
Abstract
This paper presents findings from a systematic review of the literature concerning continuity of care for people released from prison or jail with serious mental illness. Sixteen papers were included in the review. The review addresses two research questions: the extent to which people continue to access mental healthcare following release, and the impact of interventions designed to improve continuity of care on mental health and criminal justice outcomes. Descriptive studies indicated that post-release engagement with community mental health services still requires improvement. Expedited Medicaid programmes improved enrolment and use of outpatient and prescription services but did not impact significantly on use of psychiatric services. Impact on criminal justice outcomes was variable. The remaining papers reported on a diverse range of interventions, and we can tentatively conclude that effective interventions for improving mental health and justice outcomes are likely to be intensive, multicomponent, and must start pre-release.
Background and aims
The prevalence of serious mental illness (SMI) in prison populations is considerably higher than in the general population (Coid et al., 2002; Fazel and Seewald, 2012). This is the case across the world. People released from prison experience high rates of SMI, suicide attempts, substance dependence and childhood adversity (Bebbington et al., 2021).
Transitions from custody to community are associated with a loss of contact with services, raising concerns about adverse mental health and criminal justice outcomes, and increased crisis service use as a consequence. A range of intervention to improve these transitions for people with mental illness have been described, including specialised mental health probation staff, forensic transition programmes, a scheme assisting people in prison with obtaining benefits pre-release (Haimowitz, 2004), and models such as Critical Time Intervention, Prison Aftercare Programmes, and Forensic Assertive Community Treatment (Galletta et al., 2021), and it is important to understand what constitutes effective practice.
A previous systematic review investigated interventions for people transitioning from prison diagnosed with any mental health condition (Hopkin et al., 2018). This was the first systematic review to focus on interventions at this transition point, and it examined the effectiveness of interventions in three domains: health insurance coverage; health service use and forensic outcomes, finding some evidence that interventions at this transition point improved contact with community mental health services, but further high-quality evidence is needed. The impact on reoffending and reincarceration was mixed, with increased reincarceration reported in some cases due to increased monitoring (Hopkin et al., 2018).
To date, no systematic review has focused on interventions specifically aiming to improve continuity of mental health care for people released from prison or jail with serious mental illness. Consequently, we aim to answer two questions: (1) To what extent do people with serious mental illness continue to access mental healthcare in the community on release from prison or jail? (2) What impact do interventions to improve continuity of mental health care for people in prison or jail with serious mental illness have on their mental health and criminal justice outcomes?
Continuity of care for SMI is defined in terms of the components described by Burns et al. (2009): experience and relationships; regularity; meeting needs; consolidation; managed transitions; care co-ordination and supported living.
Due to study heterogeneity, findings are presented as a narrative synthesis.
Methods
Search strategy
We searched PsycInfo, SocIndex, and ASSIA (December 2024 to January 2025), and MEDLINE (September 2025) to identify relevant peer-reviewed studies. A search strategy was initially constructed in PsycInfo with assistance from a specialist and translated for the remaining databases. This consisted of keywords and subject headings relating to SMI, prison release and continuity of mental healthcare (Appendix 1). We also drew upon our existing knowledge of the literature.
Study selection and data extraction
Search results were exported into Microsoft Excel where duplicates and any studies published in a language other than English were removed. Two reviewers independently screened titles and abstracts against the study inclusion and exclusion criteria.
To be included in the review, studies needed to report (a) the extent to which people released from prison or jail with SMI access mental healthcare in the community post-release, or (b) outcomes from an intervention or combination of interventions aiming to improve continuity of mental health care on release for people in prison or jail with SMI. Here, SMI (sometimes referred to as “severe mental illness”) was defined as including schizophrenia, schizo-affective disorder, bipolar disorder, major depression and other psychoses not related to drug or alcohol misuse.
Outcomes of interest were mental health outcomes including severity of disorder, number of days in hospital, use of crisis care, and rates of hospitalisation; and criminal justice outcomes including frequency and speed of re-offending, rates of breach of probation or parole conditions, jail or prison days and reimprisonment rates.
