
Abstract
Today, more and more problems that scientists need to tackle are complex problems. Many examples of these can be found in the health sciences, medicine and ecology. Typical features of complex problems are that they cannot be studied by one discipline and that they need to take into account subjective data as well as objective data. Two promising responses to deal with complex problems are Transdisciplinary and Mixed Method approaches. However, there is still a lacuna to fill, with transdisciplinary studies bridging the social sciences and biomedical sciences. More specifically, we need more and better studies that combine qualitative data about subjective experiences, perception and so on with objective, quantitative, neurophysiological data. We believe that the combination of qualitative and neurophysiological data is a good example of what we would like to call transdisciplinary mixed methods. In this article, we aim to explore the opportunities of transdisciplinary mixed-methods studies in which qualitative and neurophysiological data are used. We give a brief overview of what is characteristic for this kind of studies and illustrate this with examples; we point out strengths and limitations and propose an agenda for the future. We conclude that transdisciplinary mixed-methods studies in which qualitative and neurophysiological data are used have the potential to improve our knowledge about complex problems. A main obstacle seems to be that most scientists from the biomedical sciences are not familiar with the (qualitative) methods from the social sciences and vice versa. To end this ‘clash of paradigms’™, we urgently need to cultivate transdisciplinary thinking.
Introduction
Today, more and more problems that scientists need to tackle are complex problems. Examples of these can be found in many fields such as health sciences, medicine and ecology. Typical features of complex problems are that they cannot be studied by one discipline and that they need to take into account subjective data (e.g. the perspective of stakeholders) as well as objective data (e.g. biological measurements). Hence, multiple methodological approaches are needed, usually from disciplines with quite different epistemological assumptions such as the biomedical and the social sciences. To achieve a complete view on complex problems, an integrative approach is necessary (Brown et al., 2010). However, due to an exponential growth of scientific research, it is challenging to keep a broad view. To keep up with their field of expertise, scientists are forced to specialise into narrower domains that they try to master. A possible danger of this development is that science will become increasingly fragmented, with the doomsday scenario of experts knowing more and more about less until they ‘know everything about nothing’ (N.M. Butler). In recent decades, many scientists have become aware of this pitfall and solutions have been proposed to cope.
Two of the most promising responses to this challenge are the development of transdisciplinary research (Brown et al., 2010; Hirsch Hadorn et al., 2008; Leavy, 2016; Nicolescu, 2008) and mixed methods (Greene, 2007; Tashakkori and Teddlie, 2003). However, as researchers in the field of health and medicine, we believe that there is still a lacuna to fill, with transdisciplinary studies bridging the social sciences and biomedical sciences. More specifically, we need more and better studies that combine qualitative data about subjective experiences, perception and so on with objective, quantitative, neurophysiological data (NPD). We believe that the combination of qualitative and NPD is a good example of what we would like to call transdisciplinary mixed methods (tMM). This specific form of mixed-method research has great potential to provide new insights and to advance research towards innovative discoveries.
In this article, we aim to explore the opportunities of a specific kind of tMM studies in which qualitative and NPD are used (or tMMNPD for short). We will give a brief overview of what is characteristic for tMMNPD and how it can be used. We give some examples to illustrate its potential; we point out strengths and limitations and propose an agenda for the future advancement of tMMNPD.
tMM: main concepts and assumptions
Before we focus on tMMNPD, we first need to clarify two main concepts on which it is built: transdisciplinary research and mixed methods (see Figure 1).

Overview of paradigms, disciplinary and methodological approaches on which tMMNPD is grounded.
Transdisciplinary research
In a reaction to the restrictions of the disciplinary approach when dealing with complex problems, multidisciplinary, interdisciplinary and transdisciplinary approaches emerged. Although these are sometimes used as synonyms, they each have a specific meaning (Brown et al., 2010). Multidisciplinary refers to research in which people from different disciplines are working together, each drawing on their disciplinary knowledge (Stember, 1990).
Interdisciplinary can be defined as collaboration between two or more disciplines with varying levels of integration of concepts, theories, methods and findings (Leavy, 2016). However, for some authors, this implies a real synthesis of approaches (Stember, 1990) while according to Brown et al. (2010), specialists remains within their discipline.
Transdisciplinarity concerns that which is at once between disciplines, across the different disciplines and beyond all disciplines. Its goal is the understanding of the present world, of which one of the imperatives is the unity of knowledge (Nicolescu, 2010). Its contribution enables cross-fertilization of ideas and knowledge from different contributors to promote an expanded vision of a subject as well as new explanatory theories (Stokols, 2006).
The main principles of transdisciplinarity are described in the Charter of Transdisciplinarity, adopted at the first World Congress on Transdisciplinarity (Nicolescu, 1994). The charter has been published as a reaction to the ‘increasingly quantitative knowledge and increasingly impoverished inner identity’ and the threats of ‘the triumph of a techno-science that obeys only the terrible logic of efficacy of efficacy’s sake’ (Nicolescu, 1994). It states that reality cannot be reduced to a single level governed by a single form of logic. Leavy (2016) states that the key principles of transdisciplinarity include a problem-centeredness, holistic or synergistic approach, transcendence, emergence, integration, innovation and flexibility.
According to Nicolescu (2010), transdisciplinarity is based on three main postulates. First, there are different levels of reality, each governed by different types of logic. From a transdisciplinary point of view, complexity is a modern form of the very ancient principle of universal dependence. A methodological implication is that mathematical languages exclusively address the analytical mind, while symbolic languages address the whole of the human being, with its thoughts, feelings and body. Second, many problems, and especially those that are crucial for the survival of humanity, are complex. The third postulate states that the axiom of classical logic that does not tolerate contradiction (something cannot be A and non-A at the same time) needs to be replaced by the logic of the included middle. According to that postulate, it is possible that both A and non-A are true. Hence, there is a third term (T) which is simultaneously A and non-A. Several examples can be found in quantum mechanics where there is experimental evidence of exclusive contradictions (A and non-A): wave and corpuscle, continuity and discontinuity (Nicolescu, 2010).
Transdisciplinarity does not deny the importance of disciplinary research; it is rather complementary to it. Transdisciplinarity is resolutely open and goes beyond the field of exact sciences, demanding their dialogue and reconciliation with the humanities and the social sciences, as well with art, literature, poetry and spiritual experience. Spirituality has to be understood in the (new) sense as an endeavour to conciliate techno-science and wisdom. Transdisciplinarity is also inherently transcultural and states that no single culture is privileged over any other (Nicolescu, 2010).
