
Abstract
The business model canvas is a popular tool used to develop value-driven business models. Specific emphasis is placed on understanding what customers value and providing users with steps on how to design and deliver value for their customers. In health care, creating and delivering value for patients is an often-discussed topic, with the provision of patient-centered care becoming a standard for many health care organizations. While patients play a key role in determining value, providers are the key to delivering value. Therefore, effective health care management relies on integrating multiple perspectives from key stakeholders. This process requires consideration of the key needs that must be addressed, the resources and capabilities necessary to meet these needs, and the interests and values specific to each set of stakeholders. The business model canvas lends itself well to health care service planning as it incorporates the factors described above into the business model’s conceptualization and subsequent realization. This article outlines how the business model canvas was applied to assess the needs of physician stakeholders to help guide the expansion of a pharmacogenomic-based precision medicine clinic that conducts genetic testing for patients at risk of experiencing adverse drug reactions. The article provides a detailed description of how the business model canvas was used and adapted to understand physician’s responsibilities and challenges related to drug prescription and dosing, and how the clinic could address physician needs and create value by mapping clinic services onto physician needs and wants. Interviews were conducted with physicians and the data were analyzed following the recommendations of the developers of the business model canvas. The article examines the strengths and limitations of the business model canvas and discusses its applicability to a health care setting.
Introduction
A business model outlines how a business intends to design, deliver, measure, and capture value for and from its customers. Maximizing an enterprise’s value generation capability requires a grounded understanding of the environment it operates in. A popular tool for and enhancing managerial understanding of the environmental landscape and subsequent business model development is the business model canvas (BMC) (Osterwalder and Pigneur, 2010). A core feature of the BMC is its visual representation of business models and the provisioning of tools for users on how to do so (Ching and Fauvel, 2013). The BMC is lauded for its simplicity and the iterative process it advocates, enabling users to refine their business models as their strategic plans evolve over time. Although originally intended for use by entrepreneurs and start-ups in the early stages of business development, the BMC can be applied to a variety of sectors to help guide organizational planning, product, and service portfolio management, and assist in assessing stakeholder needs and values.
Effective management of health care relies on multiple interactions with key stakeholders to deliver products and services to meet the needs of patients and providers. This process requires consideration of the key needs that must be addressed, the resources and capabilities needed to implement and deliver products and services, and the interests and values of a multi-faceted set of stakeholders (e.g. health care providers, administrators, funding agencies). The BMC lends itself well to health care service planning as it incorporates the factors described above into the business model’s conceptualization and subsequent realization. Accordingly, the purpose of this article is to describe how the BMC was applied in a health care setting to identify the needs of physician stakeholders to help guide the expansion of a precision medicine (PM) clinic that conducts genetic testing for patients at risk of experiencing adverse drug reactions (ADRs).
Introduction to the BMC
The BMC consists of nine building blocks: customer segments, channels, customer relationships, revenue streams, key resources, key activities, key partnerships, cost structure, and value propositions (Osterwalder and Pigneur, 2010). Customer segments represent the people a business intends to market a product or service to. Channels are the ways through which a business reaches its customer (e.g. through a website). Relationships refer to the types of relationships a business has with its customer segments (e.g. automated, face-to-face). Revenue streams represent all the sales generated through the business. Key resources describe the most important resources (i.e. financial, physical, intellectual, and human) needed for the business to operate, while key activities lay out the actions a business must take to deliver services. Key partnerships refer to the affiliates needed for the business to successfully operate. Cost structures encompass all the expenses incurred by business. Finally, value propositions are statements that describe what a business is offering and how this offering will generate value for customers (Osterwalder and Pigneur, 2010). Customer segments, channels, and customer relationships represent the market while key resources, key activities, key partnerships, revenue streams, and cost structure represent the business operations. Value propositions reside between the market and the firm’s operations (Osterwalder and Pigneur, 2010) shaped by market demands and firm operational capability. This article will focus specifically on customer segments and value propositions.
Value and value creation
The concept of value is emphasized throughout the BMC. Payne et al. (2017) define value as “the set of experiences that a business causes its customers to have” and often refers to the benefits an offering (product/service) creates for its customers. This definition implies that determining whether or not a product/service has value is a subject to evaluation on the part of the customer (Barrett, 2014). The customer must determine whether a product/service is of any benefit to them and decide if gaining this benefit is worth the cost of what a business is offering (Smith and Colgate, 2007). It is important to note that value does not always mean acquiring a good or service at a lower cost (Pitelis, 2009). The customer must believe that the price they pay is worth the experience or benefits that a product/service will provide and “firms exist to create value for others where it is neither efficient nor effective for buyers to attempt to satisfy their own needs” (Smith and Colgate, 2007: 7).
Smith and Colgate (2007) delineate different types of value based on what a firm’s offering provides for or elicits within customers. Functional/instrumental value refers to the extent to which a product performs as promised. For example, Dyson promises its customers that their vacuum cleaners are designed with the latest technology and will cover more floor with each sweep than other vacuums, facilitating a deeper clean. Experiential/hedonic value focuses on creating experiences and evoking feelings for the customer. Dining at a Michelin star restaurant is one example of experiential value as customers derive pleasure and have their senses stimulated from the dining event. Symbolic/expressive value occurs when customers associate meaning to a product. The marketing of luxury goods falls into this category. Advertisements for luxury jewelry brands (e.g. Tiffany’s) often focus on highlighting special life moments such as engagements to get customers to attach their own personal meaning to their products. Finally, Smith and Colgate (2007) discuss cost/sacrifice value, which is concerned with minimizing costs and other sacrifice that may be involved in the purchase and use of a product (e.g. using biodegradable packaging to reduce waste associated with receiving a product). The types of value described above can be created in a variety of ways. It is essential that businesses understand what is important to their target customer in order to know how an offering should be designed and delivered to most effectively create potential value for their customers.
Value creation refers to the activities a company engages in and the strategies it implements to create value for its customers (Lindman et al., 2016; Pitelis, 2009). Value creation can be divided into two stages: value design and value delivery (Barrett, 2014). Value design includes understanding customer needs in order to determine what a firm will offer to its customers. Value delivery involves ensuring a company has the operational and managerial resources and capabilities to produce, distribute, market, and sell its offering to its customers (Barrett, 2014). Creating value is contingent on thoroughly understanding the behaviors, motivations, and needs of a business’ target customers (Hassan, 2012). This process of developing a deep understanding of customer needs is an integral part of business model development because it is important that resources are allocated properly and decisions are made that will yield results that align with business objectives, whether that be profit or impact generation. Consequently, understanding value from the customer perspective and incorporating value creation activities into the business model from the beginning of business model development can help better guide how the business will operate and achieve success. This is especially important when considering that the ultimate goal of value creation for the firm is value capture (i.e. the generation of profit from customer sales) (Pitelis, 2009).