The following were excluded: books, book chapters, book reviews, commentary or opinion pieces, conference abstracts, dissertations and theses, editorials, reports, letters, papers that: purely described (an) intervention(s) rather than reporting outcomes, did not focus on people released from prison or jail settings, were about continuity of care for non-mental health related conditions, or reported criminal justice outcomes but did not report the extent of continuity of care. We also excluded papers where mental illness was considered in the round and SMI was not specified, or where common rather than serious mental illness was the focus of interest. Finally, we excluded qualitative research where the quantitative indices we sought were not available. No limits were placed on date of publication.
We ordered full copies of all papers that either reviewer had marked for inclusion or as unclear whether it met the inclusion criteria. These were independently read in full and classified as included or excluded in Microsoft Excel. The reviewers’ decisions were compared, and disagreements were resolved through discussion.
Two reviewers extracted details of when and where the studies were published, SMI diagnoses within the sample; study design; outcomes measured and key findings in relation to our research questions into pre-formatted tables in Microsoft Word.
Quality and risk of bias assessment
Quality appraisal of all papers including risk of bias assessment was conducted using the Mixed Methods Appraisal Tool (Hong et al., 2018). Consistent with the Mixed Methods Appraisal Tool guidance, no studies were excluded from the review based on quality assessment.
Results
Our initial interest in conducting a review in this area arose after reading 23 papers about continuity of care for people in prison or jail in general, and identifying a gap in the literature for a review relating to people in prison or jail with SMI. Of these initial 23 papers, 14 did not meet inclusion criteria for this review, and eight were subsequently also identified in the database searches, leaving one which was included in the review. One additional paper came to our attention during the course of writing the review.
A total of 2136 papers were identified in the database searches. After duplicates were removed, the remaining 2017 were screened against the inclusion and exclusion criteria, and 1879 were excluded from the review. Of the remaining 138 papers, we were able to access and assess 137 in full.
After full-text screening, 14
1
papers were included in the review, taking the overall total to 16 (Figure 1). Most studies were rated as moderate to high quality (Appendix 2). Green et al., (2016a, 2016b) note 41% of people referred to the initiative they evaluated did not provide consent for their data to be used for the evaluation. Studies also note concerns around attrition (Chandler and Spicer, 2006; Jarret et al., 2012), differences between groups at baseline (Chandler and Spicer, 2006; Wenzlow et al., 2011 [although the impact of this is unclear]), and intervention fidelity (Green et al., 2016a, 2016b; McKenna et al., 2015; Shaw et al., 2017; Wenzlow et al., 2011). Any concerns are noted in Tables 1–3 and Appendix 2. Preferred reporting for systematic review and meta-analysis (PRISMA) flow diagram. Studies describing post-release service use. Studies of the impact of expedited Medicaid. Intervention studies.


Of the included studies, 10 were conducted in the USA (Chandler and Spicer, 2006; Cuddeback et al., 2016; Cusack et al., 2010; Domino et al., 2019; Gertner et al., 2019; Grabert et al., 2017; Kubiak et al., 2011; Lovell et al., 2002; Morrissey et al., 2016; Wenzlow et al., 2011), two in Australia (Chowdhury et al., 2022; Green et al., 2016a, 2016b), three in the UK (Jarrett et al., 2012; Lennox et al., 2012; Shaw et al., 2017) and one in New Zealand (McKenna et al., 2015).
We divided the studies into those that simply describe patterns of post-release service use (n = 4), those assessing the impact of expedited Medicaid programs (n = 6) and studies investigating the effectiveness of other interventions (n = 6).