A problem is that ‘transdisciplinary research’ is defined in different ways, and there is little consensus about it (J Jäger in Hirsch Hadorn 2008; Leavy, 2016). Some consider it as a synergistic collaboration between disciplines within the broad domain of social research (Leavy, 2016). However, we believe that the approach should not be limited to the domain of social sciences and that it may include disciplines from the biomedical sciences (and probably a lot of other sciences) too.
Mixed-method research
Mixed-method designs are those which use methods from at least two different paradigms, typically, a qualitative and quantitative method (Leavy, 2016). Scientists are usually trained in either the quantitative or qualitative paradigm. This is especially the case in medicine, where most doctors and biomedical researchers have hardly heard about qualitative methods. Quantitative and qualitative methods have often been considered to be grounded in two fundamentally different paradigms. Quantitative methods are associated with positivism, which was, until late in the 20th century, the dominant paradigm with its epistemological tenet that the world can be described objectively and independent of the observer. In contrast, qualitative methods were based on interpretativism, a quite different view that the world is not independent of the observer and that reality is constructed or co-created in an interactive way by the researcher and the subjects of the study. These two opposite stances have been considered incompatible approaches for decades, which some have referred to as the ‘war of paradigms’ (Gage, 1989). Fortunately, in recent decades, this unproductive point of view has been increasingly abandoned. Indicative of these changes is, for instance, the fact that even in typically ‘hard sciences’ such as quantum physics, it has become evident that the observer plays a crucial role. At the same time, it has become evident that, to fully understand typical psychosocial topics such as emotion, perception, decision-making, other disciplines such as neurosciences are essential. Ethnographic studies showed that the alleged watershed distinction exists only in the minds of these people (Latour and Woolgar, 1986). Hence, the water is not as deep as some more theory-oriented epistemologists have argued. There are bridges between the two paradigms, and one of the main expressions of that evolution is the increasing number of mixed-method studies.
tMM
As we understand and use it, tMM builds further on the two above approaches that aim to formulate a response to the challenges posed by complex problems (Figure 1). Hence, tMM is a specific methodology that incorporates the principles of transdisciplinary and mixed methods. As a third characteristic, typical for tMMNPD, it includes objective as well as subjective assessments and thus bridges the domains of natural/biomedical sciences and the social/human sciences. Although subjective assessments, for instance, patients’ perspectives on the use of medicines, can be achieved with both qualitative and quantitative methods, qualitative approaches are particularly suitable for providing an in-depth view that also optimally includes the contextual factors. For objective assessments in health-related domains, NPD are well suited. This combination of subjective and objective assessments provides us with a more complete view than merely qualitative or quantitative data.
We believe that this area of research is especially underdeveloped due to scientists’ unfamiliarity with both domains. However, we have now arrived in a time that this area is especially promising because, in the past, most problems that were successfully tackled were the less complex problems that could therefore be resolved by the more traditional (reductionist, disciplinary) approaches. However, the more complex problems we have, or ‘wicked problems’ as Brown et al. call them, the more we need a tMM approach.
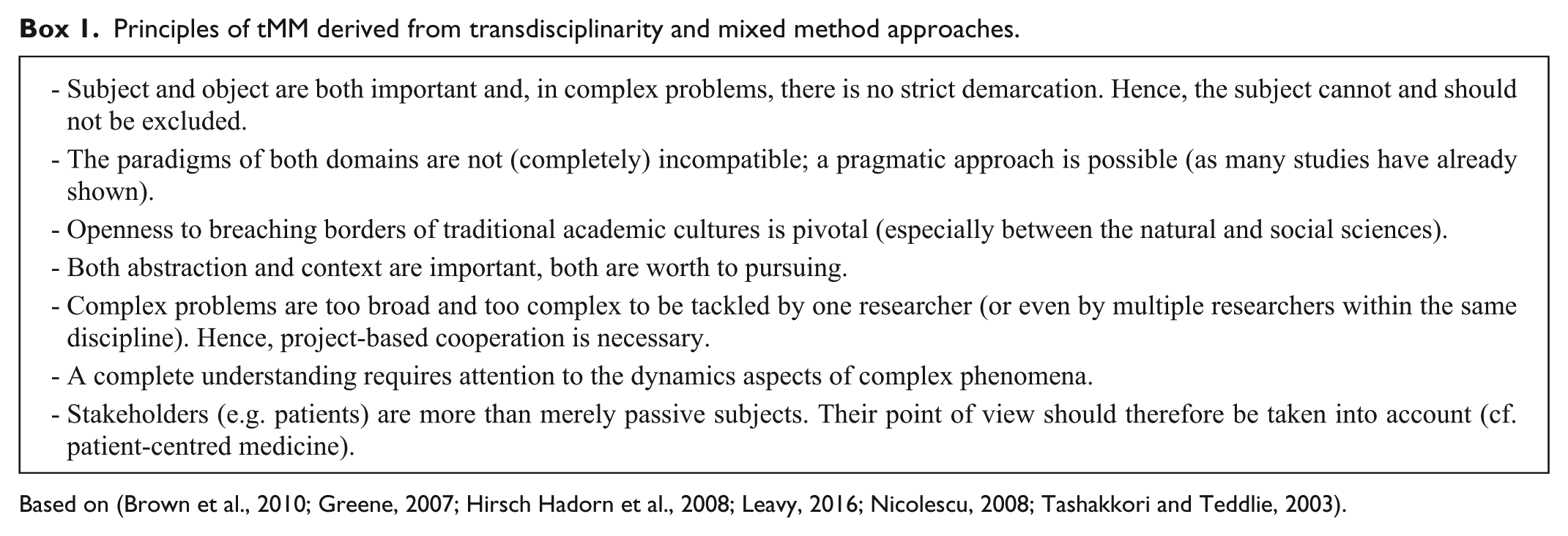
Since tMMNPD builds on the principles of Mixed Methods and Transdisciplinary approaches, its main assumptions are in line with these philosophical assumptions. Box 1 gives a concise overview of the main assumptions that are central to tMM in general and hence also to tMMNPD.
Principles of tMM derived from transdisciplinarity and mixed method approaches.
How can qualitative and NPD be combined?
There are several ways in which qualitative and NPD can be combined, and as with classical mixed-method studies (Tashakkori and Teddlie, 2003) some kind of classification is useful to specify which kind of research design is used. However, rather than proposing a clear-cut typology, we suggest a classification based on three dimensions, onto which we can map each study. The three main dimensions are dominance, sequence and integration. It is good to be aware of this because there are some important methodological consequences. We will give a concise overview of possible research designs here, illustrate them with an example and point out the methodological consequences.
