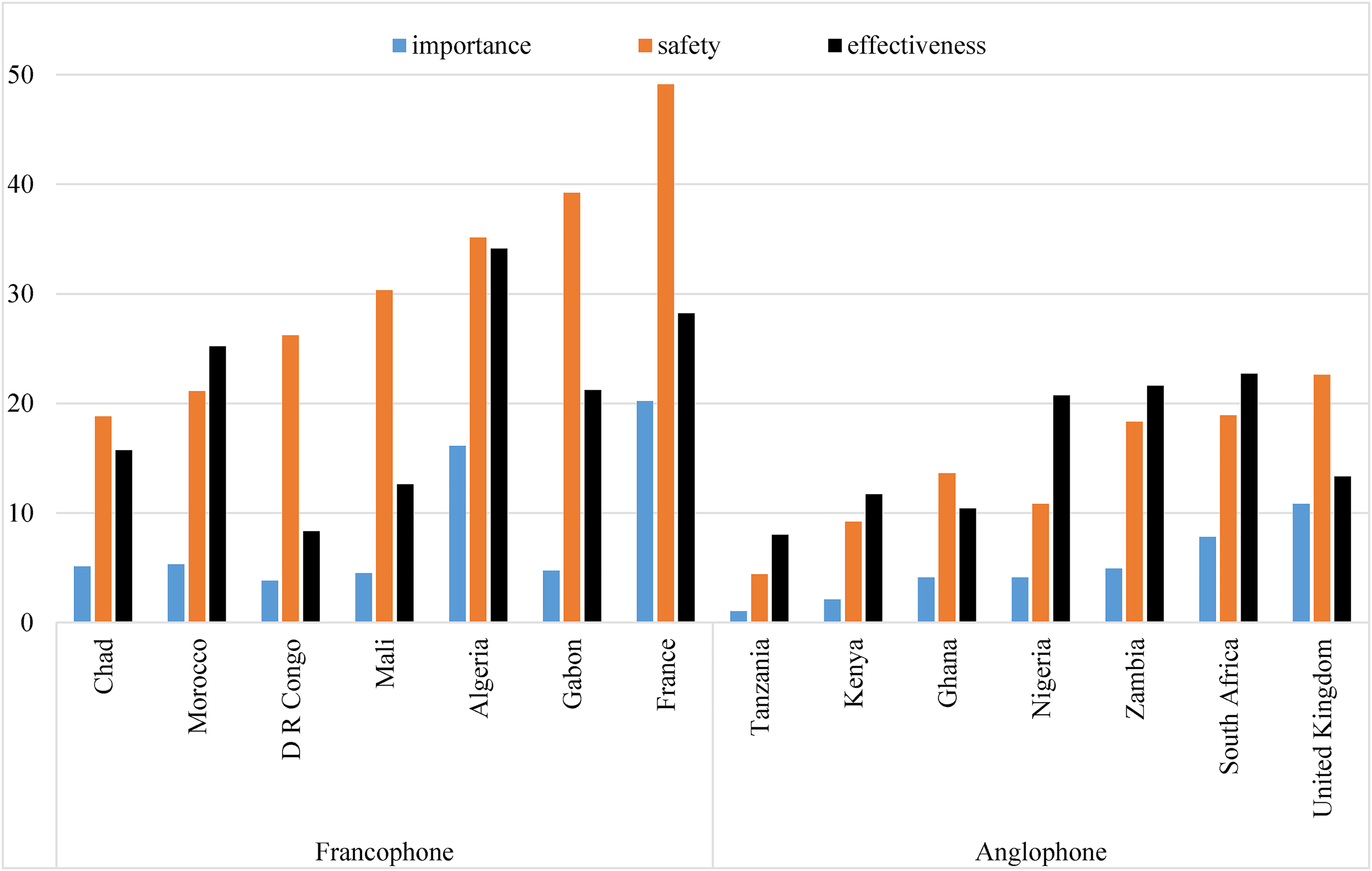
Vaccine hesitancy (neither agree nor disagree, somewhat disagree, strongly disagree and don’t know/refuse) in six francophone and six anglophone African countries compared with France and the United Kingdom.
The highest level of hesitancy about safety for the francophone countries was Gabon (39.2%) and the lowest was Chad (18.8%). The highest for the anglophone countries was South Africa (18.9%) and the lowest was Tanzania (4.4%). Levels of hesitancy about safety from the two countries from Southern Africa, Zambia and South Africa, were higher than for other English-speaking countries and just below the level in Morocco.