Studies describing patterns of post-release service use
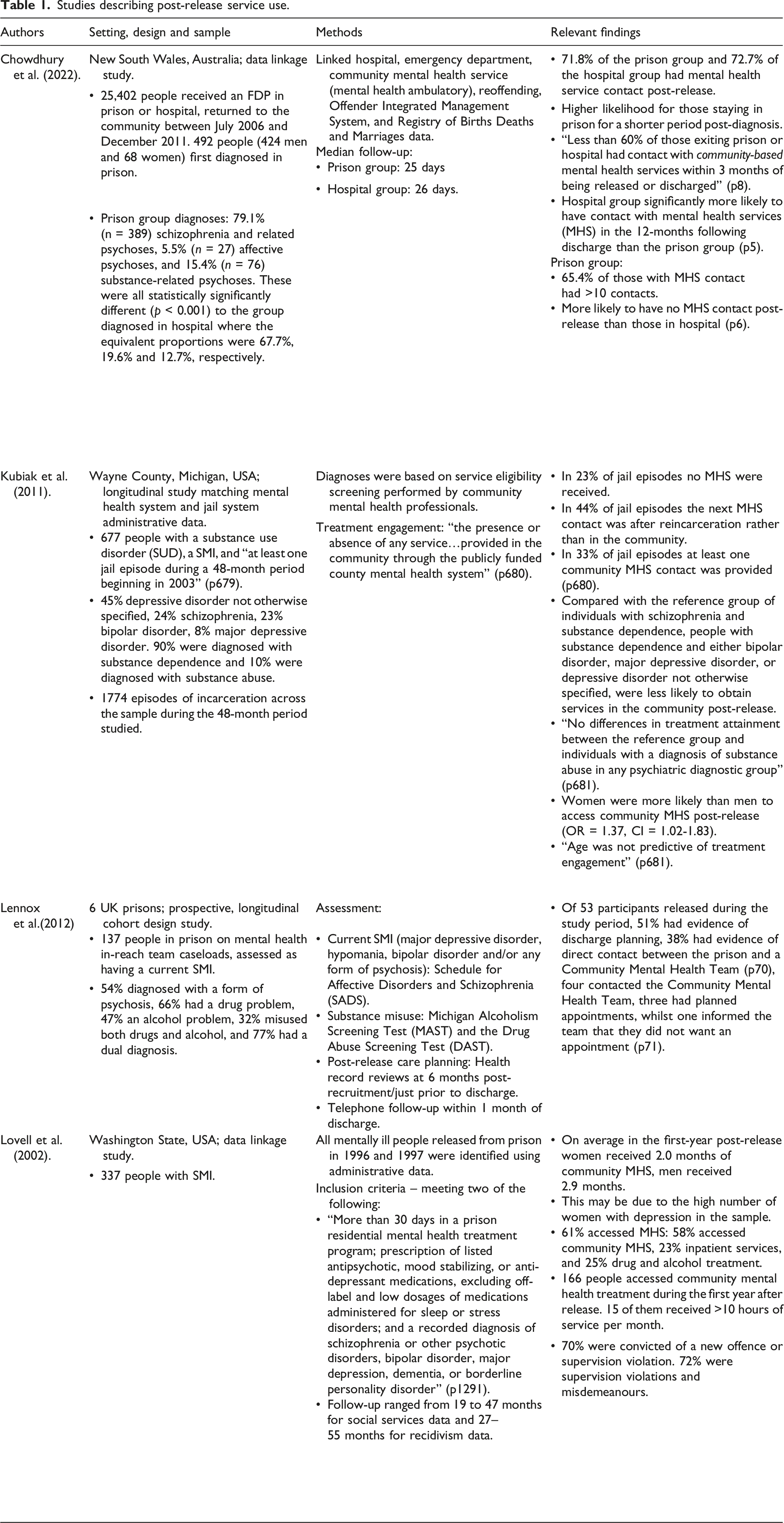
Lennox et al. (2012) examined transition planning and post-release contact with Community Mental Health Teams for people with severe and enduring mental illness on prison in-reach team caseloads. There was documented evidence of discharge planning for 27 of the 53 people released during the study period (i.e. Burns et al.’s managed transitions), and of direct communication between a prison and a Community Mental Health Team regarding just 20 of these individuals (Table 1). At 1-month follow-up, just four individuals had been in contact with a Community Mental Health Team, one of whom did not want to attend an appointment.
Kubiak et al. (2011) examined transition to community mental health services in people with both SMI, and a substance use disorder and “at least one jail episode during a 48-month period beginning in 2003” (Kubiak et al., 2011: 679). In 23% of the 1774 episodes of incarceration examined people did not access mental health services in the community or in jail, and in 44% of jail episodes, individuals’ next contact with mental health services was when they were reincarcerated rather than when they were in the community. Women were more likely to access community mental health services post-release than men, and compared with the reference group of individuals with schizophrenia and substance dependence, people with substance dependence and either bipolar disorder, major depressive disorder, or depressive disorder not otherwise specified, were less likely to obtain services in the community post-release.