Dominance
NPD as an aid for qualitative research
A first possible study design is one in which qualitative data are dominant and NPD serve as an aid. In this case, NPD is used to enrich contextual information by providing non-verbal information during a qualitative study. Non-verbal data, such as facial expression or other kinds of body language, may be helpful to clarify the specific meaning of what is said, reveal its emotional impact or uncover possible ambivalence or contradictions. Therefore, qualitative researchers are urged to pay attention to all kinds of non-verbal cues (Fontana and Frey, 2005; Marcinowicz et al., 2010). Although non-verbal data are an important source of information, which may improve validity, its use falls prey to several shortcomings.
A main problem is that many of the non-verbal cues are simply not noticed by the researcher, especially the more subtle facial or bodily reactions. One way to deal with this problem is to use video recordings which may enhance precision and reliability. However, very often emotions are not clearly expressed. Typical examples are feelings of sorrow or shame, or feelings of being hurt or irritated. Such feelings are often considered by the interviewee as ‘inappropriate’ or incompatible with their role or person and therefore hidden (cf. the ‘stiff upper lip’ or stoical attitude). There are also substantial cultural, gender and individual differences between people with regard to the expression of personal emotions and body language. In addition, coding these gestures when they are noticed is open to interpretation biases.
The shortcomings mentioned above, may be overcome by the use of additional non-verbal information from another origin and by not depending on an interviewer’s observational skills but using registration by devices as a complement. For many years, several neurophysiological parameters such as galvanic skin response (GSR), heart rate variability (HRV) and electroencephalography (EEG) have been known to be indicators of typical feelings or mental states such as fear, anger, stress, pain, lack of attention or their more positive counterparts (Du and Lee, 2014; Guntekin and Basar, 2014; Jatupaiboon et al., 2013; McCraty et al., 2009; Murugappan et al., 2013; Panksepp, 2003). NPD may therefore provide information that might enhance a more complete and context-sensitive understanding of what participants are saying (during interviews) or how they behave (during observations).
A second application of NPD as an aid for qualitative research is its use in situations where communication is difficult or even thought to be impossible. A very challenging situation, in which such an approach has already been proved to be useful, exists in people who are in what is now called a minimally conscious state. These people are completely unable to speak or to react with any kind of movement and are often mistakenly diagnosed as ‘vegetative’ patients (Cruse et al., 2011; Monti et al., 2010). However, with the use of a brain-computer interface (BCI), some of these patients could answer simple ‘yes or no’ questions. To answer a question with ‘yes’ they had to imagine they were playing tennis. This activated specific brain regions, which could be detected with EEG. This technique could be used to explore the quality of life of these patients (Bruno et al., 2008; Monti et al., 2010). Although such rudimentary ‘yes or no’ answers are typical of quantitative studies, a more qualitative approach is possible too, as illustrated by Jean-Dominique Bauby, the editor-in-chief of the French magazine Elle. Bauby had a severe stroke that resulted in locked-in syndrome; patients in such an unfortunate situation are physically paralysed but mentally fully aware. Bauby (1998) could only blink his left eye and used this to dictate a book letter by letter, using a technique called partner-assisted scanning. This provided an exceptional inside perspective of what locked-in patients’ experience. With the aid of EEG and BCI, the same technique should in principle be applicable in persons with total locked-in syndrome (unable to blink) or even in people in a minimally conscious state. Although this is of course very challenging, new BCI applications quickly push back the boundaries of what is possible. Although still in an experimental stage, such ‘mindreading’ based on a special kind of EEG is becoming possible. In a remarkable study, Pasley et al. (2012) took advantage of neurosurgical procedures for the treatment of epilepsy to measure neural activity directly from the cortical surface (known as electrocorticography). By measuring neural activity, they were able to decode individual words (Kaku, 2014; Martin et al., 2014; Pasley et al., 2012). At present, this is only possible after invasive procedures. However, EEG-based typewriters (for which no invasive methods are necessary) are already available (Hohne and Tangermann, 2014). It has also become possible to categorise images a person is thinking about and to search such images on the Internet guided by mental imagery (Naselaris et al., 2015; Stansbury et al., 2013).
Although the above examples are mixed-method studies, there is clearly a dominance of qualitative data and hence of the qualitative paradigm. Therefore, these studies can be mainly evaluated as qualitative studies and according to the standard criteria for qualitative studies (Tashakkori and Teddlie, 2003).
Qualitative data as an aid for neurophysiological research
On the other hand, there are also studies possible in which qualitative data can serve as an aid, and hence, in which NPD are dominant. An example of such a design would be the study of the objective and subjective effects of meditation. Several studies have shown how meditation has a profound effect on neurological and physiological parameters (Singh and Telles, 2015). Equally multiple qualitative studies have also explored the subjective experiences of meditators (Ando et al., 2011). However, a bibliographic search in PubMed did not provide any studies that aimed to link the subjective experiences with EEG.
Although many of such applications might improve our understanding of mind–body interaction, a promising research domain, these designs are not often used and if they are, the researchers are too often unaware that they are (to some degree) conducting a tMM study, simply because they are not trained in qualitative research and vice versa.
Sequence
Consecutive use: NPD followed by qualitative data or vice versa
Typical for these studies is that NPD are collected first, followed by a qualitative phase, usually in the form of a semi-structured interview. A typical application is to study stress. Nowadays, the physiological effects of stress can be measured with small sensors that are, for instance, integrated into a wristwatch or they can be attached to the body with a patch, an application known as carewear. It is then possible to monitor signs of stress over a relatively long time (for instance, a few hours). The result is usually a graph displaying when stress peaked or when recovery took place, for instance. In a consecutive qualitative interview, the researcher can then probe in-depth into what evoked this stress and why certain situations are stressful. The NPD can inform us when stress happened and the qualitative data can inform us more about why it happened.
The combination of NPD with qualitative research is especially fruitful because very often NPD can only be interpreted correctly when the context has been fully taken into account. Relying only on graphs and indexes entails a serious risk of misinterpretation. Therefore, neurophysiological and qualitative data are genuinely complementary in such cases, making both indispensable for an in-depth and correct understanding and evaluation in people.