Hesitancy about effectiveness in Algeria was higher than in France. France was, however, higher in this form of hesitancy than other francophone countries. Levels for Nigeria, Zambia and South Africa were similar to that for Gabon and higher than those for Chad, DR Congo and Mali.
Hesitancy about importance was highest in Algeria among the African nations but lower than in France. The highest level among the English-speaking countries was in South Africa, followed by Zambia. Tanzania and Kenya had the lowest hesitancy about vaccine importance of all the 12 African countries.
For this question, the author used the data for 40 countries. The response variables used were Q24. Vaccines are important; Q25. Vaccines are safe; and Q26. Vaccines are effective. The explanatory variables were language (English or French); demographics (age, gender, education, income and area type); the three latent trust factors (trust in social actors, trust in scientific research and trust in science and scientists); and the summative scales of progress, engagement and knowledge. The trust latent factors were converted to binary/dummy variables using the visual binning function of SPSS to select the top 33.3% (1) against the rest (0).
The hesitancy averages for the 40 African countries in the Wellcome Global Monitor 2018 were: importance 4.3%, safety 18.7% and effectiveness 15.5%. The averages for the 22 francophone countries were: importance 5.2%, safety 24.3% and effectiveness 15.7%, and for the anglophone countries were: importance 3.1%, safety 11.6% and effectiveness 15.2%. The average for francophone countries on safety was double that of anglophone countries, and the average on importance was also around double, indicating a strong influence of the colonial or francophone effect.
Table 1 shows that French speakers were more hesitant about vaccine importance and safety, while English speakers and others were more hesitant about effectiveness. Additionally, those who lived in urban areas were significantly more hesitant about vaccine importance and effectiveness.
Logistic regression output for language and other predictors of hesitancy about the importance, safety and effectiveness of vaccines in 40 African countries.
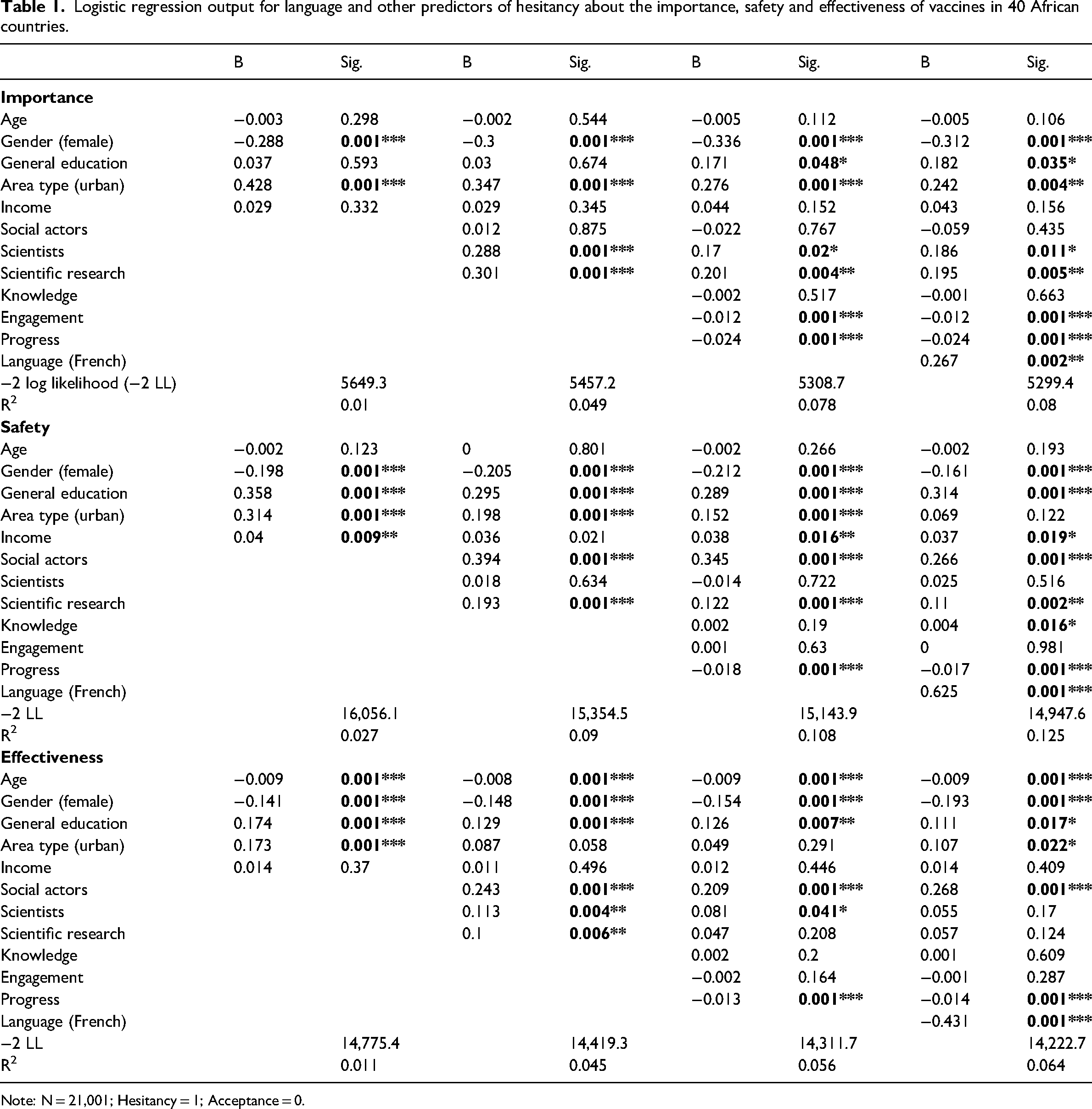
Note: N = 21,001; Hesitancy = 1; Acceptance = 0.