In a study of 337 people with SMI that were released from Washington’s state prisons Lovell et al. (2002) reported that 61% of the sample accessed some form of mental health service during the follow-up period, with 58% accessing community mental health services, and 23% inpatient services. The authors state that “the intensity of community mental health treatment was low for most subjects in the first-year after release” (Lovell et al., 2002: 1293); over 90% received less than 10 hours of service per month in the months where they accessed care. On average individuals received two to 5 hours of service per month when they were accessing care – a level that the authors state may be insufficient. On average in the first-year post-release women received 2.0 months of community mental health services and men received 2.9 months. The authors state that this may be due to the high number of women with depression in the sample.
One study showed that those first diagnosed with psychosis in prison were significantly “more likely to have no contact with mental health services post-release compared to those [first diagnosed] in hospital” (Chowdhury et al., 2022: 6). Those imprisoned for a month or less after the diagnosis were more likely to have mental health service contact post-release than those that were imprisoned for 1–3, 3–6, or more than 6 months.
Thus, in relation to our first research question, continuity of care for people with SMI needs to improve, with this perhaps being particularly important for those first diagnosed with psychosis in prison.
Expedited Medicaid programs
Turning to our second research question, six US studies examined the impact of expedited Medicaid in jail and prison settings (Cuddeback et al., 2016; Domino et al., 2019; Gertner et al., 2019; Grabert et al., 2017; Morrissey et al., 2016; Wenzlow et al., 2011) (Table 2). The approval rate for expedited Medicaid varied by setting, with 91% of those from psychiatric hospitals, 83% of those from state prisons and 66% of those from county jails being approved (Cuddeback et al., 2016: 837).
It is clear that those receiving (Wenzlow et al., 2011), being approved for (Cuddeback et al., 2016) or simply being referred for expedited Medicaid (Grabert et al., 2017; Morrissey et al., 2016) ultimately have higher rates of enrolment with Medicaid. This appears to translate into increased use of outpatient services (Cuddeback et al., 2016; Domino et al., 2019; Grabert et al., 2017; Morrissey et al., 2016; Wenzlow et al., 2011), prescription drug use (including prescription refills) (Cuddeback et al., 2016; Domino et al., 2019; Wenzlow et al., 2011) and substance use disorder services (Gertner et al., 2019). However, there were no significant differences between groups in use of psychiatric services and inpatient care. Cuddeback et al. (2016) noted that whilst there were statistically significant differences in care access between those with and without approval for expedited Medicaid for those referred from jail, the differences for those referred from prison were not statistically significant. Grabert et al. (2017) and Morrissey et al. (2016) also reported higher rates of emergency department use in those receiving expedited Medicaid intervention compared to the control groups. However, it is unclear whether this specifically relates to mental health-related contact.
Criminal justice outcomes were either not significantly impacted (Grabert et al., 2017; Morrissey et al., 2016) or negatively impacted (Domino et al., 2019; Morrissey et al., 2016), although Domino et al. found “no significant effect of timely treatment induced by Medicaid on prison reincarceration for new charges” (Domino et al., 2019: 598).
Intervention studies
The remaining studies investigated the effectiveness of other interventions to improve continuity of care (Chandler and Spicer, 2006; Cusack et al., 2010; Green et al., 2016a, 2016b; Jarret et al., 2012; McKenna et al., 2015; Shaw et al., 2017). These include a randomized controlled trial (RCT) of an Integrated Dual Disorders Treatment (IDDT) community-based after-care programme aiming to “reduce inappropriate use of high-end [mental health] services while increasing engagement and the consistent use of community-based services” (Chandler and Spicer, 2006: 413). The in-custody component was provided to both experimental (n = 103) and control arm (n = 79) participants. Controls also received “usual services” post-custody (including referral for case management and medication, plus “up to 60 days of post-release grant-funded case management and housing assistance” (Chandler and Spicer, 2006: 408). The experimental group received IDDT for up to 2.5 years (see Table 3 for the components). Comparison of baseline and study period data showed that the experimental and the control group had a significant reduction in jail days but not in felony convictions. There was a significant reduction in arrests and total convictions in the experimental group only. Comparisons between groups showed no significant difference in time to first re-arrest, total number of re-arrests or jail days. The experimental group had significantly fewer incarcerations than the control group. There was no significant change in psychiatric hospitalisation days for the experimental group, whilst this increased significantly for the control group. The same was true for crisis visits. Overall, “77% of experimental and 18% of control participants did receive an engagement-related service within 60 days after leaving jail” (Chandler and Spicer, 2006: 417). The equivalent figures for receipt of psychiatric medications during the study period were 83% and 62% respectively. There was no significant change in the average mental health service costs per participant for high-end services (days for acute hospitalisation, long-term nursing home care and psychiatric crisis care) for the experimental group, but costs increased for control group members. Average “engagement-related services” costs (outpatient, day treatment and vocational services) increased from $2,276 to $11,787 for the experimental group participants and from $1,037 to $2,829 for control group participants (Chandler and Spicer, 2006: 415).