Value proposition design
Value proposition design is a central output developed through the application of the BMC and has been identified by users of the BMC as the most important part of the model (Coes, 2014). Osterwalder and Pigneur (2010) emphasize the importance of designing strong value propositions in order to clearly convey to customers how an offering will generate benefit(s) for them through their engagement with the firm. The goal of value proposition creation is to clearly comprehend how the firm can potentially generate value for a specific set of customers, and to plainly and distinctly articulate why a customer should engage with the firm to acquire a good or service to capture incremental value. Well-developed value propositions can result in positive business outcomes as they can help retain customers, increase profits, and help reduce costs for firms (Hassan, 2012). Although commonly used to build marketing strategies, value propositions also contain pertinent information related to business operations. Value propositions provide information on who to target, where to allocate valuable firm resources, serve as a reminder of a company’s purpose, and set expectations for customers (Payne et al., 2017). In other words, value propositions can serve as roadmap for how a business should operate and achieve success and are thus a key component of the value creation process (Payne and Frow, 2005). However, businesses frequently report limited success in value proposition development and application. Research has demonstrated that less than 10% of companies have successfully developed and communicated value propositions to customers (Payne et al., 2017). Given their importance to business models and ultimately firm success, it is important to ensure that value propositions are mindfully constructed and informed by data throughout the business model development process.
Applying value proposition design within a health care setting
Health care is an industry where the concept of value creation has been discussed heavily over the past decade (Marzorati and Pravettoni, 2017). Much of the discussion has focused on value-based health care (VBHC), which conceptualizes value as optimizing outcomes that matter to patients while minimizing the costs required to achieve those outcomes (Porter and Teisberg, 2007). While value can be generated through cost reduction without reductions in outcomes achieved (efficiency), value can also be created by ensuring health care services are implemented and delivered in a way that best meets patient needs (effectiveness). VBHC involves a shift in thinking about health care systems in terms of volume of services delivered to designing health care systems focused on outcomes that are important to patients, such as improvements in functional status, time needed to access and receive care, and quality of life (Porter et al., 2016). Research on implementing VBHC and improving value for patients has focused on various organizational aspects, including the use of different management strategies (e.g. LEAN management), developing new payment models for physicians, integrating hospital and community care, and examining the role of information technology (Clark et al., 2021).
While VBHC as conceptualized by Porter and Teisberg (2007) is focused on entire health care systems, the basic principle of understanding and focusing on patients’ needs and wants can be applied to improve the individual delivery of health care services and patients’ experiences of using those services. The emphasis on improving health care services to create value for patients aligns with the concept of patient-centered care, where the goal is to emphasize the patient and their needs at the core of care efforts. As an example, in Canada, the province of Ontario announced its commitment to patient-centered care through the passing of the Patients First Act (Government of Ontario, 2015). The province aimed to place the needs of patients first through improved access to care, enhanced coordination of care, education, and improved evidence-based decisions (Government of Ontario, 2015). Much of the Patients First Act focuses on health care delivery and the need to deliver care to ensure that patients receive the right care, at the right time and at the right place in an effort to guide providers and system administrators toward increased patient value creation. The development and design of value propositions through the application of the BMC would lend itself well to these stated objectives through its focus on understanding the customer (i.e. different health care stakeholders), their specific needs, and the best way to allocate and orchestrate resources to meet those needs. Therefore, health care services should incorporate value proposition development before designing, implementing, and delivering care in order to ensure patients receive the health care outcomes they need and want in those most effective and efficient manner possible.
The value of PM
The field of PM is an area of medicine frequently referred to as an example of patient-centered care. A core facet of PM is the analysis of patients’ genomic information to guide medical decision-making (e.g. tailoring drug dosages) (Overby and Tarczy-Hornoch, 2013). A large hospital in southwestern Ontario, Canada, has established an innovative PM clinic that conducts pharmacogenomics-based (PGx) testing for ADRs. Patients referred to the clinic undergo genetic testing for the likelihood of experiencing an adverse reaction to a specific drug their physician is considering prescribing or has already prescribed. Once a blood sample is taken and tested, the clinic physician reviews and interprets the results and makes a recommendation (e.g. start at lower dose and increase if tolerated) to the referring physician. The clinic mainly does genetic testing for chemotherapy drugs, gastrointestinal medications, and statins.
While successful to date, the PM clinic is considering expanding their services beyond their local region. Currently, all testing is done in-house with patient referrals processed on a rolling basis (first in, first out). The majority of referrals are generated from physicians and specialists who have an existing relationship with the clinic’s founding director or are based on word-of-mouth recommendations from other physicians or specialists. The PM clinic is currently funded through research grants, but those grants will eventually expire. Consequently, the clinic seeks to increase demand through the expansion of its reach to a broader population of patients and range of medical specialties, and to secure consistent non-research generated funds for ongoing clinic operation and potential expansion.
Purpose
Our research team was approached by the PM clinic to develop a go-to-market strategy outlining how the clinic should operate and be marketed to those outside its existing network in order to increase the scalability and uptake of their services. A carefully constructed go-to-market strategy that incorporates the perspectives of key stakeholders would be instrumental for understanding how the clinic generates value for physicians and patients, and how its value proposition should be crafted and articulated to ensure a greater chance of successful growth. The research team grounded its data collection and sense-making in the BMC framework as a means to guide the development of a go-to-market strategy for expanding the services of the PM clinic. A large part of this process involved understanding key customer segments, their needs/concerns, and how the clinic could address them in order to develop value propositions for marketing and business plan creation. While some researchers (León et al., 2016) have used the BMC in different health care settings, a detailed explanation of how the BMC was applied and adapted to be used within a health care context is lacking. In addition, while there is so much investment in basic science research, we cannot realize the full potential of basic science research investments without the complementary work of implementing and evaluating these discoveries into the health care system. This is where understanding the BMC in a health care setting can be helpful. Therefore, this article will outline how the research team used the BMC to design value propositions for physician stakeholders (customers). We will discuss our process of using the BMC and the model’s suitability for health care application. The goal of this article is to provide an in-depth description of the steps of the BMC method and any necessary adaptions. This article aims to provide guidance to those in the health care industry interested in understanding stakeholder needs in a comprehensive and systematic way and determining how to create or deliver health care services focused on what stakeholders value. Thus, the method used to identify stakeholder needs and values will be the focus of this article, with some of the findings from the stakeholder interviews used as examples to highlight different aspects of the value proposition design process.