An example of a consecutive design starting with qualitative data is in the study of the experience of dementia. Today, we have qualitative studies of what patients with dementia go through (Edvardsson and Nordvall, 2008), but these are limited to the early stage of dementia for the obvious reason that patients with severe dementia can no longer be interviewed. We also have biomedical studies of neurophysiological changes in the severe stages of dementia, but we do not know what these patients experience (or even if they are able to experience anything at all). An example of a tMM study could be to start in early dementia with both qualitative and NPD, until communication becomes impossible, and then to continue with NPD collection alone. Nowadays, machine learning is becoming a powerful tool that can be used to let the computer learn how subjective experiences (e.g. pain, happiness) are reflected in neurophysiological signatures. After this ‘learning’ phase, once communication has become impossible, the computer is still able to make ‘statements’ about subjective experiences based on neurological assessments (Brown et al., 2011).
Concurrent designs: simultaneous use of qualitative data and NPD
Another way of combining qualitative and NPD is a form of tMM in which both types of data are collected at the same time and are equally important. Inherent to this is the idea that the findings based on the combined data provide richer insights that could not be achieved by analysing the data separately: the findings are on a higher level because the whole is greater than the sum of the parts.
An example is COMPAS (COMfort during PAlliative Sedation), a study by our team that is currently underway, on the experiences of pain and discomfort during palliative sedation. It is assumed that patients who are sedated according to the current standards of care are unaware of their clinical situation and therefore do not experience symptoms of discomfort such as dyspnoea, delirium and other distressing conditions that are common during the terminal phase. However, a critical evaluation based on more recent evidence raises the question of whether the current assessments of suffering and awareness are accurate enough (Deschepper et al., 2013). The existing studies on the efficacy of palliative sedation to relieve pain and discomfort are almost exclusively based on observational assessments by caregivers. Although some efforts have been made to validate the observational scales, all these attempts are based on the same paradigm, which is that all kinds of distress in all patients can be measured by observation of the patient, and that this is the only available method in palliative care. In recent years, neurophysiological assessments based on EEG and electrocardiography (ECG) have been proved helpful in detecting pain and awareness. We therefore started a transdisciplinary study in which we concurrently collect qualitative data and NPD in 30 palliative sedated patients. From the start of the palliative sedation until they die, we continuously monitor brain activity (to minimise the burden for the patient and family we only use a simple kind of EEG-based assessment with three electrodes on the forehead) and HRV (with three electrodes on the chest) in combination with video observation (to detect visual signs of awareness and discomfort), visual analogue scales on which doctors, nurses and family members indicate their assessments and some commonly used scales for pain in non-communicative patients.
Integration
Although all the studies above are examples of mixed-method studies in which qualitative data are combined with NPD, they differ in the degree of integration of the methods. In the first examples (sub-section ‘Dominance’), integration is rather limited and hence these studies do not fully adhere to the principles of transdisciplinarity and mixed-method research.
It has to be remarked that full integration is not a condition sine qua non to achieve high-quality studies. Sometimes studies with less integration may be excellent multi- or interdisciplinary studies. However, according to Leavy (2016), the degree of integration is determinative to consider a study either as multidisciplinary, interdisciplinary or transdisciplinary. A transdisciplinary approach stimulates methodological integration, and in their best execution, each method informs the use of the other methods (Hesse-Biber, 2011). Therefore, high levels of integration are fostering the development of new conceptual, theoretical and methodological frameworks (Brown et al., 2010). The basic concept of integration is also that it maximises the strengths and minimises the weaknesses of each type of data (Creswell et al., 2011). Therefore, we believe that optimal integration through the use of systematic integrative procedures is an important aim in tMMNPD.
In the COMPAS study, a high degree of integration is possible only because researchers from different disciplines (palliative sedation, neurology, psychology and medical anthropology) were involved from the very beginning (problem statement and study design) until the end. Also members of the palliative community and lay people (patients and their family) were involved, for example, to agree on what is ethically and practically acceptable, especially with regard to the collection of NPD and video observation.
Some potentially useful physiological and neurological indicators
The types of data used in qualitative research are well-known: unstructured data based on individual interviews, focus groups, observations or already existing documents or audio-visual material. Furthermore, there is ample guidance on how to optimally collect, analyse and interpret these data (Strauss and Corbin, 1990). For NPD, this is less evident. Some indicators have been used for many years for purely biomedical purposes while others are newer and their meaning is less clear.
A main assumption on which neuropsychological assessments are based is that every change in emotional or cognitive state will be echoed in physiological parameters, and hence can be measured. This assumption reflects a type of logical positivism and is at the heart of the domain of psychophysiology. According to the kind of emotional states, cognitions or behaviour, one or more physiological indicators should be deliberately chosen, reflecting a body system (e.g. sympathetic nervous system), which mediates such psychological changes.