Cusack et al. (2010) investigated a Forensic Assertive Community Treatment intervention for frequent jail users with SMI. There was no significant difference in conviction rates between groups. Intervention participants were less likely to be jailed than controls in the first year, but “once in jail, there was no difference in length of stay” between groups (Cusack et al., 2010: 6). There was no significant difference in the rate of crisis service use, or whether people were hospitalised. Intervention participants had significantly fewer days of psychiatric hospitalisation compared to TAU participants and over twice the rate of outpatient visits in the first year (Cusack et al., 2010: 6). Per-person inpatient costs were lower and outpatient costs higher for the intervention group than for TAU. Per person jail costs were lower for Forensic Assertive Community Treatment than TAU in both years.
McKenna et al. (2015) evaluated the introduction of a standardised prison in-reach model informed by assertive community treatment principles. This consisted of screening, referral, assessment, treatment and release planning. Outcomes were compared for prison in-reach team caseloads from the year prior to the introduction of the new model and the year after implementation. During the 6 months post-release, the proportions of each group receiving new charges or being convicted were similar. Post-implementation, the proportion of males on remand engaging with general mental health services increased significantly from 42% to 63% (Z = .1947, p = 0.05) (McKenna et al., 2015: 435), and there was significantly more engagement with probation services at the women’s prison (McKenna et al., 2015: 435-436). There was a significant improvement in the rate of people released from prison taking up at least one face-to-face appointment with community mental health services (Z = 2.388, p = 0.02).
Green et al., (2016a; 2016b) described outcomes from a transitional support initiative in Queensland, Australia. The initiative had two components – a prison mental health service Transitional Coordination Program (TCP) focused on release planning and facilitating continuity of care, and a Transition Reintegration Recovery and Support (TRRanS) Program providing social and recovery support for up to 6 months. The study compared people accessing TCP only (n = 10), “TR-Short” – those only receiving TRRanS support whilst in prison or that received support for less than 62 days in the community (n = 30), and “TR-Long” – those receiving 62 days of more of TRRanS support in the community (n = 23) (Green et al., 2016a: 801). Risk of reincarceration was decreased by receiving either no TRRanS community support or longer-term TRRanS community support. The proportions of the TR-long group that were hospitalised post-release, and that were treated under the Mental Health Act were higher than in the other groups. A higher proportion of the TR-long group engaged with public community-based mental health provisions of service than in the other groups. Overall, 28.6% of participants did not engage with these services. The median length of engagement was longer for the TR-long group than either of the other groups. A greater median number of provisions of service were associated with being under the Mental Health Act during the follow-up or a lifetime history of being under the Mental Health Act, and with a diagnosis of psychosis at release.
In a pilot RCT Jarrett et al. (2012) compared Critical Time Intervention (CTI) and TAU in 60 people in prison in three local prisons in the UK, (n = 23 followed up: CTI = 15, TAU = 8). Some positive trends were reported (Table 3), but high attrition limited conclusions. During the study, some CTI managers were based with prison in-reach teams whilst others were based with Community Mental Health Teams. The researchers stated that a future model in which the CTI manager is based with an in-reach team is preferable. An RCT following on from this pilot study reported significant improvement in engagement with community mental health services at 6-weeks and 6-months post release, but not at 12-months post-release (Shaw et al., 2017) (Table 3). Economic analysis showed higher costs (measured as services received) for the intervention group than for the control group, but further research is needed to determine whether the increased engagement with services will keep people well for longer and whether this will translate into reduced health and criminal justice-system costs in the long-term.