Method
An exploratory qualitative design was employed to examine physician stakeholders’ perspectives on the use of personalized medicine in a clinical care setting. The goal of exploratory research is to investigate new phenomena or gain deeper insight into an already existing phenomenon (Swedberg, 2020). An exploratory approach aligns well with the principles of market research, which focus on identifying target markets and the needs and preferences of customers within that market (Osterwalder and Pigneur, 2010). An exploratory design was applied because the first step of determining how to expand the clinic’s services involves identifying and understanding customers’ needs and what customers value (Osterwalder and Pigneur, 2010). Qualitative methods enabled the research team to collect detailed data from physicians about their views and beliefs about the role of PM in patient care and their experiences using the PM clinic. Listening to participants’ experiences using the PM clinic allowed the team to identify and describe what physicians considered important to generate tailored value propositions. Semi-structured interviews were conducted, and the themes were generated from the data as recommended by the creators of the BMC (Osterwalder and Pigneur, 2010). The reminder of this article provides a comprehensive overview of the process the research team used to understand physician stakeholders’ needs and how the BMC was applied to develop value propositions for each stakeholder group.
Situating the PM clinic within the Canadian health care system
Prior to discussing the research team’s process of using the BMC, a brief overview of the Canadian health care system is needed to contextualize the findings. Canada has a single universal-payer system where the costs of health care services are shared by the federal and provincial governments (Government of Canada, 2011). Provincial governments are responsible for the delivery of health care services in their respective provinces (Government of Canada, 2011). Provinces receive funding for health care services from the federal government annually (via the Canada Health Transfer) and provide their own funding as well. Medically necessary services (i.e. services provided by a physician or services received in hospital) are publicly funded in Canada. Services such as home care, physiotherapy, and prescription drugs (unless administered in hospital) are not publicly funded and require citizens to pay for them out-of-pocket or through private insurance (The Commonwealth Fund, 2020). Hospitals are run on a not-for-profit basis and are managed by private or public companies (The Commonwealth Fund, 2020). Physicians in Canada are not employees of the government but are private practitioners who are reimbursed for their services on a fee-for-service basis (Government of Canada, 2011). Physicians bill the provincial government they practice in for each service, including referrals to other specialists, they provide to their patients (The Commonwealth Fund, 2020).
Value proposition design for the PM clinic
The BMC outlines three steps of value proposition design: (1) understanding your customer segments, (2) analyzing how your business can meet customer needs, and (3) creating the value proposition (see Figure 1). The first step involves getting to know and understand each customer segment through the creation of a customer profile. This step is critical as a well-designed value proposition should be tailored to, and resonates with, your target customers (Payne et al., 2017). A customer profile describes what a customer does (their jobs and roles), any challenges they experience (pains), and any benefits received through their role (gains). The second step of value proposition design involves determining how the business and its resources can best be cultivated and orchestrated to address the target customers’ needs. The BMC conceptualizes this process as value mapping and involves considering what you can offer to help with tasks and activities (products/services), the ways in which your business can solve customer complaints (pain relievers), and how you can create benefits (gain creators) for the targeted customer segment (Osterwalder and Pigneur, 2010). Finally, a value proposition is created that describes how the business will deliver value to the customer through analysis of the customer profiles and value maps. In addition, our research team added an intermediate step between steps 2 and 3 which consisted of validating the findings from the profiles and value maps.

Value proposition design process.
Step 1: constructing customer profiles
An initial consultation with the PM clinic staff was conducted to identify key customer segments. Customers were defined as the individuals who decide whether the PM clinic services should be used for patients. As a result, physicians were identified as the primary customers because they acted as the decision makers for whether or not a patient should be referred to the PM clinic. Patients were defined as consumers of the clinic services. Further consultation with PM clinic staff revealed the different individuals and departments with whom the clinic interacts to identify key physician customer segments. The clinic staff provided the names of physicians who regularly refer patients to the clinic, primarily from the oncology and gastroenterology departments. This customer segment reflected the current users of the PM clinic and was essential for the analysis. Current customers would be able to provide detailed insights into how the clinic currently functions in practice, and the benefits and challenges of using PM to inform enhanced decisions related to patient care. Following the initial interviews, snowball sampling was used to identify other individuals and other medical specialties with an interest in PM and the services of the PM clinic. It was important to include potential future customers when designing the PM clinic value propositions in order to gain an understanding of the resources required for the clinic to function in other specialty areas of medicine and how the needs of potential future users might differ from those of current users.
Once the customer segments were identified, participants were contacted via email to ascertain whether they were willing to participate in an interview. Semi-structured interviews were conducted over the phone and audio-recorded for future transcription. The goal of the interviews was to develop a broad understanding of each physician specialty group’s needs, and how the clinic currently fit, or could potentially fit, in with their practice operations. Approximately four to five physicians from each of the following specialties were interviewed: oncology, gastroenterology, family medicine, geriatrics, psychiatry, pharmacology, and pediatrics. The interviews focused on understanding physicians’ needs related to medication prescription and dosing. Specifically, participants were asked to (1) describe their job role and their duties related to medication prescription, (2) discuss any challenges they currently face in relation to prescription/drug dosing, (3) outline how PM fits in with their clinical practice, (4) identify and describe the benefits and challenges of using PGx-based testing as part of patient care, and (5) discuss the resources and capacity needed for expanding the services of the PM clinic.
Analysis of the interviews followed the steps recommended by the creators of the BMC (Osterwalder and Pigneur, 2010). The interviews were coded in order to construct a customer profile (see Figure 2) by identifying customer jobs, customer pains, and customer gains, with color codes created for each profile category. Customer jobs were anything related to the physicians’ responsibilities and tasks at work such as diagnosing patients and prescribing medication. Customer pains referred to any difficulties/challenges encountered by physicians in relation to medication prescription and dosing. For example, references to the trial-and-error nature of medication prescription and delays in patient treatment were coded as pains. Customer gains were identified through any references to benefits associated with the physician role and responsibilities such as reduced length of stay in hospital for patients and health systems cost savings. The BMC (Osterwalder and Pigneur, 2010) recommends ranking jobs, pains, and gains based on order of importance. Importance rankings were determined for each of the customer jobs, pains, and gains based on how frequently each of the categories was mentioned in the physician interviews. Themes that were mentioned across multiple interviews were given priority over those less frequently mentioned. The ranking process enabled a determination of what was likely most important to the physician customer and how the PM clinic could potentially meet those specific needs.