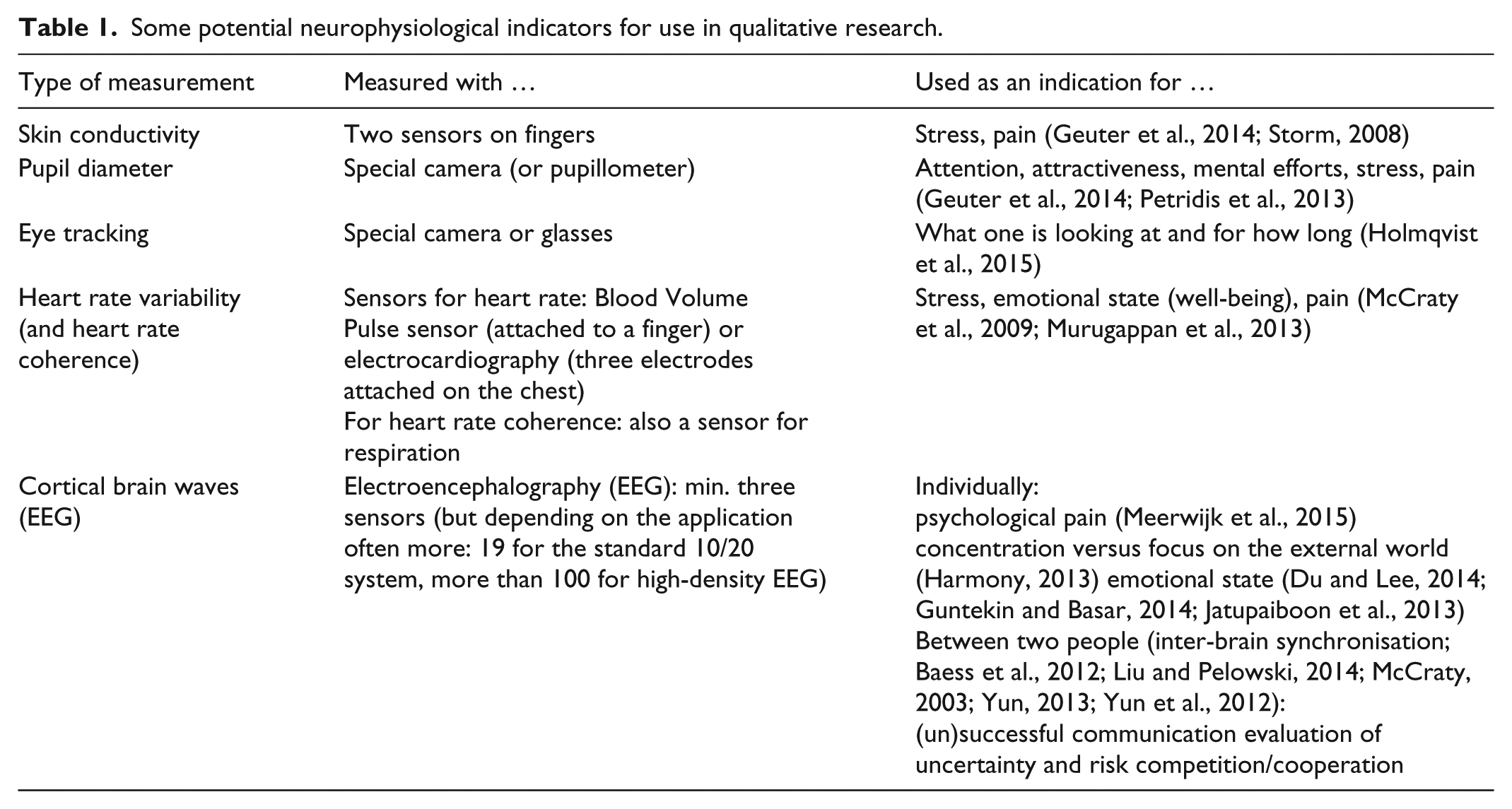
In Table 1, we present some potentially useful examples of non-invasive neurophysiological indicators for use in tMM studies, but this is not an exhaustive overview by any means. Furthermore, the field of applied psychophysiology is rapidly developing and new indicators, registration methods and applications are becoming available.
Some potential neurophysiological indicators for use in qualitative research.
GSR, also referred to as skin conductance, is an indicator often used for stress detection as its activity reflects sympathetic responses (Tulen et al., 1989). GSR can be easily measured by two sensors that are attached to the fingers and may provide real-time data, for instance, in the form of a graph, indicating stressful moments. This is probably one of the simplest neurophysiological indicators for qualitative research. However, GSR lacks specificity because elevated levels of GSR are not always the result of stress, since other factors (such as temperature) may also result in an increased GSR (Bakker et al., 2011). Therefore, more recently, pupillometry has been proposed as a more effective and robust parameter for detection of stress (Ren et al., 2014).
Pupillometry is the assessment of the diameter of the pupil. Pupils react not only to changes in intensity of light but also to arousal and emotions. Pupil dilatation is caused, for instance, by pictures or persons that are perceived as (sexually) attractive. More generally, pupil dilatation reflects activation of the brain and also reflects increases in the difficulty of mental tasks (Hess and Polt, 1964). Another study found that pupil diameter increased when viewing emotional pictures, regardless of their valence, and that this correlated with GSR, suggesting that pupil diameter increase is sympathetically mediated (Bradley et al., 2008). It can also be used for the detection of pain, for instance, in non-communicative patients (Ren et al., 2014). Pupil dilatation can now easily be measured with special glasses or cameras, even in an unobtrusive way (Petridis et al., 2013).
Another technique that has many interesting applications is eye-tracking. It provides information about what people are looking at and can help show what attracts people’s attention. It can be used during interpersonal interactions or while looking at objects, reading documents and so on. It is usually used in combination with video registration and results may be presented as dots on images being watched. The larger the dots are in a certain location, the more attention participants have been giving to a certain spot. Heat maps are also possible for presenting global results of multiple viewers (Holmqvist et al., 2015).
HRV is a measure of the degree of change in the normal beat-to-beat intervals. It is mostly a measure of vagal nerve activity, and it correlates highly with actual activity of this nerve (Kuo et al., 2005). According to a recent review, HRV may be a reliable indicator of changes in the emotional state of subjects and provides an approach to a real-time emotional assessment system with a higher reliability than other systems (Murugappan et al., 2013). A reduced HRV was found to be associated with emotional strain and elevated stress (Chandola et al., 2010). A meta-analysis showed that several areas in the brain, including the amygdala and the medial prefrontal cortex, involved in perceptions of threat, emotional regulation, safety and decision-making, are also associated with HRV (Thayer et al., 2012). HRV is related to breathing.
One interesting application of HRV has been its use as a moderator, where it differentiates among people who recover from slowly versus fast from social stress, according to indexes reflecting multiple physiological systems (Weber et al., 2010). Here, the context and timing are the qualitative aspect while the NPD reflect the quantitative aspect of tMM. Taking together, HRV is a simple and powerful non-invasive parameter with a lot of potentially useful applications, also for qualitative and clinical researchers.
Measurement of both HRV and breathing frequency, which reflects the degree of heart rate coherence, may provide information about the emotional and cognitive state of people. McCraty et al. (2009) found that HRV was directly associated with the subjective activation of distinct emotional states, and that HRV is mostly directly related to emotional states. They identified six distinct heart rhythm patterns that are generated during different emotional states. One of these states, labelled ‘Psychophysiological incoherence’, is associated with negative emotions such as anger, frustration and anxiety. Conversely, another state called ‘Relaxation’ is a state of emotional calm. These states are dynamic and can be influenced by internal and external factors. Since positive emotions, such as appreciation, care and kindness, also proved to have an impact, these states can (unwittingly) be influenced by the interviewer and monitored during the interview (Figure 2). Besides ordinary feelings, hyper-states of extreme negative emotions are possible to detect in a similar manner. These are associated with unpredictable, destructive behaviour directed either at oneself or projected onto others. Such situations may be encountered more in research with specific populations such as patients with certain psychiatric disorders. In these cases, extra caution is required with regard to the circumstances and topics of the interview.