The positive association of high levels of trust in scientific research with vaccine importance and safety indicates that more trust led to more hesitancy, which was not the case for effectiveness. Trust in scientists was significant only for hesitancy about vaccine importance. Trust in social actors was important for hesitancy about vaccine safety and effectiveness but not for importance.
General education and gender were significant across all three hesitancy variables, but the association with gender was negative, showing that men were more hesitant than women. Younger people were significantly more hesitant about vaccine effectiveness but not about safety and importance.
Perceptions of science as progress were very significant for all three hesitancy types. The negative relationships indicate that Africans with more progressive attitudes were less likely to worry about the importance, safety and effectiveness of vaccines. The significant but negative beta for engagement (information-seeking) for hesitancy about importance also indicates that higher levels of engagement led to less hesitancy about vaccine importance.
The explanatory and response variables were the same as for the 40 countries: demographics (age, gender, education, income and area type); the three latent trust factors (trust in social actors, trust in scientific research and trust in science and scientists); and the summative scales of progress, engagement and knowledge.
Logistic regression output for hesitancy about importance of vaccines.
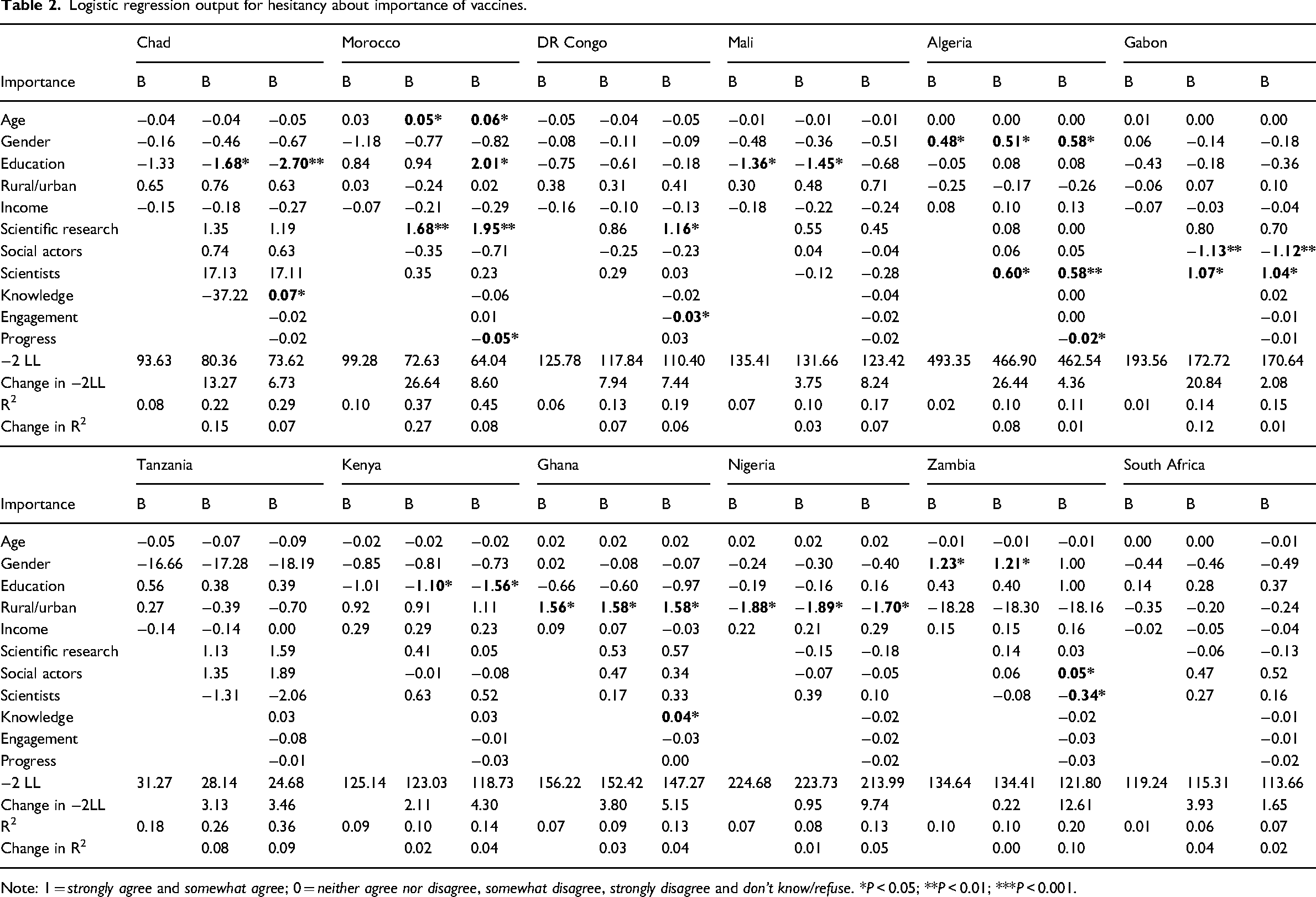
Note: 1 = strongly agree and somewhat agree; 0 = neither agree nor disagree, somewhat disagree, strongly disagree and don’t know/refuse. *P < 0.05; **P < 0.01; ***P < 0.001.
Logistic regression output for hesitancy about safety of vaccines.
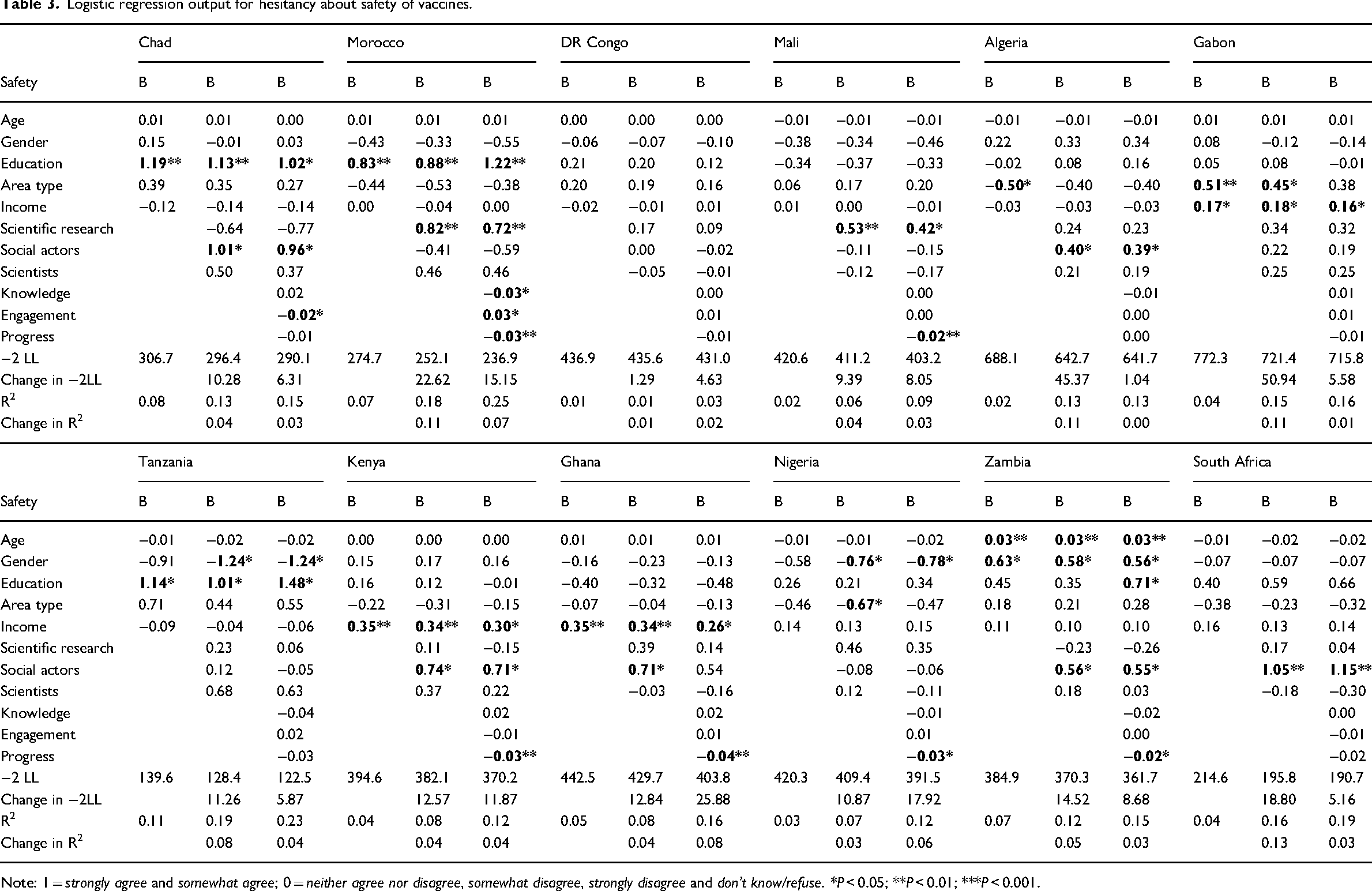
Note: 1 = strongly agree and somewhat agree; 0 = neither agree nor disagree, somewhat disagree, strongly disagree and don’t know/refuse. *P < 0.05; **P < 0.01; ***P < 0.001.
Logistic regression output for hesitancy about effectiveness of vaccines.
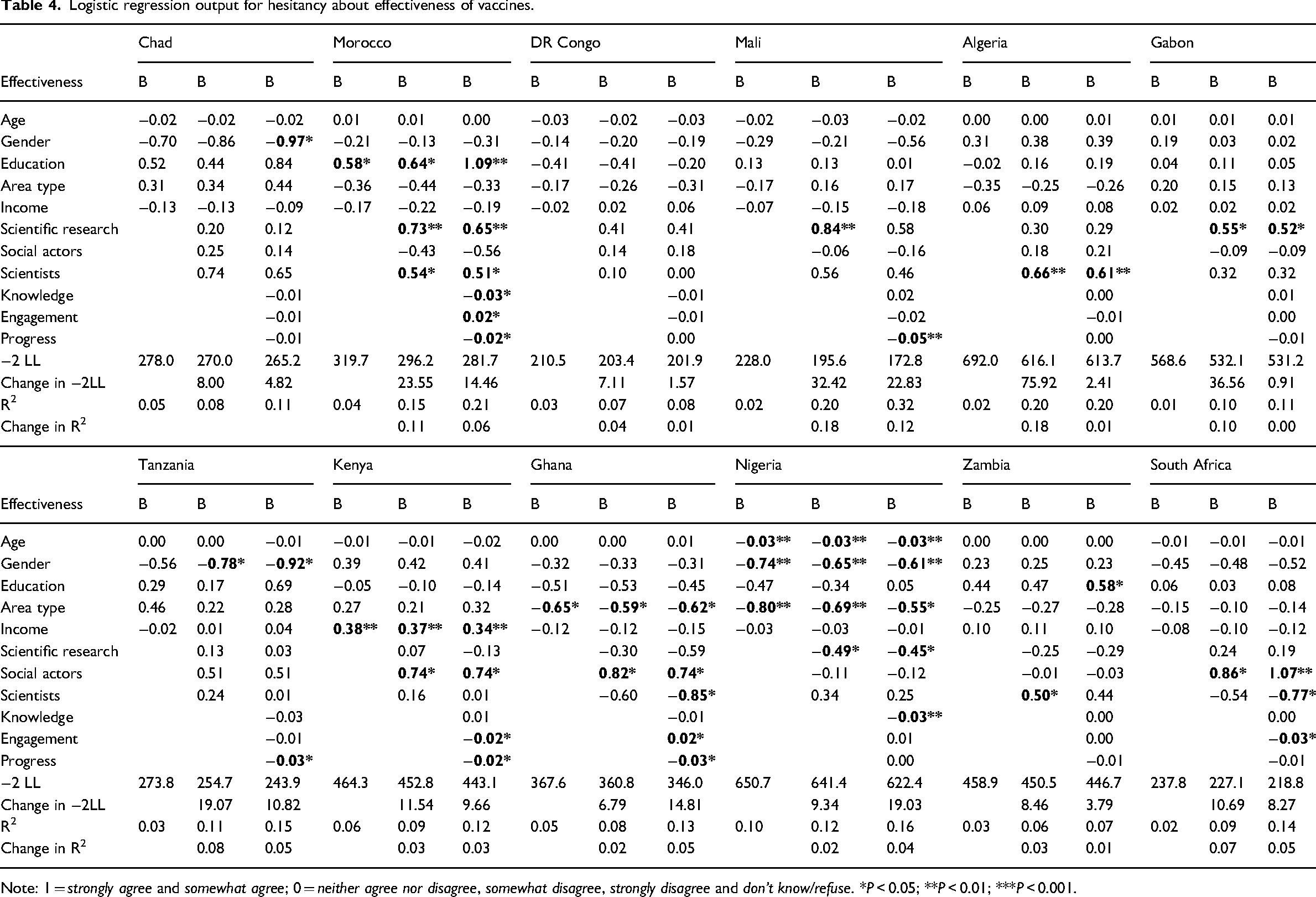
Note: 1 = strongly agree and somewhat agree; 0 = neither agree nor disagree, somewhat disagree, strongly disagree and don’t know/refuse. *P < 0.05; **P < 0.01; ***P < 0.001.