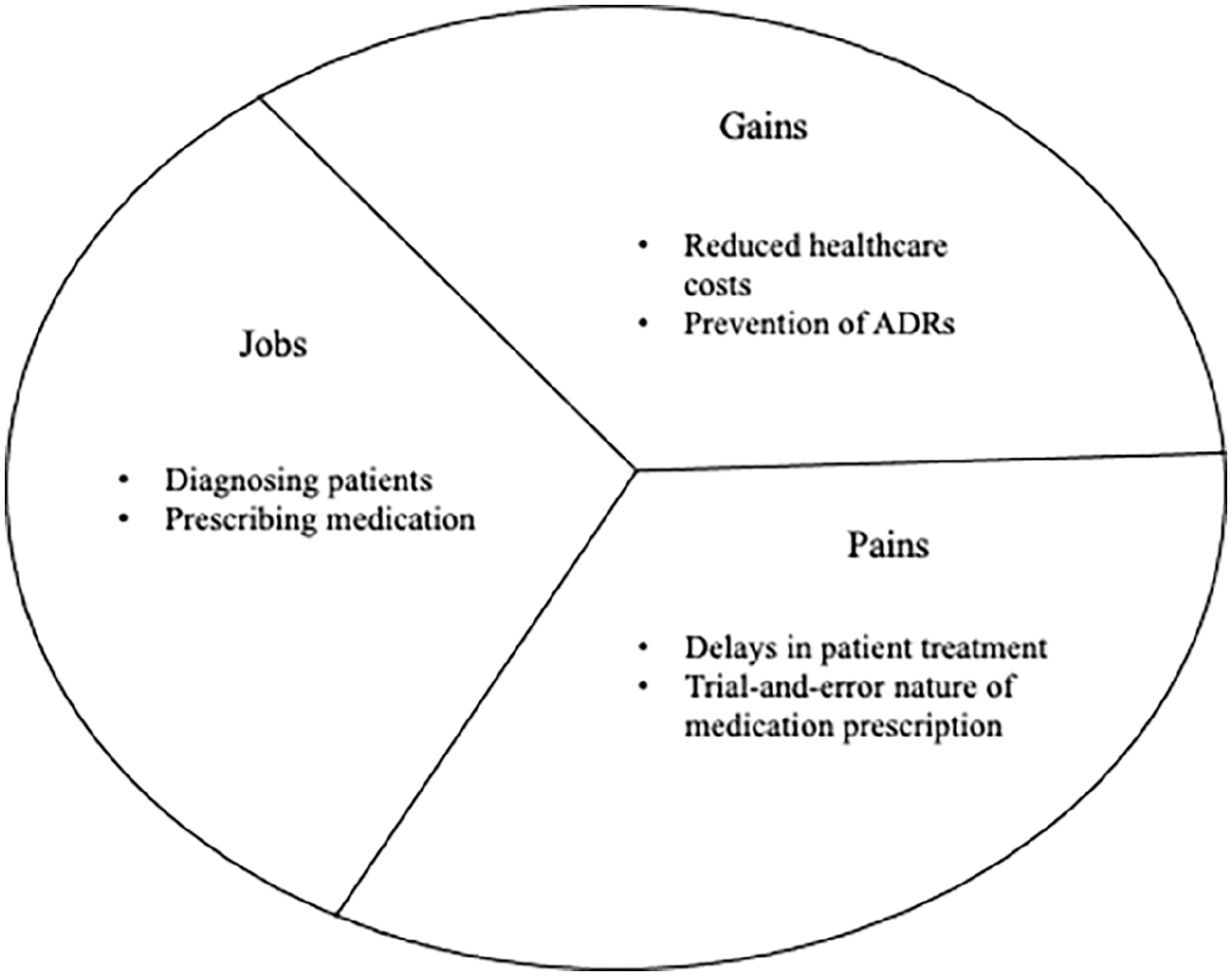
Sample physician customer profile.
Step 2: constructing value maps
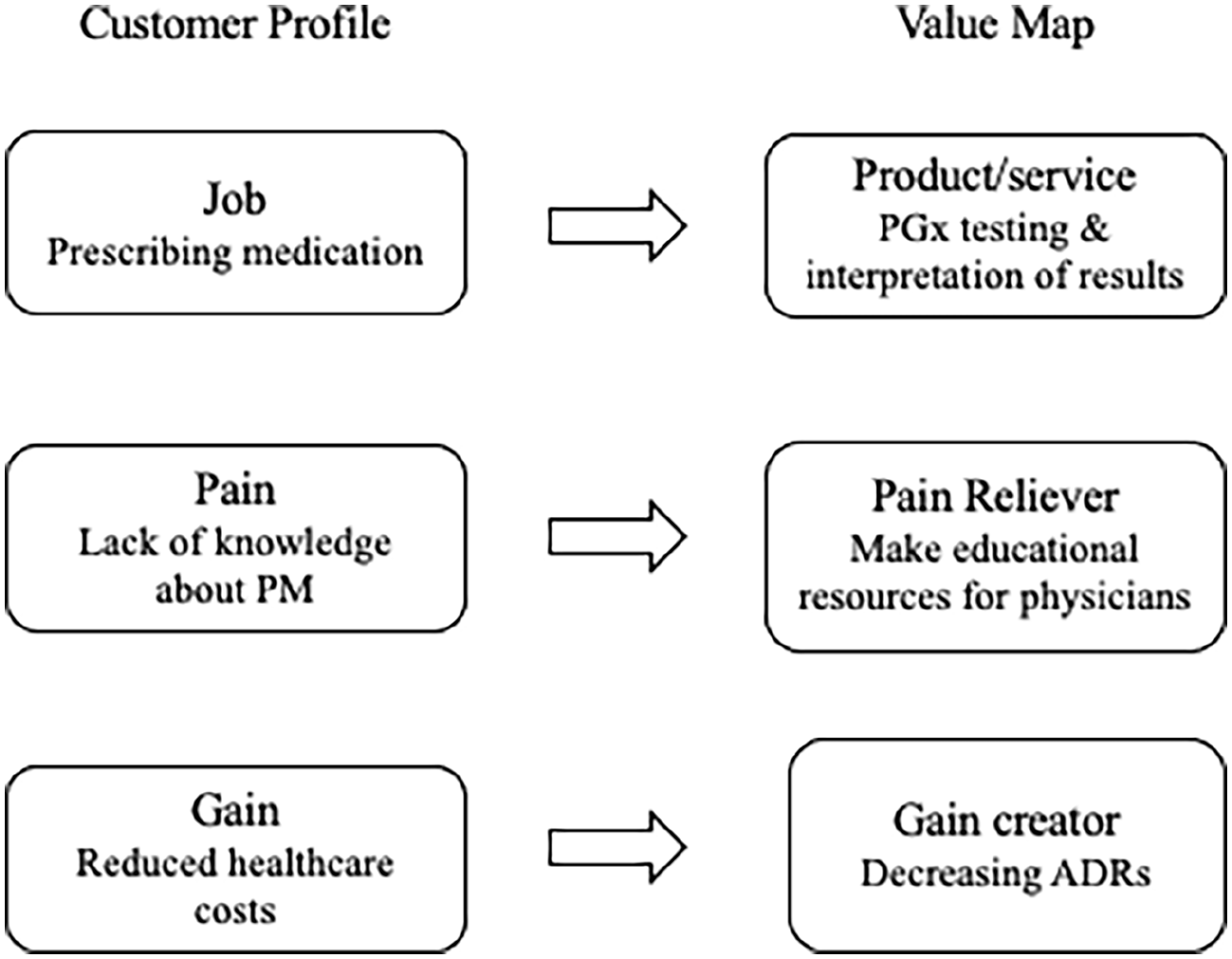
Once the customer profiles were complete, value maps (see Figure 3) were constructed for each customer segment. The value map is a tool used to think about which aspects of your business address customer needs and create value for customers. It is meant to help businesses reflect on their value proposition and how to tailor it to each customer segment. The top jobs and concerns of the physicians were focused upon when constructing the value map. Initially, the value map construction began by analyzing the most important customer jobs. In this instance, a principal focus was on testing for ADRs, thus multiple jobs related to medication management were identified, such as prescribing medications to patients, adjusting drug dosages, and treating drug side effects. The customer jobs were mapped onto the products/services of the value map, which refer to what the clinic is offering to the customer. The product/services were related to providing guidelines on which