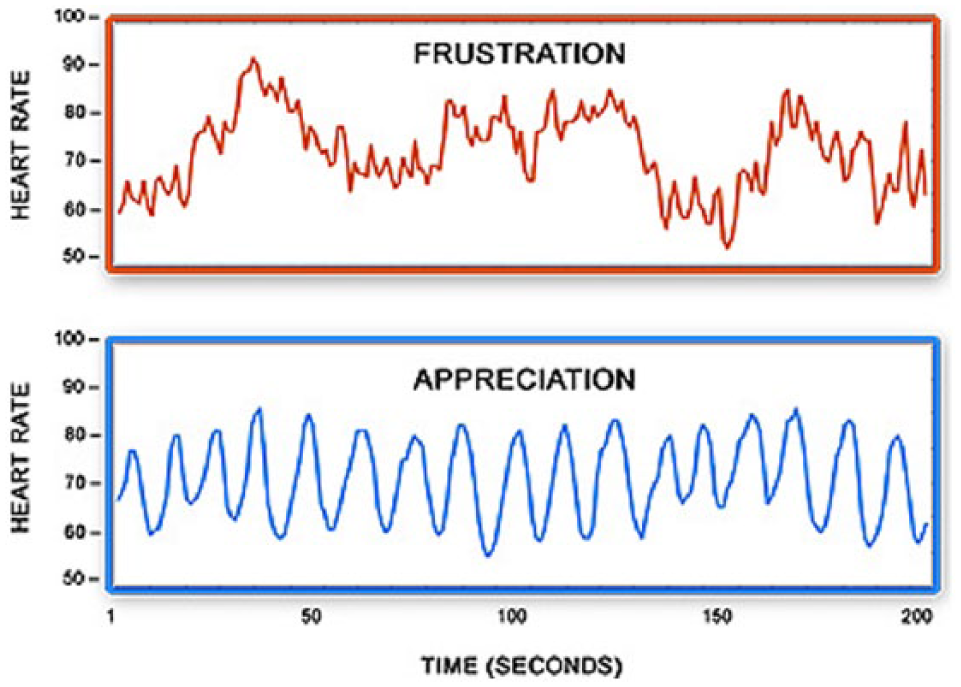
Frustration and appreciation (McCraty et al. 2009).
Another application is EEG. In the past, this procedure was logistically complex due to the placement of the electrodes on the scalp and still remains rather complex in terms of interpreting the results of the measurements. Thanks to more user-friendly headsets and the development of digital EEG, this has now become relatively easy and can be administered by trained (qualitative) researchers. Great progress could be made by the use of software which enables quantitative electroencephalography (qEEG) analysis. This permits subtle patterns to be detected, which in the past went unnoticed by visual inspection, even by experienced neurologists. EEG has a high temporal resolution and therefore detects changes in cortical activity rapidly. Besides the use of EEG in persons unable to communicate as already mentioned, EEG can be used to inform us about the cognitive state of the participant and his or her degree of arousal. EEG waves are usually classified according to their frequency.
Alpha waves (8–13 Hz) can be indicative of being relaxed and alert, and are associated with focused attention. Alpha waves cannot exist alongside anxiety or aggression. Beta waves (14–37 Hz) are typically found when someone is active or busy and they increase when someone is afraid, angry or wants to flee. Theta waves (4–8 Hz) are associated with creative and relaxed thinking but are also indicative of drowsiness. Gamma waves (38–80 Hz) can sometimes be observed during intense mental activity. Delta waves (<4 Hz) are related to deep sleep. Besides the frequency of the EEG waves, several other characteristics, such as the specific brain regions where they are produced, synchronicity and hemispheric lateralisation may provide information about the cognitive or emotional state. Alpha waves in the left frontal lobe indicate emotions such as positive affect and anger, while high electrical activity in the right frontal lobe is correlated with withdrawal emotions such as anxiety and depressive feelings (Jesulola et al., 2015; Morins, 2011). Furthermore, during stress, people shift from left to right frontal activity measured by EEG, and the degree of this shift positively correlates with self-reported illness (Lewis et al., 2007).
An innovative EEG application is inter-brain synchronisation between two or even more persons. In a few studies, synchronisation of specific regions in the brain were found to be typical of specific modes of interaction such as successful face-to-face communication, cooperative versus competitive interaction, or risk evaluation (Liu and Pelowski, 2014). Such research can provide crucial neurophysiological insights into human interaction.
It is of course also important to determine how such measurements need to be done, for instance, with regard to the number and place of the EEG electrodes, which are dependent on the specific applications. However, some quite simple applications exist as well, even with no more than three electrodes, as often used in neuro-feedback, or with a wireless 14-channel headset, as used in a study on the real-time measurement of happiness (Jatupaiboon et al., 2013). The interpretation of EEG data remains a critical issue and should be done carefully. Although EEG is a well-established technique, some applications are quite new and need further validation.
Other neurological measurements currently used are hemoencephalography (HEG), which measures the (relative) blood flow inside the brain, and Loreta, a technique based on EEG which calculates a 3D image of the relative activity of the brain. New neurophysiological indicators and applications are being developed at a great pace.
Very often a combination of different techniques and indicators is used and for some parameters such as heart rhythm coherence, measurement of two variables (heart rate and respiration rate) is required. Our overview is not exhaustive, and we have limited it to small instruments that are in principle accessible for most interested researchers. Hence, we have not included very powerful applications such as functional magnetic resonance imaging (fMRI), which require (extremely) expensive devices and highly specialised experts.
The wicked problem of validation
An important aspect of quality of tMMNPD studies is related to the validation. There are two important rules to keep in mind.
The validity of a tMMNPD study depends on the validity of the tools of the separate methods of the respective disciplines. If these are weak then results of tMMNPD study will probably also be weak.
tMMNPD is an approach that may enhance validity because of three principles that are inherent to it: (a) involvement of multiple disciplines, (b) the role of subjects, and (c) involvement of stakeholders (Brown et al., 2010; Nicolescu, 2010; Yeasmin and Rahman, 2012).
The involvement of multiple disciplines is some kind of methodological triangulation (Leavy, 2016). Therefore, the results of tMMNPD studies are based on multiple paradigms (from the ‘exact’ and the ‘social’ science) that are used to check one another. Subjects (e.g. patients, family members …) are actively involved by taking, as much as possible, their perspective into account. Hence, the findings of the researchers are confronted with the experiences and opinions of the study subjects. Or in other words, the objective reality is checked by the subjective reality. tMMNPD studies stimulate involvement of stakeholders, that is, people from the broader communities for which the results are relevant (e.g. representatives of organisations for which the study findings are relevant such as patient organisations, professional or societal groups). This enhances external critical reflexivity, that is, not limited to the scientific community, which can be considered as a kind of ecological validation.