The hesitancy about vaccine safety average for the 22 francophone countries was more than double the average for the 18 anglophone countries. Hesitancy about vaccine importance for francophone countries was also almost double that for English speakers. These differences mirror that observed between the United Kingdom and France, splitting Africa along colonial lines, and are thus strong indicators of the colonial or francophone effect. This division on vaccine hesitancy plausibly reflects the strong role of a continued sharing of language, education and cultural ties with former colonies. Shared communication is also more readily accessible through social media with expanding internet access, its popularity and reach. Language restricts African people to news and public debates from French- or English-speaking media, and this has become even more important as health news is increasingly sought from online groups, blogs and social-media apps rather than from official vaccine information sites.
Comparing where the respondents reside, this study found that people in urban areas, who are more likely to have internet access, were more hesitant about vaccine importance and effectiveness than those in rural areas, who, in Africa, are largely farmers and less likely to have internet access.
With trust in institutions, those who had higher levels of trust in social actors (such as national government, journalists, people neighborhood, doctors and nurses) were more hesitant about the safety and effectiveness of vaccines, but not their importance. Thus, social actors play a strong role in public perceptions of safety and effectiveness. Social actors are more likely to be found in the media, on unofficial vaccine information sites and in everyday social communications, so these findings expand our understanding of the importance of non-scientific actors in vaccine hesitancy.
With scientific actors, higher levels of trust in scientific research led to more hesitancy about the importance and safety but not the effectiveness of vaccines. Trust in scientists was significant only for hesitancy about importance. An increasing level of general education was also significantly associated with all three hesitancy variables. These findings suggest that the expectation that ‘the more people know about science, the more they love it’ may not always be met and, in fact, may have an opposite effect with regard to vaccine hesitancy. This study found, however, that Africans in the sample population who saw science as progress and as benefiting the public and improving lives were less likely to be hesitant about the importance, safety and effectiveness of vaccines.
At the country level, the significance of variables as predictors varied, and there was no overarching predictor for all 12 countries, which may indicate the strong role of local social and cultural factors. For Nigeria and Ghana, both in West Africa, rural versus urban living was important for perceptions of the effectiveness and the importance of vaccines. On safety, income was important for Ghana and Kenya. The level of general education was important for Chad and Morocco. Gender was important for Nigeria, Tanzania and Zambia.
This research has shown the role of continent-wide and country-level predictors for all three types of vaccine hesitancy and will be valuable for informing future public-health policies and communication campaigns, even beyond vaccines. Health policies and campaigns need to recognize continent-wide similarities, the potential impact of language differences and country-level cultural differences for successful implementation and outcomes. It is also important to keep a longitudinal data stream as part of a monitoring and evaluation process to guide the content of communication campaigns and the direction of further policy. More research is needed on the relationship between language and vaccine hesitancy, in particular the role of the media in public perceptions.
The data for this study was collected a year before the COVID-19 pandemic and the subsequent introduction of COVID-19 vaccines. While this can be seen as a limitation, it is also an advantage in that it provides baseline data for future comparisons.
Footnotes
Acknowledgements
The author would like to thank colleagues in the MACAS (Mapping the Cultural Authority of Science) group for insightful comments during the research process: Dr Petra Pansegrau of the University of Bielefeld, Germany; Professor Martin Bauer of the London School of Economics and Political Science, United Kingdom; Professor Ahmet Suerdem of Istanbul Bilgi University, Turkey; and Professor Carmelo Polino of the University of Oviedo, Spain. Appreciation also goes to Professor Johann Mouton, director of the DSI-NRF Centre of Excellence for Scientometrics and STI Policy and professor at the Centre for Research on Evaluation, Science and Technology (CREST), Stellenbosch University, South Africa.