patients are eligible for testing in the PM clinic, education pamphlets for patients, education resources for physicians, and the actual testing provided by the clinic. In the next step, pain relievers were identified. These describe how the PM clinic will solve specific customer problems. For example, oncologists discussed delays in chemotherapy as a result of having to continually adjust dosages for patients experiencing ADRs. Accordingly, an identified pain reliever for the oncologists’ customer segment was the timely interpretation of patient test results and provisioning of a recommendation for drug selection/dose by the PM clinic physician in order to ensure chemotherapy can begin as soon as possible. The last section of the value maps includes gain creators, which describe how benefits will be created for customers through the product/service. One of the gain creators was identifying patients at risk of ADRs prior to prescribing a drug, thereby decreasing their chances of negative outcomes and decreasing length of stay in hospital.
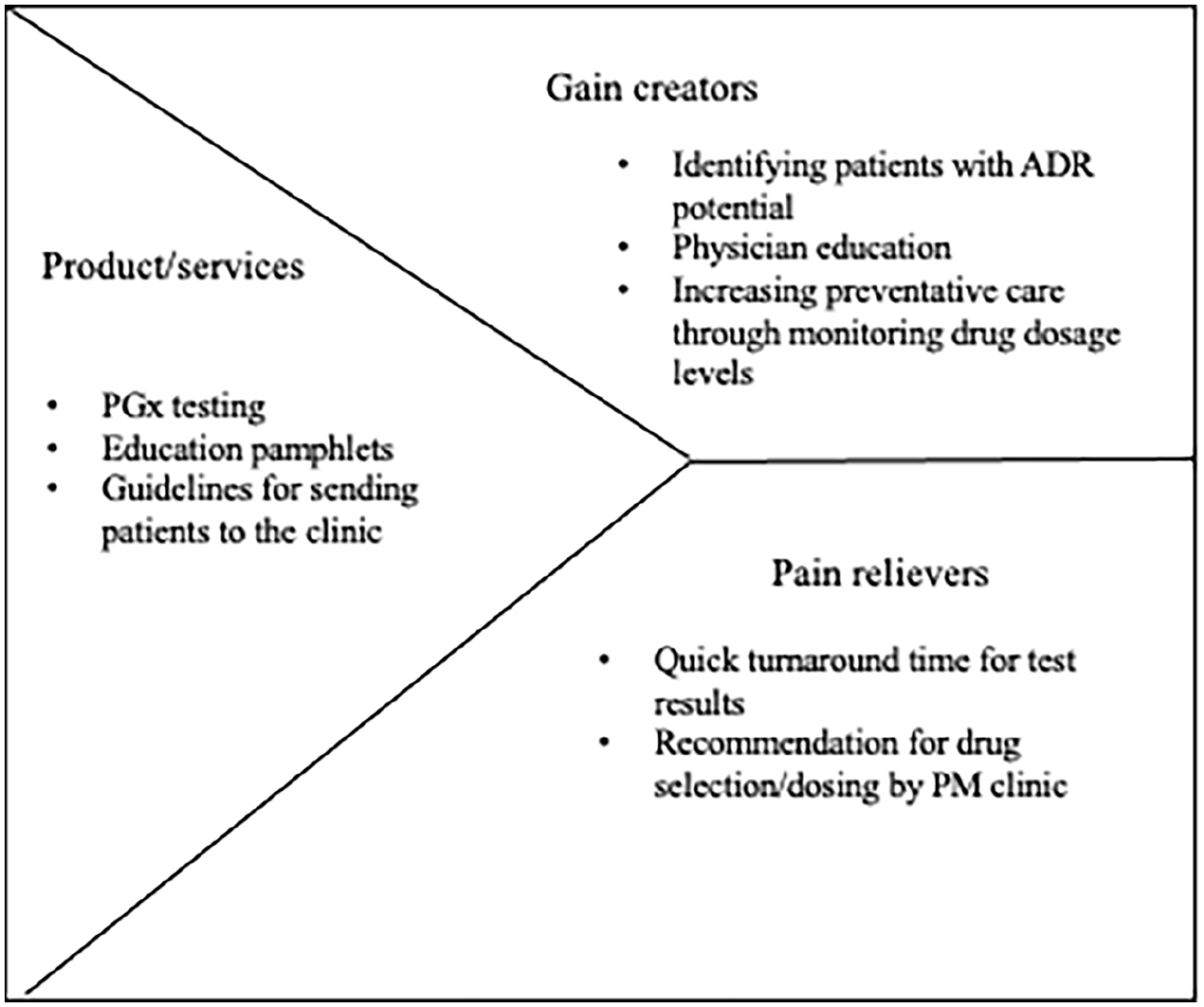
Sample physician value map.