Discussion
This review identified 16 studies, mostly from the US, Australia, and the UK. The focus was specifically on CoC for people with SMI released from prisons or jails and exclusively qualitative research was excluded. None of the studies identified examined the role of probation services (including those with mental health specialist roles) in release planning. This is an important limitation of the current evidence base as arguably probation services should be a key part of any initiative to improve CoC for people leaving prison.
We reported the studies in three broad categories: naturalistic studies (simply exploring post-release outcomes); expedited Medicaid studies; and intervention studies. The naturalistic studies were heterogeneous, but overall, strongly suggest that mental health service use by people released from prisons or jails could be much improved, especially in community mental health services.
In relation to our second research question, the studies of expedited Medicaid point to a significant positive impact on Medicaid enrolment and subsequent community mental health service use (Gertner et al., 2019; Grabert et al., 2017; Morrissey et al., 2016), suggesting that investing in such an approach where individuals require health insurance coverage is worthwhile. However, such interventions may increase the probability of re-imprisonment, likely due to violations rather than new offences (Domino et al., 2019).
Intervention studies were diverse in design and scope. Apart from one pilot study where high attrition made it impossible to draw inferences (Jarret et al., 2012), most interventions improved engagement with community mental health services post-release, and in some cases, reduced days of psychiatric hospitalisation. That said, many people still received little or no community care post-release. Further research is needed to understand and respond to reasons for attrition. There is a weak link between services received and future recidivism.
Evaluations of Forensic Assertive Treatment have produced mixed findings, likely due to variation in model implementation (Goulet et al., 2022; Lamberti and Weisman, 2025; Lurigio et al., 2004; Smith et al., 2010). Key components have now been identified as a high-fidelity Assertive Community Treatment team, dual (mental health and criminal justice system) admission criteria; risk/needs assessment; collaboration with criminal justice professionals; legal leverage (offering treatment as an alternative to punishment); informed choice to accept the treatment; evidence-based mental health and substance use intervention; evidence-based criminal justice intervention; and shared training (between mental health and criminal justice professionals) (Lamberti and Weisman, 2021, 2025). Further evaluation of services implementing these elements is required.
Further research is also needed for us to be able to identify which interventions most effectively improve CoC for people released from prison or jail with SMI, let alone for particular subgroups of this population. Whilst this review specifically focused on interventions to improve CoC for people in prison or jail with SMI, it is important to note that a meaningful proportion of this population have comorbidity of SMI and substance misuse. These individuals have a higher risk of reincarceration than those with SMI or substance use disorder alone (Baillargeon et al., 2010) and comprise a substantial proportion of frequent users of emergency care (Butler et al., 2020; Snow et al., 2022). This is arguably a key consideration for intervention planning.
Despite variability among studies, we can tentatively conclude that whilst they may be costly, intensive, multi-component services that embed discharge planning pre-release impact positively on post-release engagement with mental healthcare. Often these include a form of release planning and medication and in some cases include elements that are not specifically about mental health treatment such as support with housing or finances. Impact on criminal justice outcomes is mixed, but one study suggested that longer interventions (lasting more than 2 months) may have more impact on reincarceration outcomes than shorter interventions (Green et al., 2016a, 2016b). Given the high levels of attrition in engagement with services, future research should explore the impact of lived experience involvement in future intervention design on duration and quality of engagement. Finally, many studies only recorded service use, assuming that mental health service utilisation equates to benefit. Future work should measure quality of service provision and outcomes such as quality of life and flexible continuity.
Conclusion
It seems clear that most individuals received little or no community care after their release. Medicaid improves access to services but not necessarily criminal justice outcomes. Effective interventions for improving mental illness and justice outcomes are likely to be intensive, multicomponent (including addressing dual diagnoses and wider issues such as housing and finances), and must start pre-release. Further work is needed to understand the reasons behind attrition in engagement with services and interventions and to investigate the impact of engagement with services on other outcomes such as quality of life. Lived experience perspectives may be crucial for any future studies in this area.
Footnotes
Acknowledgements
Thank you to Marishona Ortega, Academic Services Manager for her assistance with constructing and conducting the database searches.
Ethical considerations
Ethical approval was not required for this review.
Consent to participate
There are no human participants in this article and informed consent is not required.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.