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Author biography
Bankole Falade is a research officer at the Department of Psychological and Behavioural Sciences, London School of Economics and Political Science, United Kingdom. His research interests are in cross-cultural psychology, science and health communication, text analysis and research methods.
Appendices
Goodness-of-fit indices for 12 countries individually and the 40 African countries combined.
| Multigroup confirmatory factor analysis | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Chisq | Df | CFI | TLI | AIC | BIC | RMSEA | SRMR | ||
| Africa 40 | fit.configural | 2742.75 | 124 | 0.971 | 0.964 | 693076 | 693748 | 0.044 | 0.023 |
| fit.loadings | 2757.90 | 134 | 0.971 | 0.967 | 693071 | 693663 | 0.042 | 0.023 | |
| fit.intercepts | 3071.09 | 144 | 0.968 | 0.965 | 693364 | 693876 | 0.043 | 0.025 | |
| fit.means | 3143.42 | 147 | 0.967 | 0.965 | 693431 | 693918 | 0.043 | 0.026 | |
| Africa 12 | fit.configural | 1046.97 | 124 | 0.967 | 0.958 | 213715 | 214289 | 0.047 | 0.026 |
| fit.loadings | 1065.70 | 134 | 0.967 | 0.961 | 213714 | 214220 | 0.045 | 0.027 | |
| fit.intercepts | 1151.75 | 144 | 0.964 | 0.961 | 213780 | 214217 | 0.045 | 0.029 | |
| fit.means | 1178.58 | 147 | 0.963 | 0.961 | 213801 | 214218 | 0.045 | 0.03 | |
| Chad | fit.configural | 221.599 | 124 | 0.959 | 0.949 | 15920 | 16274 | 0.056 | 0.04 |
| fit.loadings | 231.626 | 134 | 0.959 | 0.952 | 15910 | 16222 | 0.054 | 0.043 | |
| fit.intercepts | 246.04 | 144 | 0.957 | 0.954 | 15904 | 16174 | 0.053 | 0.045 | |
| fit.means | 249.118 | 147 | 0.957 | 0.955 | 15901 | 16159 | 0.053 | 0.046 | |
| Morocco | fit.configural | 233.12 | 124 | 0.882 | 0.851 | 10685 | 11004 | 0.073 | 0.066 |
| fit.loadings | 239.27 | 134 | 0.886 | 0.867 | 10671 | 10952 | 0.069 | 0.07 | |
| fit.intercepts | 275.94 | 144 | 0.857 | 0.845 | 10688 | 10931 | 0.074 | 0.076 | |
| fit.means | 297.48 | 147 | 0.837 | 0.827 | 10703 | 10935 | 0.079 | 0.089 | |
| DR Congo | fit.configural | 172 | 124 | 0.98 | 0.975 | 16592 | 16942 | 0.04 | 0.038 |
| fit.loadings | 182.7 | 134 | 0.98 | 0.977 | 16583 | 16891 | 0.039 | 0.044 | |
| fit.intercepts | 198.99 | 144 | 0.978 | 0.976 | 16579 | 16846 | 0.04 | 0.046 | |
| fit.means | 204.37 | 147 | 0.977 | 0.975 | 16579 | 16833 | 0.04 | 0.049 | |
| Mali | fit.configural | 189.38 | 120 | 0.962 | 0.95 | 13594 | 13953 | 0.051 | 0.044 |
| fit.loadings | 204.65 | 132 | 0.96 | 0.953 | 13585 | 13895 | 0.05 | 0.051 | |
| fit.intercepts | 216.29 | 142 | 0.959 | 0.955 | 13576 | 13846 | 0.049 | 0.052 | |
| fit.means | 229.73 | 145 | 0.953 | 0.95 | 13584 | 13841 | 0.052 | 0.064 | |
| Algeria | fit.configural | 188.69 | 122 | 0.96 | 0.949 | 16873 | 17248 | 0.044 | 0.04 |
| fit.loadings | 197.03 | 133 | 0.962 | 0.955 | 16860 | 17186 | 0.041 | 0.043 | |
| fit.intercepts | 218.51 | 143 | 0.955 | 0.951 | 16861 | 17144 | 0.043 | 0.046 | |
| fit.means | 228.39 | 146 | 0.951 | 0.948 | 16865 | 17135 | 0.044 | 0.048 | |
| Gabon | fit.configural | 281.63 | 118 | 0.937 | 0.916 | 19589 | 19991 | 0.066 | 0.045 |
| fit.loadings | 304.17 | 131 | 0.933 | 0.92 | 19586 | 19930 | 0.064 | 0.049 | |