Validating the customer profiles and value maps
Once the value maps were complete, members of the research team came together to review the data in order to verify and validate initial findings and initiate the development of customer value propositions (see Figure 4). Findings validation consisted of three major components. First, each member of the research team read over the interview transcripts and recorded any information that they thought would be relevant for the customer profiles and value maps. The purpose of returning to the transcripts was to ensure we did not miss any key information and to determine if any new information could be added to improve the customer profiles and value maps. Using multiple researchers to gather and examine data is one way to enhance the creditability (i.e. trustworthiness) of the data through crystallization (Tracy, 2010). According to Tracy (2010), crystallization involves the use of multiple researchers, different methods, or types of data to generate a more complex and in-depth understanding of a phenomenon. Having each member of the research team read the interview transcripts allowed us to collect multiple perspectives on the data and through group discussion about interviews, encouraged us to reflect more thoroughly on key customer needs and how the clinic could meet those needs. Revisiting the transcripts after having completed one set of analyses allowed the research team to deepen its understanding of the data and further identify nuances and subtleties that may not have been captured during the first round of data analysis. For instance, the researchers were able to break down the customer job of “develop treatment plans for patients” into specific tasks (e.g. monitor health, prescribe medication, collaborate with other care providers), giving greater insight into how the PM clinic could address all of these jobs.
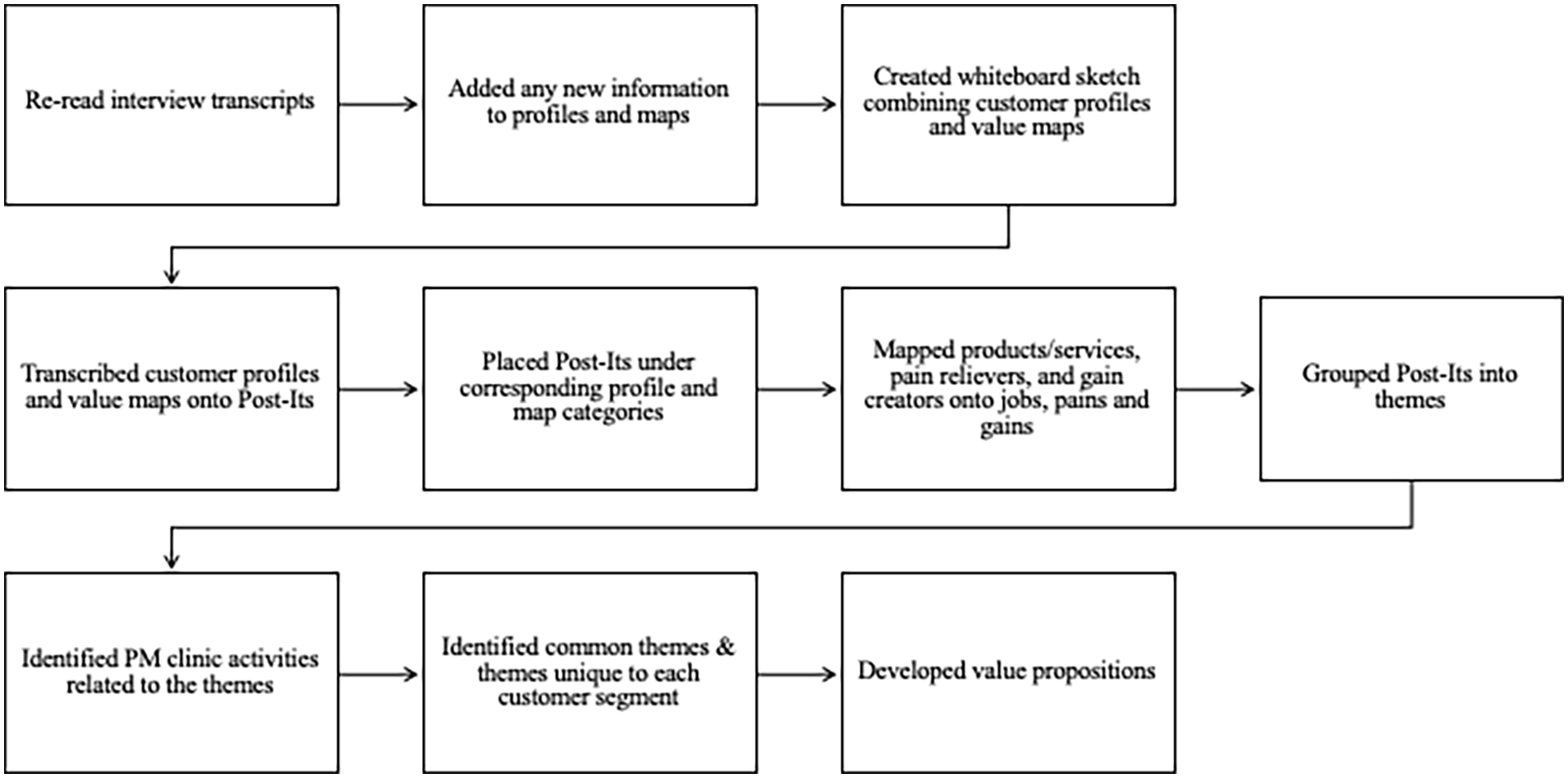
Process map of findings validation.
The second step of the verification activity consisted of a visualization exercise of the customer profiles and value maps using a white board and sticky notes for each customer segment (see Figure 5). The creators of the BMC (Osterwalder and Pigneur, 2010) recommend sketching out the canvas with sticky notes. This exercise allowed the research team to visualize and see how the various aspects of the BMC are related to each other and provided the opportunity to move the notes around and test different versions of the model to ascertain what version best aligned with and represented the data. Organizing the whiteboard in this fashion enabled the team to corroborate that the PM clinic was addressing the concerns raised by customers, and how the clinic would address each of the identified concerns. Each finding from the customer profile and value maps was recorded onto single sticky note, and each note was placed under its corresponding category. Then, the sticky notes were analyzed and grouped into themes (e.g. funding, human resources, workflow).