The above-mentioned problem of assessment of pain in palliative sedation is a good example of a ‘wicked problem’ for which validation of the assessment is a critical issue. Comfort in palliative patients is cause for concern exactly because of the lack of validation of the current assessments. Pain assessment in palliative care is based only on a subjective (qualitative) assessment of observable signs of pain, a method that is congruent with the paradigm of palliative medicine that values a non-technical approach to relieve suffering in which empathy is central. In neurology and anaesthesiology, to the contrast, doctors tend to rely only on neurophysiological assessments because this provides objective assessments through the use of EEG-based monitors used in anaesthesiology. However, both approaches have been criticised because of doubts about the validity of their assessments (Deschepper et al., 2013; Sackey, 2008). The issues of reliability and validity are at the heart of these two approaches, since one could argue that while the reliability of quantitative methods is high, their validity (meaning of what is measured) can be questioned. In contrast, the (face) validity of qualitative methods is clearer while they obviously lack reliability. As such, they are complimentary (Yeasmin and Rahman, 2012). Methodological triangulation in tMMNPD can therefore be considered as a way of transdisciplinary cross-validation in which multiple imperfect methods from different disciplines are used to achieve the best possible validation. We are therefore convinced that a tMMNPD approach may be the best way to validate the currently used tools for assessment of pain in palliative (and other non-communicative) patients.
Hence, because assessments based on both approaches are imperfect and since we do not have a golden standard, also tMMNPD approaches are limited (rule 1). However, while the limitations of tMMNPD should be acknowledged, it is precisely using a tMM approach, that validation can be improved (rule 2). The fact that this is currently often overlooked is, in our view, mainly due to the total unfamiliarity of scientists from the ‘exact’ sciences with the methods of the ‘soft’ social sciences and vice versa (Leung, 2015).
Ethical aspects
A tenable account of transdisciplinarity knowledge requires attention to the ethical aspects (Russell in Brown et al., 2010). In tMM research, the combination of NPD and qualitative research provides researchers with a powerful tool to probe into the heart and mind of the participant. Compared to ‘ordinary’ qualitative interviews or observations, participants become much more of ‘an open book’ for the researcher. Since some of the NPD also correlate with emotional and cognitive changes, it is often impossible for participants to hide their feelings, and even their thoughts and intentions. The use of NPD in combination with open questions comes very close to an application that has been used in criminology for several decades: the polygraph (lie detector). The researcher thus gains insights into the participants’ fears, preferences, desires and so on: a situation that requires extra attention to avoid potential abuse by the researcher or someone else who gets access to such data. Hence, we need to pay special attention to the ethical aspects. Questions have also been raised with regard to its use for commercial and political purposes or to gain control over people. Researchers should also be aware that supposedly ‘objective’ measurements are not perfect and should be used as cues rather than stigmatising labels. Due to these ethical considerations and other factors, informed consent is always needed. In addition to an explanation of the aims and methods of a study, explicit consent should also be asked for neurophysiological assessments.
Strengths and limitations of tMM
As with every scientific method, qualitative and neurophysiological methods have their typical weaknesses and problems. On a philosophical and epistemological level, the main problem seems to arise from the fact that tMMNPD, as well as the ‘classical’ mixed methods within the social sciences, are based on two different paradigms. We cannot go into that discussion here, and refer to the exhaustive discussion on this topic by Tashakkori and Teddlie (2003) with regard to mixed methods and Brown et al. (2010), Leavy (2016) and Nicolescu (2010) with regard to transdisciplinarity. When taking a more pragmatically stance, we can mention that more and more researchers conduct mixed method studies and that these provide helpful insights (Tashakkori and Teddlie, 2003).
Also with regard to validity, it has been argued that qualitative and quantitative paradigms have their own criteria to assess the quality of studies and that concepts such as validity, generalizability and reproducibility have different meanings in the two traditions (Creswell, 2007). It is not possible simply to ‘mix’ the principles and concepts of the two. We agree with this and admit that several issues are still unresolved. However, as we have argued, a main strength of mixed method studies is that the weaknesses inherent in one method, can be compensated by making use of the other method that is assumed not to have the same weaknesses. This principle is also known as triangulation (Yeasmin and Rahman, 2012). More specifically for tMMNPD, we believe that transdisciplinary cross-validation, that is, validation with methods from different disciplines and paradigms, is one of its main strengths.
On a more practical level, we consider the lack of guidance for tMM researchers and reviewers as a major obstacle. We therefore need specific training and guidelines on how to conduct and evaluate tMM studies in analogy with the National Institutes of Health (NIH) workgroup on MM (Creswell et al., 2011).
On a more technical level, it should be mentioned that great progress has been made with regard to how these data can be collected. Until quite recently the devices to collect NPD were not user-friendly and quite complex to handle. The participant needed to be connected to an awkward and unwieldy device with many sensors and cables. Today, however, the sensors have become much more comfortable. Thanks to miniaturisation and the use of Bluetooth technology, application of sensors to the body is quite simple and participants are hardly aware of the fact that registration is going on. This enables more portable measurements, thus also in people’s natural psychosocial environments. This increases the ecological validity of such research and enables to ask more interesting research questions. For instance, for certain applications, participants only need to put on a kind of ‘wristwatch’ or a simple sensor. Even more important is the technological evolution in data processing. Most analyses are quantitative analyses (such as qEEG) performed by computers, making it possible to present real-time information in a user-friendly way with, for example, graphs or numerical indexes. A strength related to the possibility to continuously collect NPD is that tMMNPD studies may now provide a highly dynamic picture of changes over a longer period.
Issues to consider when designing or evaluating tMM
When designing or evaluating tMM, several aspects should be considered. We present only a short checklist here that may be useful when designing or evaluating tMM studies (see Box 2).