| fit.intercepts | 330.54 | 141 | 0.927 | 0.919 | 19592 | 19891 | 0.065 | 0.051 | |
| fit.means | 354.51 | 144 | 0.918 | 0.912 | 19610 | 19896 | 0.067 | 0.063 | |
| Tanzania | fit.configural | 194.43 | 122 | 0.961 | 0.95 | 17386 | 17771 | 0.043 | 0.039 |
| fit.loadings | 200.98 | 133 | 0.963 | 0.957 | 17371 | 17707 | 0.04 | 0.042 | |
| fit.intercepts | 233.52 | 143 | 0.951 | 0.946 | 17383 | 17674 | 0.044 | 0.046 | |
| fit.means | 237.62 | 146 | 0.95 | 0.947 | 17381 | 17659 | 0.044 | 0.049 | |
| Kenya | fit.configural | 168.69 | 102 | 0.959 | 0.947 | 20288 | 20646 | 0.042 | 0.039 |
| fit.loadings | 183.06 | 111 | 0.956 | 0.948 | 20284 | 20601 | 0.042 | 0.045 | |
| fit.intercepts | 209.786 | 120 | 0.945 | 0.94 | 20293 | 20569 | 0.045 | 0.048 | |
| fit.means | 210.765 | 123 | 0.947 | 0.943 | 20288 | 20550 | 0.044 | 0.049 | |
| Ghana | fit.configural | 280.453 | 124 | 0.958 | 0.947 | 20827 | 21222 | 0.056 | 0.038 |
| fit.loadings | 285.869 | 134 | 0.959 | 0.953 | 20812 | 21160 | 0.053 | 0.042 | |
| fit.intercepts | 306.766 | 144 | 0.956 | 0.953 | 20813 | 21114 | 0.053 | 0.044 | |
| fit.means | 309.738 | 147 | 0.956 | 0.954 | 20810 | 21097 | 0.052 | 0.044 | |
| Nigeria | fit.configural | 221.47 | 122 | 0.963 | 0.952 | 20099 | 20494 | 0.047 | 0.037 |
| fit.loadings | 240.2 | 133 | 0.96 | 0.953 | 20096 | 20440 | 0.047 | 0.044 | |
| fit.intercepts | 255.36 | 143 | 0.958 | 0.954 | 20091 | 20389 | 0.046 | 0.045 | |
| fit.means | 272.2 | 146 | 0.953 | 0.95 | 20102 | 20386 | 0.049 | 0.056 | |
| Zambia | fit.configural | 171.56 | 118 | 0.977 | 0.97 | 18562 | 18957 | 0.039 | 0.035 |
| fit.loadings | 179.56 | 131 | 0.979 | 0.976 | 18544 | 18882 | 0.035 | 0.038 | |
| fit.intercepts | 195.33 | 141 | 0.977 | 0.975 | 18540 | 18834 | 0.036 | 0.04 | |
| fit.means | 202.1 | 144 | 0.975 | 0.973 | 18540 | 18822 | 0.037 | 0.045 | |
| South Africa | fit.configural | 260.61 | 124 | 0.949 | 0.936 | 20134 | 20520 | 0.055 | 0.042 |
| fit.loadings | 283.35 | 134 | 0.944 | 0.935 | 20137 | 20476 | 0.055 | 0.05 | |
| fit.intercepts | 297.18 | 144 | 0.943 | 0.938 | 20131 | 20424 | 0.054 | 0.051 | |
| fit.means | 314.43 | 147 | 0.937 | 0.934 | 20142 | 20422 | 0.056 | 0.061 | |
Note: Fit measures for MGCFA include chi-square, Tucker-Lewis index (TLI), comparative fit index (CFI), root-mean-square error of approximation (RMSEA) and standardized root-mean-square residual (SRMR). The Akaike information criterion (AIC) and the Bayesian information criterion (BIC) can also be used to compare competing models and balance model fit and model complexity. While the CFI ranges from 0 to 1, the TLI can exceed 1. Acceptable values should be in the 0.90 range, and are better if they are greater than 0.95. TLI attempts to correct for model complexity but is somewhat sensitive to a small sample size. The RMSEA and the SRMR decrease as fit improves; therefore, the lower the value, the better. The SRMR ranges from 0 to 1, and it is generally agreed that a value less than 0.05 is a good fit and that those around 0.8 are acceptable. RMSEA is insensitive to sample size, but sensitive to model complexity (Bialosiewicz et al., 2013).