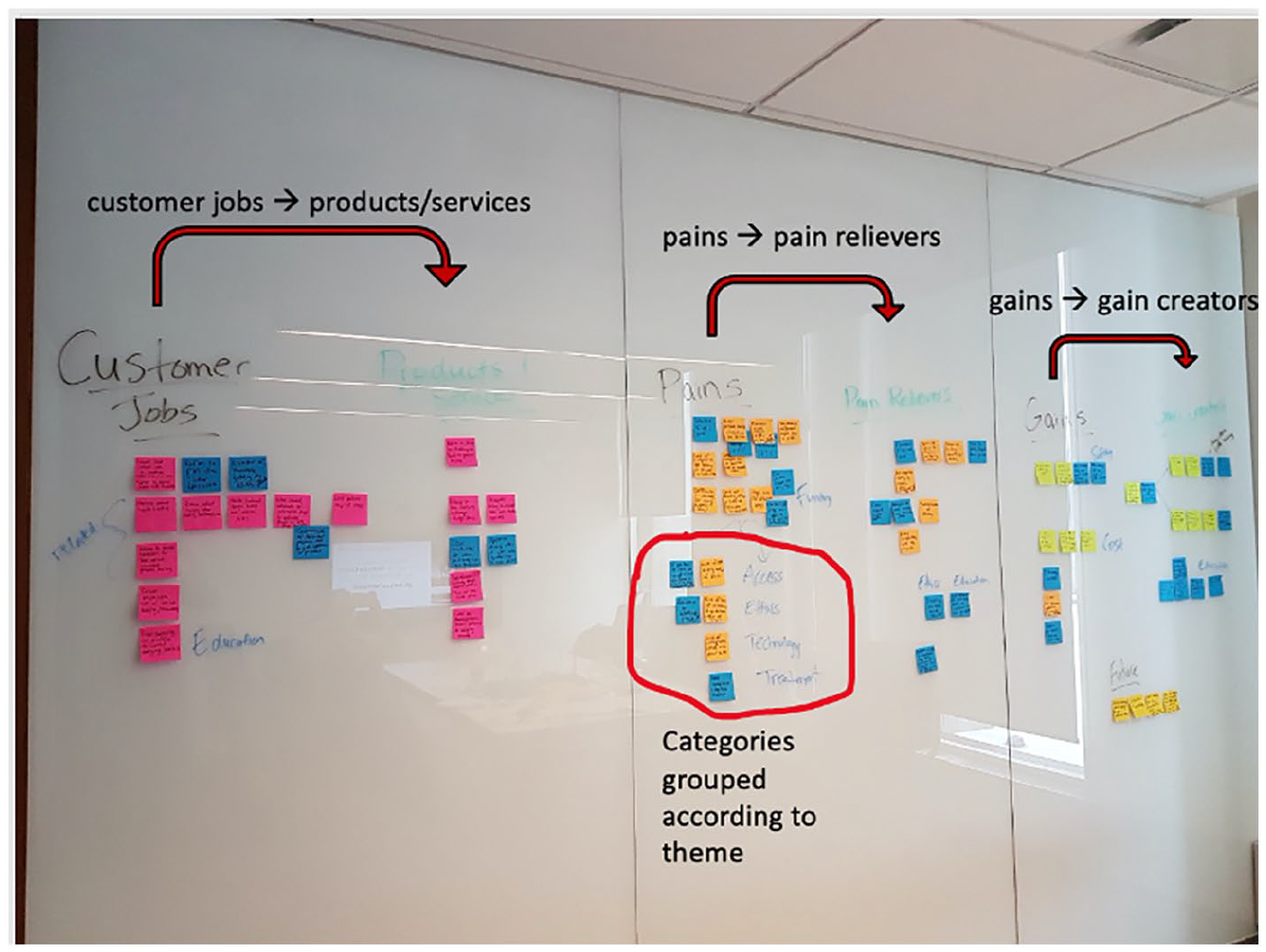
Whiteboard sketch of a customer profile and value map.
After themes were identified, the team reflected on which parts of value maps addressed the themes (see Figure 6). For example, education was a major theme with physicians reporting both a lack of knowledge about PM and the PM clinic in general. As a result, one of the pain relievers was to create education resources for physicians. Visualizing the interview data and analyzing how the interview data related to the components of BMC was another form of crystallization the research team used to enhance the credibility of the research. The team was able to generate a more nuanced understanding of physician needs and the clinic’s capabilities to meet those needs by physically mapping and matching aspects and services of the clinic that met specific customer needs. As well, merging and visualizing the customer profiles and value maps and grouping themes together for each discipline enabled the team to identify concerns common to all customer segments as well as those unique to each segment. For example, all physicians were concerned with getting timely information related to patients’ susceptibility to experiencing ADRs in order to avoid delays in treatment, while gastroenterology-specific concerns included using the PM clinic test results to get patients access to drugs that require proof that the patients cannot tolerate an alternative drug. Being able to determine both common and unique needs of customers through the team activity generated a better understanding of each customer segment in order to determine the best ways in which the PM clinic could meet their needs through customization of standardized offerings and value propositions.
Aligning customer profiles and value maps.
Step 3: developing value propositions
The main themes and customer concerns identified through the team activity were used to develop the value propositions for the customer segments. This process involved briefly describing the services of the clinic and outlining the ways in which the clinic would address the most important needs of the customers. A common theme across all the value propositions was the clinic’s ability to maximize patient comfort and safety, which was a predominant concern important to all physician customers. The value propositions differed in terms of how the clinic would assist physician customers in meeting the needs of different patient populations. For example, the value proposition for oncologists focused on incorporating pre-emptive testing prior to starting chemotherapy into standard of care while the value proposition for gastroenterologists focused on demonstrating need for access to alternative drugs for patients. Validating the findings from the customer profiles and value maps prior to the value proposition development step enabled the team to identify both common and unique concerns in order to create some standardization of solutions, while maintaining the ability to customize value propositions for the various customer segments.
Discussion
The research team used the BMC (Osterwalder and Pigneur, 2010) to design value propositions for physician customers of a PM clinic that conducts PGx-based testing for ADRs. This article provides a detailed description of the processes used to understand the needs of the physician customers (related to medication prescription and management) and the ways in which the PM clinic could potentially address those needs to increase the demand for its service offering and the subsequent value created and captured through that service delivery. In addition, the article outlines how the customer profiles and value maps were integrated in a group activity to verify interview findings and create strong value propositions for each physician customer segment.
One of the strengths of the BMC is its iterative approach to value proposition design (Ching and Fauvel, 2013; Osterwalder and Pigneur, 2010). Users are able to continue add to and iterate the customer profiles until a sufficient amount of information has been collected about each customer segment. The application of this structured approach enabled the research team to compare interviews within and between customer segments and to revise interview questions as needed in order to collect as much relevant information as possible about physician’s views on the current state of medication prescription practices and where the PM clinic can provide value. In addition, the research team found the BMC to be an easy-to-use framework for data depiction, sorting, and analysis. Analyzing the customer interviews using the jobs, pains, and gains categories of the customer profiles provided a simple way of organizing the interview data and helped ensure that all the necessary information was captured as required for creating the value propositions. Based on the customer profiles, the research team was able to clearly outline how the PM clinic could address each physician segment’s respective concerns and articulate the benefits associated with engaging the clinic’s services.