Questions to pose with regard to designing and evaluating tMM studies.*
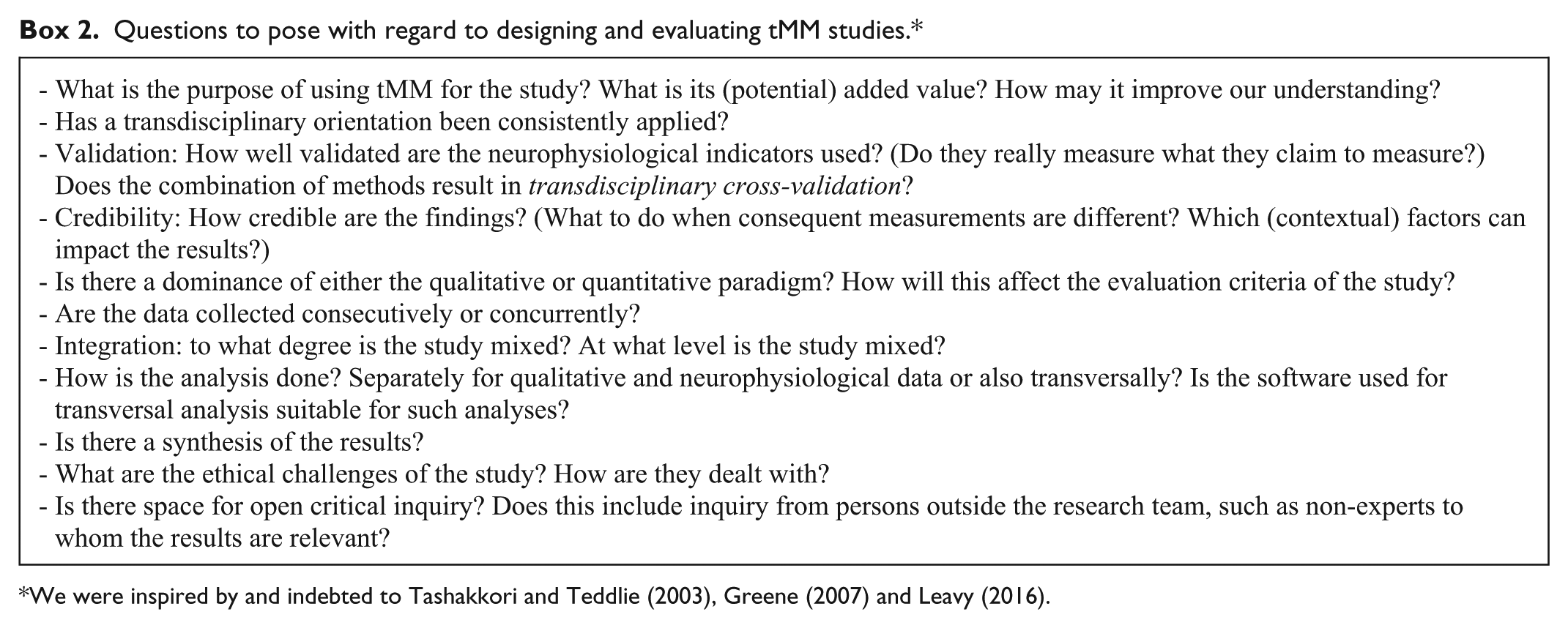
We were inspired by and indebted to Tashakkori and Teddlie (2003), Greene (2007) and Leavy (2016).
If we, by way of an illustration, apply these to our example of the COMPAS study on palliative sedation, a weak point of the study is the limited validity of the different assessment tools. However, this is also an argument in favour of opting for a tMMNPD approach since it enables transdisciplinary cross-validation. The transdisciplinarity approach has been applied throughout the study (from the problem statement and research question to the reporting). The data are collected concurrently and to ensure transversal analysis, software has been chosen in which both the qualitative data from the video observation and the NPD can be entered and analysed to achieve optimal integration. Both the qualitative and NPD are equally important and the combined use may provide new insights that cannot be obtained by the separate methods. The main decisions were made by an interdisciplinary team (including social scientists, a psychologist, a neurologist, a palliative care expert). Also stakeholders (patients and their family members, caregivers) were involved and agreed that the study was ethically challenging but warranted because there was a clear purpose and added value for the (future) patients and caregivers. If the findings based on the different methods are in line with each other, this can be considered as a validation and, hence, observational assessment as practised now, seems to be a safe and practical method. However, if the NPD contradict the observational data, the current paradigm stating that pain can be assessed by observation should be questioned and the use of more sophisticated neurophysiological assessments may be required.
Based on the above evaluation, we can conclude that the COMPAS study adheres to the main tMMNPD criteria and can therefore be considered a tMMNPD study.
We should note that there are not (always) a priori good or bad answers. Instead, these questions should be viewed as a way to become more aware of the choices that all too often remain implicit and unarticulated. Furthermore, the fact that a study cannot be considered a tMMNPD study does not imply that it is necessarily not a good study.
It usually can be considered as some kind of validation when results based on qualitative data are in line with findings based on NPD. However, discrepancy is not always a bad sign. In a tMMNPD study on neuromarketing, participants indicated that they were still in doubt as to whether or not to buy a product. On the other hand, neurological data indicated that ‘their brain’ had already made a decision (Javor et al., 2013 and Morins, 2011). Such discrepancies not necessarily reflect methodological weaknesses. On the contrary, it was only thanks to the use of a tMM approach that this remarkable process of decision-making could be revealed and that we now better understand the complexity and ambiguity of such decision-making processes.
Concluding remarks and agenda for further development of tMMNPD
tMM in which qualitative and NPD are used (tMMNPD) have the potential to improve our knowledge in many domains that are of great interest. Unfortunately, tMMNPD is scarcely used today and it has not received the attention it deserves. The main obstacle seems to be that most scientists from the natural and biomedical sciences are not familiar with the (qualitative) methods from the social sciences, and vice versa. Even worse, many look disparagingly on the others’ methodology. To end this ‘clash of paradigms’, we urgently need to learn about each other’s methodology so that all scientists are aware of the potential and limitations of the approaches typical of the social and natural sciences. To cultivate transdisciplinary thinking, a scientist trained in one of the two main paradigms (‘soft’ or ‘hard’ sciences) should at least have a basic understanding of the other paradigm. This is especially crucial for scientists working with human subjects in disciplines such as medicine, psychology and sociology.
Second, we need guidelines and training in tMMNPD so that researchers are given guidance with the theoretical, methodological and more practical aspects of how to conduct tMM studies that comply with the basic scientific standards. A critical aspect of tMM studies that needs to be addressed is the validation of the neurophysiological indicators.
Finally, we need more tMMNPD studies and researchers should be stimulated to conduct high-quality tMM studies. However, evaluation committees should also be more open to such studies and therefore their members should not only include experts from both disciplines but also experts who are able and willing to think transdisciplinary.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This work was supported by a grant (G.0566.15N) from the Flemish Fund for Scientific Research (FWO) and from the VUB (Imagica, IRP8).