Another strength of the BMC is the ability to acquire a more thorough understanding of a firm’s customers and their respective needs. The BMC helps achieve this understanding through its use of multiple customer interviews and the visualization of the model (Coes, 2014; Osterwalder and Pigneur, 2010). The research team’s immersion in, and analysis of, the data enabled an enhanced comprehension of the phenomenon under study. As more individuals were interviewed from each customer segment, recurring themes across segments were discovered, and the unique needs of each customer segment more clearly identified and understood. For example, while all physicians were concerned about the trial-and-error nature of medication prescription, oncologists’ related concerns were focused on delays in treatment. In comparison, psychiatrists were worried about patients not taking their medication and experiencing psychiatric symptoms because of the length of time and side effects associated with determining the correct dose. Visually depicting the customer profiles and value maps enabled team members to easily communicate the model to each other during the findings verification exercise (Coes, 2014) and permitting a more focused discussion on the most important customer needs and values, and how the PM clinic could address those for customers with its services. Visualizing the maps and profiles also allowed the team to clearly see where the offerings of the PM clinic aligned with customer needs and preferences. By gaining a comprehensive understanding of the customer segments using the BMC, the team was able to keep the characteristics of the various customer segments in mind at all times when designing their unique value propositions. Adherence to this method of understanding facilitated the creation of strong value propositions that resonated with customers (Payne et al., 2017).
Limitations
While the BMC was useful for understanding the needs of each physician group, there were some limitations to its use. First, the BMC does not include an analysis of the competition in its business plan development process (Ching and Fauvel, 2013; Coes, 2014). As a result, the team was unable to include questions about other similar services in our customer interviews and assess the likelihood of substitutions in the market. The lack of a competitive analysis, and the competitors’ attributes that would have been discovered, made it difficult to include information on the differentiating factors of the PM clinic (compared to other genetic testing services) in the value propositions. For example, there are some direct-to-consumer PGx tests available on the Canadian market where members of the public pay to have the DNA in their saliva analyzed for drug sensitivities and are sent a report with their results. The research team was unable to analyze the demand for these services by the public and how these services differ from the services provided by the PM clinic using the BMC. The research team was also unable to examine the PGx services provided by other health care providers or hospitals with the BMC. Although health care services are publicly funded in Canada, it is still imperative to understand how services differ between health care providers as this information can help identify the factors that will make physicians use one service over another. One of the most successful competitive strategies in business is the ability to provide better and unique value to the customer by differentiating one’s business from the competition (Kar, 2006). This strategy involves being able to demonstrate how one’s product/service is superior to, or improves upon, what is already offered to the customer by the competition. The ability to investigate the current market competition would have facilitated the creation of stronger value propositions, because the team would have been able to describe how the PM clinic could meet the needs of physicians in ways the current competition cannot.
A second limitation is that the BMC was intended to be used by entrepreneurs focused on profit generation (Coes, 2014; Osterwalder and Pigneur, 2010) and was not originally designed for use within non-profit sectors (e.g. Canadian hospital clinics). Many non-profit organizations base strategic decisions on their organizational mission statement, which is generally focused on the social value an organization aims to provide to its users (Coes, 2014). While social enterprises must still consider cost structure and revenue streams in their business models, their value-generating activities go beyond the traditional consumer-oriented business model and the focus on financial gain, and often occur outside of the business sector. This makes the BMC difficult to use for organizations whose main goal is something other than profit generation as the model does not incorporate social value into its value proposition design process (Coes, 2014). For example, the PM clinic under study in this article operates within a publicly funded health care system. Therefore, we had to adapt the model to be reflective of the PM clinic setting and its ongoing challenge of acquiring the requisite working capital associated with operating as a part of a public non-profit health care system. Another important adaption involved expanding the definition of customer beyond the traditional idea of those who purchase a good/service to be reflective of the health care sector. Customers were defined as individuals who decide whether or not a patient will use a health care service (i.e. referring physicians).
A third limitation is that the BMC does not incorporate external forces, such as economic or political forces, into its business model development (Austin, 2020). This restricts the ability to interpret how these external forces may impact the growth and development of a business. For example, interviews with gastroenterologists revealed how policies related to the prescription of biologics (i.e. drugs made from or containing components of living organisms) affected prescribing practices. Patients have to be treated with a non-biologic first, lengthening the amount of time needed to reach an effective treatment. By choosing the BMC as its principle tool, the research team was unable to address external factors like the policy described above in the customer analysis and value proposition development.
A fourth limitation of the BMC is that while it is lauded for its iterative and easy-to-use features, it lacks a formalized process for analyzing the data collected. The research team found it difficult to analyze the interview data in a systematic way without any guidance from the model. The BMC does recommend categorizing interview data into the components of the customer profiles (jobs, pains, and gains), but lacks directions on how to analyze and code interviews to develop customer profiles, and how to consolidate findings to develop value propositions. The research team found that relevant information regarding what physicians valued and needed at times did not always fit within the jobs, pains, or gains categories. While re-reading the interview transcripts and adding additional information to the profiles during the finding verification activity was helpful in ensuring all necessary information was captured within the model, the categorization of data into the designated categories was at times overly challenging. Finally, while this study provides insights into customers’ (physicians’) perceptions of value, the end consumers’ (patients’) perception of value is not the focus of this research. A study of patient perceptions will be a beneficial extension to this research.
Conclusion
This article demonstrates that the BMC is a tool that can be used in a health care setting and is worthy of greater consideration. Often, health care services are delivered without much consideration about how these services are experienced by the individuals using them. This is why the idea of framing services in terms of value generation is essential in health care. Health care administrators, leaders, and innovators must put more thought into the ways in which their organizations can deliver value for the people who access their services. This will not only help generate the best outcomes for patients but can also result in greater system efficiency and effectiveness (Porter and Teisberg, 2007).
The BMC places value at the forefront of business plan development. As the BMC was originally developed for entrepreneurs (Osterwalder and Pigneur, 2010), little information exists on how to use the principles of the BMC outside of a business setting. This article provides a detailed description of each of the steps of value proposition design as outlined by the BMC and provides recommendations for how individuals working in health care can use the BMC to learn what is most important to stakeholders when designing and implementing health care services. The article outlines how the research team developed and analyzed physician customer profiles and value maps to construct value propositions in pursuit of summarizing how the PM clinic could address customer needs and create value for physicians referring to the clinic. To our knowledge, this article is the first to provide a comprehensive overview of the methods involved in each of the steps of value proposition design. The article also discusses ways the BMC could be adapted for business model development within a health care setting.
The use of the BMC framework allowed the team to deepen its understanding of each customer segment, the importance of customizing the message to each segment, and the articulation of how the PM clinic could address some of the challenges each segment is experiencing. Through enhanced design of its value propositions and subsequent operationalization of its value delivery system, the PM clinic is better positioned for success.
In conclusion, the BMC stimulates thinking about how value is currently created and how it can be created and captured in the future. It also allows users to gain a thorough understanding of the individuals they are seeking to reach, serve, and delight. Broader utilization of the BMC framework can only help bring better clarity to customer needs, generate more value-added offerings, and create and capture more value for the health care system and the patients its serves.
Footnotes
Author’s Note
Mathushan Subhasri is now affiliated with McGill University in Montreal Canada.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.